
Abstract
Evidence-based practice has become somewhat of a catchphrase over the past ten years. In this paper evidence-based practice is defined and its importance for the development of the prosthetics and orthotics profession is highlighted. The authors suggest that evidence-based practice needs to be prioritized within the profession and that a cultural change needs to be initiated which supports clinicians in incorporating research findings into their daily practice. In addition, the authors highlight the need for prosthetists/orthotists to become more active in generating research rather than relying on other professional groups to contribute to their professional body of knowledge.
Introduction
The demand placed upon medical and allied health professionals to incorporate evidence into daily practice has increased substantially over the past decade. This demand is only likely to increase as reimbursement agencies are increasingly requiring clinicians to demonstrate the cost and quality of life benefits associated with the provision of orthopaedic devices (Mant 1997; Nielsen 2002). The aim of this article is to review the state of evidence-based practice (EBP) in the prosthetics and orthotics industry today and to highlight key areas that need to be addressed in order to promote EBP within the profession.
Background
While there are numerous definitions of evidence-based practice, that which is most commonly cited has been proposed by Sackett et al. (2000) and defined as the conscious and systematic use of best available research evidence in making decisions about the care of individual patients. Contemporary definitions of EBP go beyond the use of evidence as the primary decision making tool and suggest that evidence should not be used in isolation but integrated with information regarding the individual receiving treatment and the clinicians own personal experience (Doherty 2005).
In order to determine what constitutes the best available evidence for EBP, classification systems have been established and designed to give greater weight to evidence that is based on scientifically sound and rigorous research (Hill 2000; Doherty 2005). These classification systems typically rank randomized clinical trials (RCTs) and meta-analyses among the highest levels of evidence and expert opinion as the lowest. Table I presents the classification system promoted by the Centre for Evidence-based Medicine at Oxford University (2007).
Levels of evidence: Centre for Evidence-based Practice, Oxford University
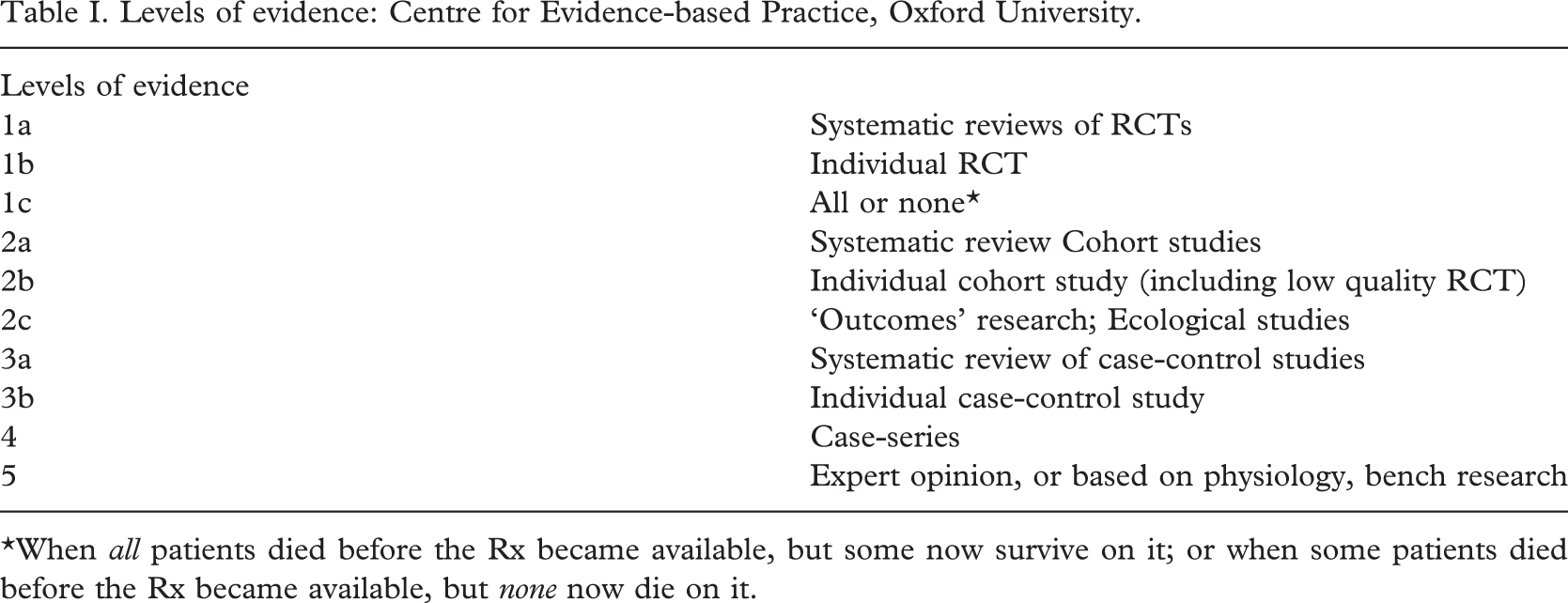
∗When all patients died before the Rx became available, but some now survive on it; or when some patients died before the Rx became available, but none now die on it.
