
Abstract
The objective of the study was to determine whether insoles with a low Shore A value (15°) as prescribed for patients with a diabetic neuropathy have a negative effect on posture stability because these insoles may reduce somatosensory input under the feet. It was conducted in the Center for Rehabilitation, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands The study was observational and conducted on 30 diabetic patients (aged 37 – 82 years) with a neuropathy. Posture stability (body sway) was assessed in a shoe without insole, on a flat insole with a low Shore A value (15°) and on a flat insole with a higher Shore A value (30°). These assessments were done under four different conditions: (1) eyes open, no dual-task, (2) eyes closed, no dual-task, (3) eyes open, dual-task (mental arithmetic) and (4) eyes closed, dual-task. Additionally 10 healthy controls (aged 27 – 51 years) were assessed similarly. A significantly higher root-mean-square (rms) value of the anterior-posterior velocity, Vy , was found in patients compared with controls (3.4 cm/s vs. 1.2 cm/s, p < 0.05). Also a significant difference in rms value of the anterior-posterior velocity, Vy , was found between eyes open and eyes closed (1.9 cm/s vs. 2.7 cm/s, p < 0.05). No significant effects were found for insoles or dual tasks for the total group. In diabetic patients no significant effect was found of insoles on posture stability. The effect of closed eyes on posture stability was significantly larger for diabetic patients compared to controls. It was found that prescribing insoles with a low Shore A value (15°), compared to insoles with a higher Shore A value (30°) has no significant negative effect on posture stability in patients with a diabetic neuropathy.
Introduction
Patients with a diabetic neuropathy have an impaired somatosensory input from their feet resulting in a posture stability impairment compared to diabetic patients without a diabetic neuropathy (Simmons et al. 1997; Uccioli et al. 1995; Simoneau et al. 1994). A deranged posture stability is a risk factor for falls in patients with diabetic neuropathy, independent of the co-morbidity often accompanying such a neuropathy (Richardson et al. 1992; Richardson and Hurvitz 1992; Richardson and Aston-Miller 1996; Sorock and Labiner 1992).
Patients with a diabetic neuropathy are often prescribed insoles with a low Shore A value to protect their feet against pressure ulcers. These insoles provide a redistribution of pressure between feet and insoles thereby providing cushioning and shock absorption. However, these insoles with a low Shore A value, which is less stiff, may lead to a diminished sensory input that might result in difficulties in posture stability. Posture stability may be expected to decline when patients are wearing thicker, softer and more elastic shoe soles (Robbins et al. 1992; Robbins et al.1997; Robbins et al. 1998).
Posture stability is improved, when special insoles increase sensory input, especially under circumstances where visual information is limited (Maki et al. 1999).
Wearing rigid insoles with a Shore A value of 70° during 4 weeks does not significant influence the anterior-posterior sway and the mean balance but significantly reduces the medio-lateral sway compared to not wearing insoles (Rome and Brown 2004). A significant reduction of postural sway was found when standing on magnetic insoles. This reduction in sway, when wearing magnetic insoles, was attributed to increasing blood flow and sensory changes in the foot (Suomi and Koceja 2001). Vibrating gel-based insoles, with noise system, have a positive effect on postural stability because they produce a mechanical noise and thereby create auditory feedback (Priplata et al. 2003).
No research has been performed so far into the effects of insole adaptations on posture stability in diabetic neuropathy. Because these patients often have visual limitations, which also may lead to declining posture stability, it is meaningful to measure the effects of insoles with different Shore A values on posture stability. The object of this study was to evaluate the effects of insoles with different Shore A values on posture stability in patients with a diabetic neuropathy under several measurement conditions.
Materials and methods
Subjects
Patients with diabetes mellitus and a neuropathy, aged 18 to 85 years at the time of the study, who visited the Center for Rehabilitation of the University Medical Center Groningen, were invited by means of a letter to participate in this study. Excluded were patients with ulcers on the plantar surface of the foot, with severe visual and cognitive problems and patients who were unable to stand alone without support. Visual problems were operationally defined as not being able to see a sticker (colour: white; size: 1 cm2) on the wall from 1 meter. Cognitive problems were operationally defined as not being able to understand the balance task or being able to perform the mental arithmetic.