One of the major challenges associated with EBP in the clinical environment is ensuring that clinicians have access to, and knowledge of, the best available evidence from clinical research and that they possess the skills to critically appraise it. The most effective strategy for integrating evidence into practice is to educate clinicians as lifelong, self directed learners (Banta 2003). This philosophy was developed at McMaster University in Canada (Sackett et al. 2000; Cohen 2004) but is now adopted by many other institutions throughout the world.
The development of EBP
There are several reasons for the development of EBP. The onset has often been acknowledged to epidemiologist Archie Cochrane who, among others in the 1970s, recognized a vast lack of knowledge regarding the effects of alternate treatments given to patients. He further pointed out the fact that many medical practices were based upon non-randomized data and subsequently called for significant changes in practice (Cochrane 1972). While Cochrane was among those calling for change in medical practice, the development of specific methods and indeed coining of the phrase ‘evidence-based practice’, evolved from work at McMaster University and was first described in 1992 (Guyatt et al. 1992). McMaster University has a long tradition and is a world leader in problem based learning. With this teaching philosophy as a foundation a sound methodology for EBP was developed at the University. This ‘evidence-based’ method not only provided a means by which one could scrutinize available evidence but also promoted EBP as a life long process, ensuring that treatment decisions are always based on the best current evidence and not that which was taught during ones university years or published in books.
While pushed forward by people such as Cochrane and the team at McMaster University, the development of EBP also grew out of a need to deal with the increasing volumes of information that have become available to clinicians over the past 15 years. Increasing quantities of published material within the medical and allied health professions has necessitated that clinicians develop means of systemizing the information and scrutinizing its quality in order to be able to identify and subsequently implement the findings of research that are pertinent to clinical treatment.
Criticisms of EBP
EBP is not without its critics and it would be amiss to disregard these criticisms. Buetow et al. (2006) for example eloquently turn the tides on EBP proponents in a call for empirical ‘evidence’ demonstrating that EBP produces better health outcomes. Doherty (2005) rejects this argument and presents a case to demonstrate that EBP does lead to better care.
EBP has also been criticized for promoting a top down ‘cookbook’ approach to treating patients (Strauss and McAlister 2000). Critics, from a variety of health professions suggest that the philosophy promotes categorization of patients and application of general formulae without consideration of the individual (Cohen 2004; Briggs 2005). As a result there is also a fear of ‘evidence-based policy making’ whereby access and allocation of funds for healthcare will be governed by the availability of evidence and the autonomy of clinicians to provide individual patient care will be compromised (Doherty 2005; Buetow et al. 2006).
A practical criticism of EBP is that busy clinicians simply do not have time to search and appraise clinical research. To address this issue, several attempts have been made to facilitate easy and efficient access to evidence. These include point of care wireless internet access (Leon et al. 2007), the development and dissemination of clinical practice guidelines (Boluyt et al. 2005) and online evidence databases (Bennett et al. 2006). While such attempts to improve access to evidence are certainly a step in the right direction, easy and efficient access to information still remains a significant challenge for busy clinicians.
A lack of evidence upon which to base clinical decisions is likely to be a common experience among prosthetic and orthotic practitioners and is often cited as a reason why EBP is not possible to practice. Although high level evidence may be difficult to access for many prosthetics and orthotics clinical applications, this should not be used as an excuse for not applying the principles of evidence-based practice. Clinicians are reminded that the definition of EBP refers to best available evidence. Although RCTs and meta- analyses are preferred, if they are not available the principles of EBP suggest that one should turn to the next best available evidence. This may include case reports, observational studies or even expert opinion (Doherty 2005).