Of the total of 79 patients who were invited to participate, 35 returned the letter and were willing to participate. Nevertheless 5 of them could not participate; because 2 developed ulcers on the plantar surface of the foot, 1 moved to another part of the country and 2 died before stability assessment. Thus finally 30 patients (30/79 = 38%), 12 women, 18 men; mean age 62.5 yr (sd = 11.3); range 37 – 82 yr with a neuropathy participated in this study. The presence of a neuropathy was determined with the Semmes Weinstein 10 gram Monofilaments and the Vibration Perception Threshold 128 Hz (Meijer et al. 2002).
The Semmes Weinstein Monofilaments were tested on the plantar surface on the hallux and central at the heel on both sides. The Vibration Perception Threshold was tested at the dorsum of the hallux on the interphalangeal joint and at the lateral malleolus on both sides. Patients were defined as having a neuropathy when the Semmes Weinstein Monofilaments were detected maximally at one place and when they felt the vibration at maximally one place.
Additionally, 10 male subjects with no disease affecting posture stability; mean age 37 yr (sd = 7.9); range 28 – 52 yr were recruited from the members of staff of the Center for Rehabilitation to act as a control group.
The assessment procedure of the controls with no disease affecting stability was similar to that of the patients. Informed consent was obtained from all the subjects before testing.
The Medical Ethical Committee of the University Medical Center Groningen approved the study.
Stability assessment
The study was performed in the Motion Analysis Laboratory of the Center for Rehabilitation. For stability assessments a force platform, Bertec type 4060 was used. x- and y- co-ordinates of the centre-of-pressure (CoP) were recorded by an A/D card and processed by custom Labview software on a personal computer. As the outcome measure for posture stability the root-mean-square (rms) value of the anterior-posterior velocity, Vy , was used (Guerts et al. 1993). The Vy data were entered in SPSS and analysed using linear mixed model analysis (fixed effects). The variables that significantly influenced Vy were analysed again in a linear mixed model analysis (fixed effects) with interaction terms. Finally patients were analysed separately for the influence on posture stability under different measurement conditions.
Measuring procedure
The participants wore standardized sandals (Figure 1). All these sandals had a hard 1 cm thick sole, with a leather lining and a heel rise of 1 cm. Different sized sandals were used during the stability assessment depending on the size of the feet of the participants. The insoles were flat and off-the-shelf. Patients were provided with the insoles and the measurements were performed.

Standardized sandal.
The patients were asked to stand in an upright position on the force plate with their arms aside their body. The position for assessment standardized as follows: heels 2.5 cm apart and feet toeing-out of 15°. The position adopted was based on the standard proposal by Snijders et al. (1975). It should be comfortable, but not too stable, as it should lead to a sufficient amount of body sway. A 15° angle between the medial foot borders is in agreement with the preferred orientation in adults (McIlroy and Maki 1997).
Patients were instructed to stand at ease during the measurement and that no arm sway or talking was permitted. The measurement period was 30 seconds. All data obtained during the measurement time were used in the analysis.
Posture stability was assessed under 3 measurement conditions; no insoles, 8 mm thick insoles with a low Shore A value (black foam, Shore A value: 15°) and 8 mm thick stiffer insoles (multiform, Shore A value: 30°).
For each measurement condition posture stability was assessed four times; (1) eyes open, no dual-task; (2) eyes closed, no dual-task; (3) eyes open, dual-task; and (4) eyes closed, dual-task. The dual-task consisted of mental arithmetic.
For all participants the first measurement condition (no insole, eyes open and no dual-task) was repeated at the end of the whole session to analyse whether participants were performing better or worse.
To reduce systematic influence of a fixed sequence of assessment conditions the first 15 patients were supplied with the insole with a lower Shore A value first and in the remaining 15 patients were given the stiffer insole first.
Results
The mean of the rms of the anterior-posterior velocity, Vy , for different measurement conditions is presented in Table I.
Mean of the root-mean-square value of the anterior-posterior velocity, V y , for patients (n = 30) and controls (n = 10) and patients only
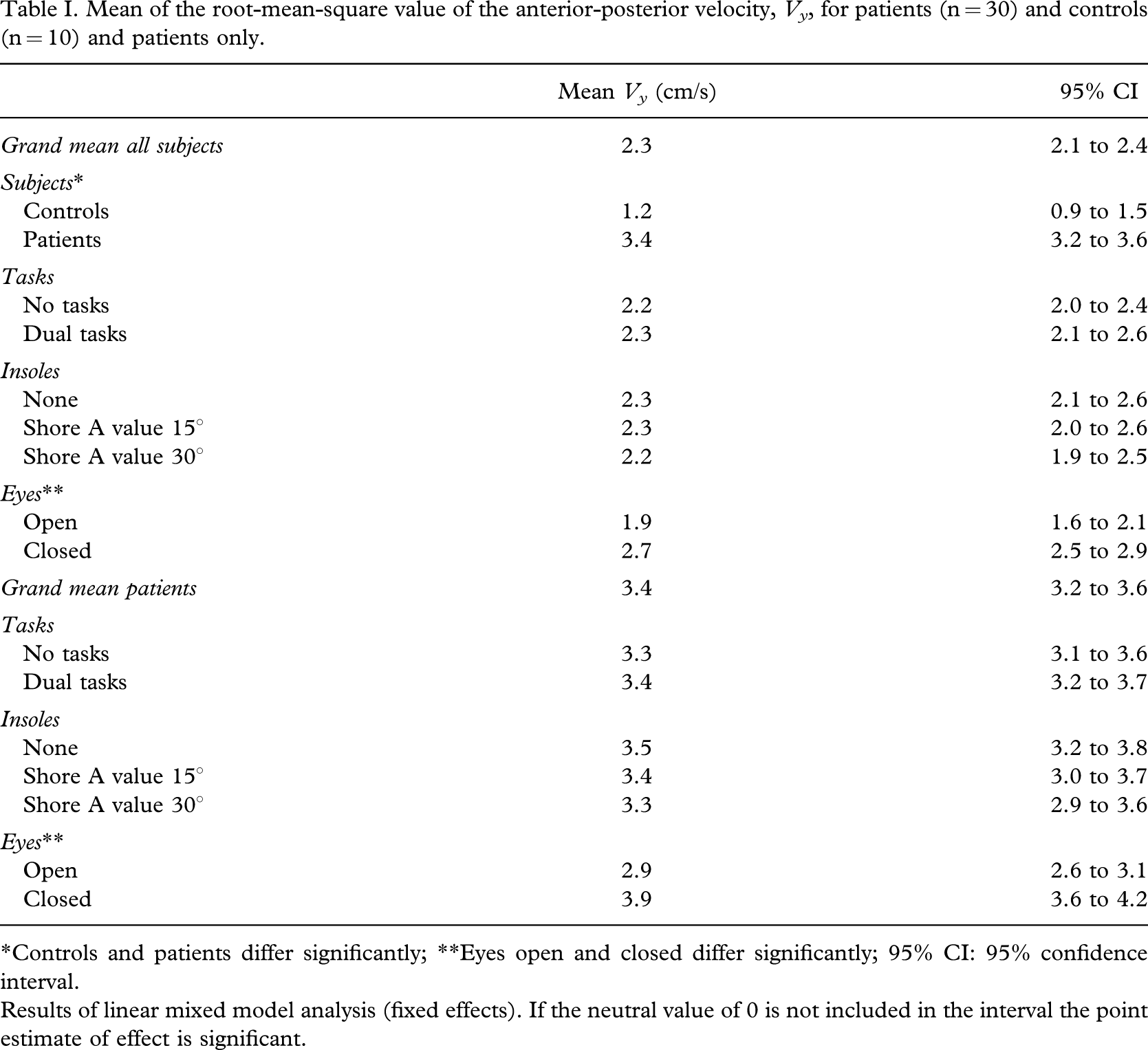
∗Controls and patients differ significantly; ∗∗Eyes open and closed differ significantly; 95% CI: 95% confidence interval.
Results of linear mixed model analysis (fixed effects). If the neutral value of 0 is not included in the interval the point estimate of effect is significant.