Barriers in accessing evidence
There are many reasons why evidence is not being accessed for use in clinical practice beyond those that can be attributed to limited education within the subject area. Maher et al. (2004) highlight some of the major barriers as being current health policies, organizational barriers, incomplete access to the evidence and ineffective continuing education programs.
A number of authors have discussed the issue of health policies as a barrier to EBP (Barnard and Wiles 2001; Kamwendo 2002; Jette et al. 2003; Schreiber and Stern 2005). It is suggested that an emphasis on productivity, inherent in many health policies, inhibits clinicians in the time that they have available to source and critique scientific literature and to implement relative findings into their own practices. Organizational policies can also make it difficult for individual clinicians to access scientific evidence. This can be considered in light of the fact that contracts for provision of prosthetic and orthotic services have traditionally been price-based and not quality-based. Individual companies are subsequently forced to implement policies that focus on productivity and device delivery rather than promoting evidence-based care.
Clinicians working in practices that are not affiliated with teaching or research institutes often face challenges in accessing relevant scientific evidence. While there is an increasing trend towards open access journals which provide free full-text articles on-line, research evidence is rarely compiled in one place and subscription to various databases can be a costly exercise. In the ideal world clinicians would have access to online databases at the point of care. Initiatives such as the Cochrane collaboration (Cochrane Controlled Trials Register 2006) which attempts to present a review of all relevant literature in one area are a positive step towards improving accessibility of information however limited prosthetic and orthotic specific reviews are currently available via this platform.
A final barrier towards accessing evidence-based information can be attributed to inadequate continuing education programs related to evidence-based practice. It is the authors' experience that the demand for continuing education in evidence-based prosthetics and orthotics has increased substantially over the past five years. This may suggest that a change is beginning to occur within the prosthetics and orthotics profession.
Why should prosthetists and orthotists be concerned about EBP?
The principles of EBP have been well developed in many areas of medicine but to date a minimal amount of literature specific to the prosthetics and orthotics profession is available. The authors believe that it is time for change and that a primary goal of the prosthetics and orthotics profession should be well founded treatment decisions based on best evidence. Reasons for adopting the philosophy of evidence-based medicine into daily prosthetic and orthotic practice are numerous and range from the obvious clinical goal of providing one's patient with the most appropriate up-to-date treatment to the more economical goal of justifying the existence of one's services to governmental and funding authorities.
In an era where health-economists are increasingly scrutinizing medical care, the demand for improved evidence upon which to base treatment modalities will likely be crucial to the future of the profession. Expenses for healthcare have been escalating over the past decades and are expected to increase further in the decades to come (Dormont et al. 2006). This rise in cost has been attributed to numerous factors including aging and more obese populations, developments in the health technology sector, more aggressive primary preventative treatment and increasing consumer demand (Thorpe 2006). As a result of escalating costs, prioritizing of services has become a major issue in the healthcare sector. To date, priority setting within healthcare has largely been based upon vertical prioritization in which priority is established between interventions that target the same condition or use similar methods of attaining a single goal. The result is a hierarchical means of choosing between treatments options, for example, the selection of a prosthetic knee joint. It is likely, however, that the need for horizontal prioritizing will increase as governments and funding agencies prepare for rising healthcare costs. Horizontal prioritizing means that authorities will be forced to establish priorities for interventions between conditions or with quite different aims (National Health Committee 2004). This will, of course, lead to an increasing need for the prosthetic and orthotic profession to prove the efficiency of their treatment in comparison to other areas of health care. One could say that the desire to embrace all new medical technologies has, since the 1970s, been gradually replaced with growing suspicion and demand for more scientific evidence before the introduction of new health technologies into routine care (Carlsson 2004).
A further reason for the prosthetics and orthotics profession to embrace EBP is raising competition from other professional groups who are competing for markets previously held by prosthetist/orthotists (Raschke and Ford 2000). If other professions are encroaching onto the market share previously held by prosthetists and orthotists and at the same time conducting research to justify their treatments, it is obviously easier for them to attract and maintain this business.
Finally, it is important for the prosthetics and orthotics profession to consider the EBP practices of its professional peers and colleagues. A review of academic literature demonstrates that professional colleagues including medical doctors, occupational therapists and physiotherapists are all working to increase their own use of EBP stimulated by their own professional groups and certifying bodies (Cullen and Titler 2004; Coster 2005; Bennett et al. 2006; Springer et al. 2006). It is subsequently reasonable to assume that our peers and fellow members of the clinical team will come to expect and demand that prosthetists/orthotists practice from an evidence-based platform.