Diabetic patients with impaired sensory input had a significantly higher rms of the anterior-posterior velocity, Vy , compared to healthy controls. Diabetic patients and controls had both a significantly higher rms value of the Vy when they closed their eyes compared to measurement conditions with open eyes. Performing a dual-task did not significantly influence the rms value of the Vy . No significant difference between standing without insole, an insole with a low Shore A value or an insole with a higher Shore A value was found when analysing both patients and controls (Table I). In diabetic patients no significant effect was found of insoles on posture stability (Table I). The interaction term between diabetic patients and eyes open and closed was significant, indicating that the effects of closed eyes on the rms of the Vy was larger for patients compared to controls (Table II).
The estimated fixed effects of mean of the root-mean-square value of the anterior-posterior velocity, V y , for patients (n = 30) and controls (n = 10)
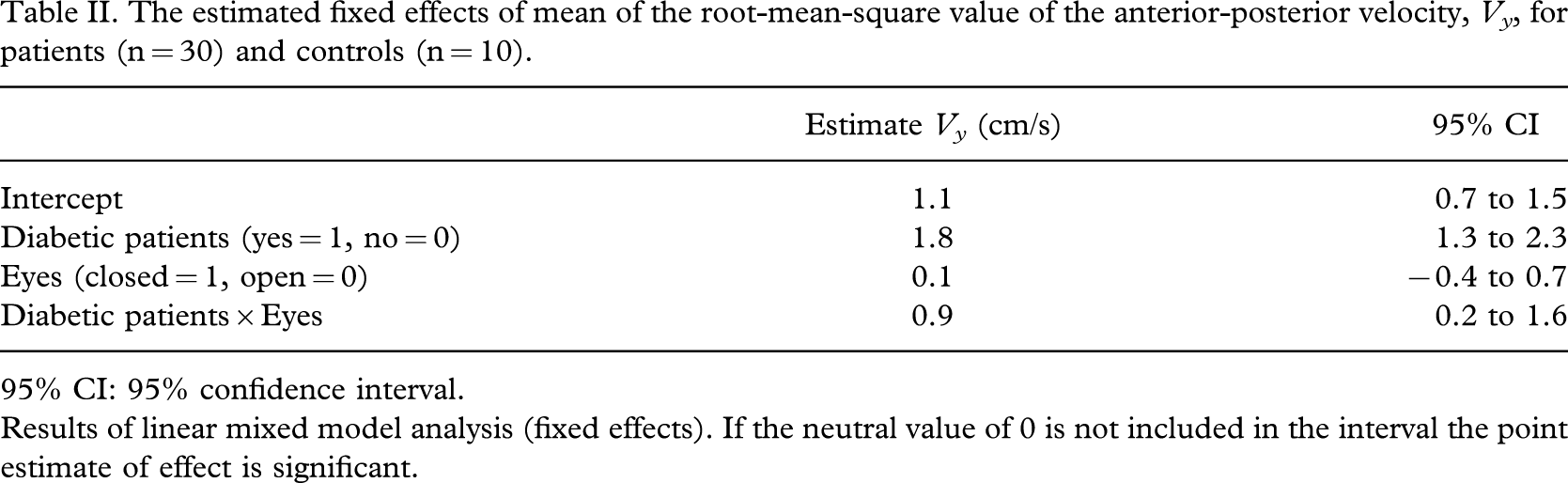
95% CI: 95% confidence interval.
Results of linear mixed model analysis (fixed effects). If the neutral value of 0 is not included in the interval the point estimate of effect is significant.
For the total group the mean of the rms value of the Vy of the first session was 2.5 (sd = 1.6) and for the last session 2.2 (sd = 1.3). The mean difference was 0.3 (sd = 1.0) (p = 0.047). For the controls the mean of the rms value of the Vy of the first session was 0.9 (sd = 0.2) and for the last session 0.8 (sd = 0.2). The mean difference was 0.08 (sd = 0.2) (p = 0.22). For the patients the mean of the rms value of the Vy of the first session was 3.0 (sd = 1.5) and for the last session 2.6 (sd = 1.2). The mean difference was 0.4 (sd = 1.1) (p = 0.062).