Prosthetics and orthotics research culture
EBP is highly dependent upon the availability and integration of clinical research in practice. The integration of research into the culture of medical and allied professionals has gradually evolved over the past two decades. Numerous factors have likely contributed to this cultural shift, including changes in health service priorities, greater demands by stakeholders, an increased need to demonstrate accountability and an increasing threat of litigation. A further major factor influencing the use of evidence in practice has also been demonstrated as the shift of education to the university sector. Universities have a long tradition of research and scholarship and an expectation that employees will contribute to the development of their respective profession through scientific exploration (Wrightson and Cross 2004). Unfortunately for the prosthetics and orthotics profession, the shift to the university sector has come later than other allied health professions (Table II). This has meant that the research culture within prosthetics and orthotics has not evolved to the extent that it has for other allied health professions and that there are currently fewer persons qualified to pursue high degrees and lead research from within the profession.
Indicating the year that students were accepted into the first degree level program in each respective country

∗Kell (2006) states that degree level education was introduced in 1992 but does not state at which university.
Given the limited number of prosthetists and orthotists with the educational background to prepare them for independent research, coupled with the relatively small size of the profession as a whole, it is not surprising that the majority of prosthetics and orthotics research has been conducted by representatives from other professional groups. To demonstrate this point the authors conducted a six-year retrospective search of all primary authors in the two major peer reviewed prosthetics and orthotics journals (Prosthetics and Orthotics International and Journal of Prosthetics and Orthotics). Results are presented in Figure 1 and indicate that on average, 12% of primary authors who published in Prosthetics and Orthotics International and 34% of primary authors who published in the Journal of Prosthetics and Orthotics held qualifications in prosthetics and orthotics. In a review of progress towards developing a physiotherapy knowledge base, Sackley (1994) highlighted the scarcity of research output and publications from physiotherapy educators citing a shortage of research experts, lack of funds, lack of time, and lack of motivation to undertake research as possible explanations. It is likely that the prosthetics and orthotics profession has fallen to a similar fate.
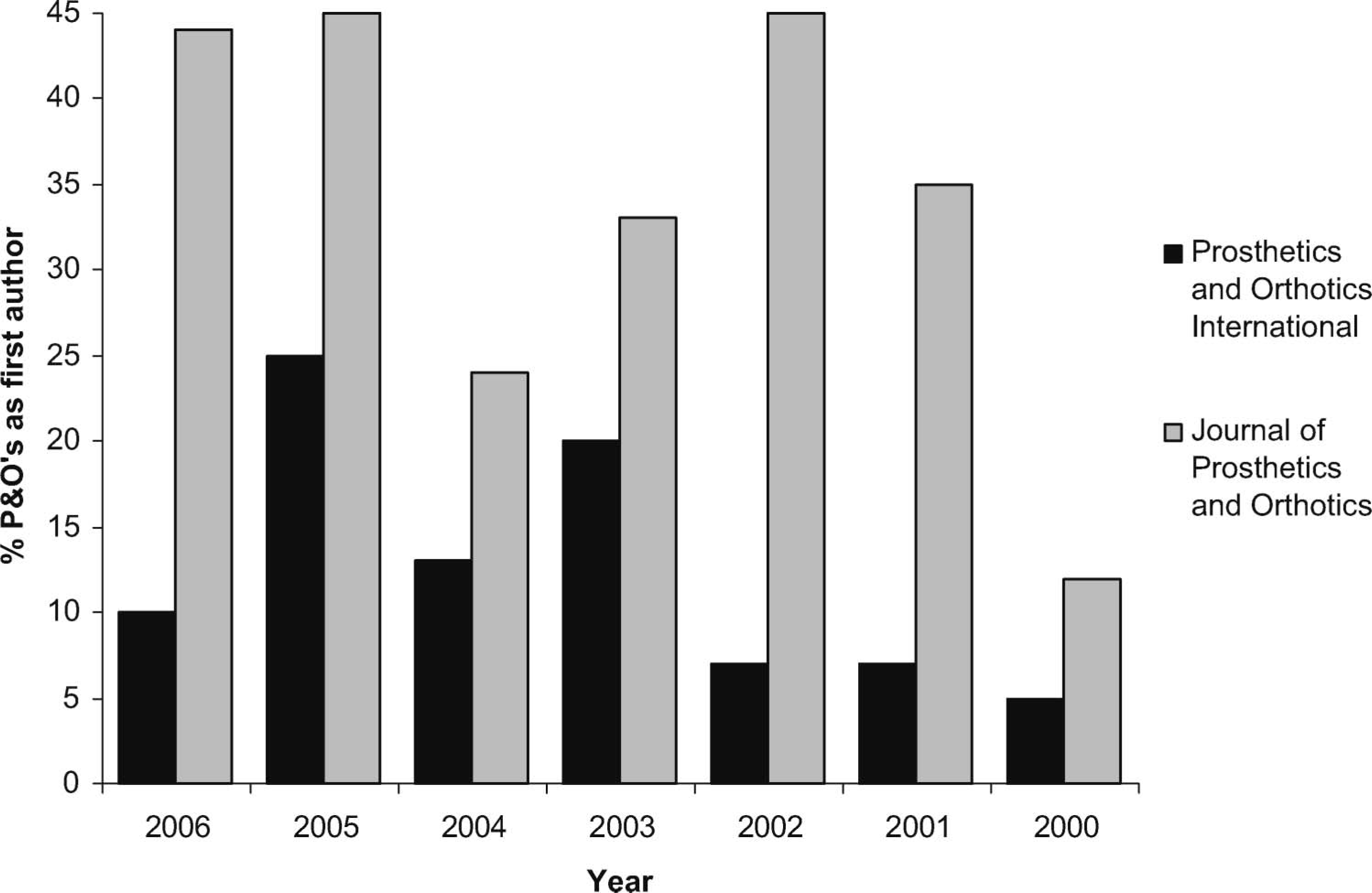
Chart showing the percentage of first authors of articles in Prosthetics and Orthotics International and the Journal of Prosthetics and Orthotics who are prosthetists/orthotists.
To gauge the volume of evidence that is available in the field of prosthetics and orthotics the authors conducted a search of the MEDLINE database using the MeSH tems ‘Artificial limbs’ and ‘Orthotic devices’. Results of this search are presented in Table III and clearly demonstrate that while research in the field of orthotics has consistently increased over the past three decades, the quantity of prosthetics research has remained relatively unchanged.
Articles listed in the Medline database that are registered under the MeSH terms ‘Artificial limbs’ and ‘Orthotic devices’. The table displays total search results for each MeSh term and also results of a search that is limited to include only randomized controlled trials (RCTs) or meta-analyses
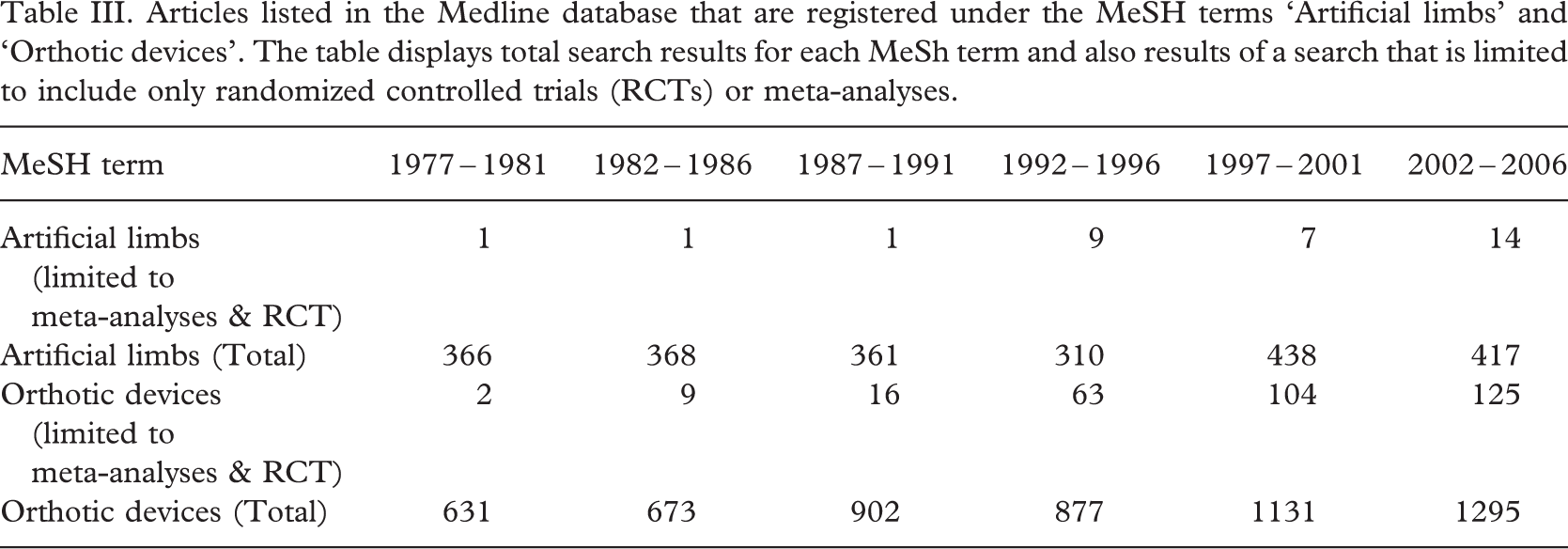
Given that RCTs and structured critical reviews or meta-analyses of RCTs are accepted as the gold standard of clinical research, the authors sought to further assess the quality of available evidence in prosthetics and orthotics by searching for research articles that employ these methods. A search of MEDLINE (1977 – 2006), and the Cochrane Controlled Trials Register (2006) for meta-analyses and randomized trials that combined one or both of the MeSH terms ‘artificial limb’ and/or ‘orthotic devices’ (exploded to include the search term ‘braces’). Results for the MEDLINE search are also presented in Table III. The Cochrane Controlled Trials Register contained one review article under the MeSH term ‘Artificial limbs’ and 15 review articles under the MeSH term ‘Orthotic devices’.
It is interesting to consider the trend in the presented data toward orthotics-related research rather than prosthetics. This is observed both in the number of publications available as a whole and in the larger number of randomized controlled trials and meta-analyses. One can only theorize as to why this is the case but reasons may include the fact that prosthetics facilities to a larger degree are private, profit-driven companies who are less likely to commit time and funds to research. It may also be due to the fact that the field of orthotics has had a larger influence from other professions (e.g., physiotherapists) who are working in the field and producing research.
What needs to be done?