Discussion
In diabetic patients with impaired sensory input we found a worse posture stability compared to the healthy subjects. Diabetic patients and healthy subjects with visual deprivation had also a higher rms value of the anterior-posterior velocity, Vy , in a static situation compared to normal vision.
No effect of Shore A values of insoles on the rms value of the Vy was found. Also a dual-task did not have an effect on this velocity.
The significant decrease in rms value of the Vy the authors found for the total group between the first and last session can be explained by the assumption that participants were better focused on their posture stability at the end of the measurement, compared to the beginning of the measurements. This learning effect was independent of the sequence of insoles because 15 patients were given the insoles with a lower Shore A value first and 15 patients were given the stiffer insoles first.
This study provides evidence that prescribing insoles with a lower Shore A value on patients with a diabetic neuropathy has no negative effect on posture stability. This conclusion is based on the following: the study group existed of a representative sample of diabetic patients, the study had no missing data, the outcome variable (Vy ) predicts posture stability (Geurts et al. 1993) and no significant difference between standing on an insole with a low Shore A value and a stiffer insole, which are used in common practice, was found.
It can be argued that the sample size is too limited to detect significant differences in V y due to different Shore A values of insoles or no insoles at all. Looking at the small differences (Table I) between the insoles with different Shore A values, a very large sample size would have been needed to detect a significant difference. It is questionable whether such a difference might be of clinical relevance.
The control group existed of healthy young people because it is known that older people often have diminished vibration sense and the authors used the control group to compare the effects of the stiffness of the insoles on posture stability with people with normal sensory feedback.
In this study 8 mm thick insoles were used because thinner insoles are not effective in reducing the pressure under the foot and thicker insoles could have influenced posture stability. Additionally, this thickness is normally used in daily practise.
The patient group and the control group might also be classified as “young age” and “old age” groups respectively, but because the main effect of insoles is not significant neither for the total group nor the patient group the differences in age between the control group and patient groups is not relevant with respect to the use of insoles in diabetic patients.
A limitation of this study is that the stability was measured in a static situation. The authors would have preferred to have measured stability in a dynamic situation; however, they lacked a valid measurement instrument.
The authors used Semmes Weinstein Monofilaments (10 gram) and vibration perception threshold (128 Hz) tests because it has been proven that these tests have a high predictive value for neuropathy in diabetes (Meijer et al. 2002) and these tests are quick and easy to perform, without any harm for the patients. Therefore neuropathy was not determined by means of EMG. Although other common variables such as total sway, sway area and the maximum CoP range exist to assess posture stability, only anterior-posterior sway was assessed because it predicts posture stability best (Geurts et al. 1993). Finally the authors investigated the difference posture stability on insoles with Shore A values, which are used in common clinical practice. An insole with a Shore A value of 15° and a stiffer insole with a Shore A value of 30° were used. If insoles with lower or higher Shore A values had been chosen a significant difference in posture stability might have been found but this would have lacked clinical relevance.
Despite these limitations this study provides evidence that diabetic patients with limited sensory input from under their feet have a declined posture stability, which is in agreement with previous research results (Simmons et al. 1997; Uccioli et al. 1995; Simoneau et al. 1994; Richardson et al. 1992; Richardson and Hurvitz 1995; Richardson and Ashton-Miller 1996; Sorock and Labiner 1992; Maki et al. 1999; Geurts et al. 1993).
A significant further decline of posture stability on patients with diabetic neuropathy when visual information was limited was found, supporting evidence already described in literature (Simoneau et al. 1994; Maki et al. 1999; Giacomini et al. 1996).
Further research is necessary to investigate if posture stability is influenced by the stiffness of insoles when measured in dynamic situations and if prescribing insoles with lower Shore A values are a risk factor for falls in diabetic neuropathy.
Conclusion
Diabetic patients with limited somatosensory input, especially in circumstances without visual information have reduced postural stability. Standing on an insole with a Shore A value of 15° (compared to the stiffer insole with a Shore A value of 30°), that is used in common clinical practice, has no negative effect on postural stability.
Footnotes
Acknowledgements
The authors thank Ronald Davidsz, staff member of the Motion Analysis Laboratory of the Center for Rehabilitation, for his technical assistance. They also thank the OIM Groningen for manufacturing and providing the sandals, the insoles and for their advice.