In order to meet the challenges associated with integrating EBP into the prosthetics and orthotics community, steps must be taken on a number of levels. EBP has a strong link to problem-based learning and accordingly education is of great importance. Education is also considered a key factor in the integration of research and evaluation into clinical practice (Wrightson and Cross 2004). It is essential that clinical prosthetists/orthotists are confident in the integration of research results into clinical practice and that they have the ability to critically appraise the quality and relevance of these articles to a specific clinical situation. Incorporation of the principles of EBP into the education of the undergraduate students is occurring. It is important however to also address those clinicians already engaged in clinical practice. These clinicians also require education and training in EBP principles by way of postgraduate and or professional development programmes.
In the clinical setting it is necessary to have a well developed infrastructure for the dissemination of evidence-based information. Clinicians should be able to readily access the best available clinical evidence. The internet and in particular full text databases are proving useful tools in this context however even accessing these easily accessible resources may pose as a challenge to small prosthetic and orthotic facilities due to the high costs of online services. Here the national membership societies or collaboration between companies may prove particularly beneficial by developing clinical practice guidelines based on EBP principles.
It must be recognized that enhancing clinicians' knowledge and skills in EBP and generating collaborations for making evidence available will not be sufficient unless research directed at producing more evidence within the field of prosthetics and orthotics is simultaneously being conducted. This will demand a larger degree of research which is led by our own profession and answering questions pertaining to the daily treatment choices of a clinical prosthetist and orthotist. Achieving this can only be done by educating clinicians to higher levels and affording them the opportunity to investigate questions of specific clinical interest.
Conclusion
Achieving evidence-based practice should be the aim of modern healthcare. It is the authors' opinion that the prosthetics and orthotics profession has fallen behind other health professions in the evidence-based domain and that longevity of the profession will become dependent upon the ability to demonstrate evidence in practice. This will require a cultural shift on behalf of the profession and a change in the way that clinicians perceive and utilize clinical research. In 1979 Scottish epidemiologist Archie Cochrane awarded the profession of obstetrics a ‘wooden spoon’ as the medical specialty that had made the least effort to seek good evidence upon which to base its practices. It is the authors' hope that the prosthetics and orthotics profession will not be branded with a similar label and will take steps necessary to conduct quality research allowing its treatment interventions to stand the scrutiny of its patients, funding agencies and medical and allied health colleagues.