
Abstract
This pilot study compares the effect on walking speed, in eight subjects with neuromuscular conditions, of wearing Ligaflex ankle-foot orthoses (AFO), Leafspring orthoses and shoes or with shoes alone. Range of motion, muscle strength and sensation were tested in the lower leg. Subjects underwent a standardized timed 10-m walking test five times in each of the orthoses and shoes as a measure of gait efficiency. A self-administered questionnaire was used to seek the subjects' perceptions of their functional difficulties and their opinions about the relative comfort and stability of these orthoses. Subjects had reduced ranges and strength of dorsiflexion and eversion. Some had proprioceptive deficiencies. Mean walking speed was 0.99 m/s (Leafspring) and 1.1 m/s (Ligaflex or shoes) compared to about 1.3 m/s for a normal population. Repeated measures ANOVA revealed that subjects were significantly slower in Leafspring compared to Ligaflex or to shoes. Questionnaire results rated the Leafspring as least comfortable and the Ligaflex most stable. Providing stability may be more important than assisting foot clearance when weakness is restricted to distal muscles. Further research is required to evaluate the comfort and effectiveness of orthoses to compensate for ankle instability in people with neuromuscular conditions.
Introduction
People with neuromuscular diseases present themselves with gait abnormalities due to muscle weakness which is the predominant symptom. In certain neuromuscular diseases, e.g. Charcot-Marie-Tooth disease (CMT) and other neuropathies including fascio-scapulo-humeral dystrophy (FSH) and myotonic dystrophy (MyoD) weakness of ankle dorsiflexors leads to difficulty in swing phase with foot clearance. Additionally there may be loss of active range, or contractures, and in the neuropathies diminished proprioceptive function. Ankle-foot orthoses (AFOs) that assist ankle dorsiflexion are frequently prescribed to improve foot clearance and thus reduce the frequency of falling or tripping.
There is little literature evidence about the effects of the use of orthoses in managing walking disability in people with neuromuscular diseases. Most studies on the use of AFOs have been undertaken on patients with upper motor neurone lesions, especially post-cerebrovascular accident (CVA) hemiplegia. Tyson and Thornton (2001) found that the hinged AFO significantly improved the gait of such patients. Their functional mobility, stride length, cadence and velocity improved, with users indicating that benefits outweighed any reservations about appearance. Butler et al. (1997) reported a patient post-traumatic brain injury with improvement in gait parameters following late orthotic intervention. Hesse et al. (1996) noted that stroke subjects showed improvements when walking with shoes and that there were further improvements when they used ankle-foot orthoses when compared to their barefoot walking state. Lower motor neurone (LMN) weakness is a common cause of foot-drop world wide. Heim et al. (1997) found that the lightweight carbon fibre orthosis (which is 30% lighter than a metal orthosis) could be used to preserve ambulation in people with post-poliomyelitis syndrome. The potential for improvement of gait in LMN lesions and rarer distal neuromuscular disease is iterative.
Landorf and Keenan (2000) reviewed the literature concerning the efficacy of foot orthoses. They concluded from their review that there was always difficulty in establishing the success or otherwise of orthotic therapy when results of some studies are inconclusive or negative. Their review did not include neuromuscular conditions. Alexander and Johnson (1989) describe pes cavus in CMT. They identify sequential muscle wasting in the foot intrinsics, the peronei and tibialis anterior as causes of deformity but do not suggest orthoses to compensate for muscle weakness in their case management. They prefer to address the deformity with surgical techniques specific to the individual patients' needs. CMT International UK (2000) has published a practical guide which indicates that splints may be prescribed to control foot position and thus benefit body posture and reduce the effort of walking.
At Oswestry neuromuscular clinics, recent practice has been to prescribe the Ligaflex ankle orthosis or an ‘off-the-shelf’ Leafspring ankle-foot orthosis for patients when the prescribing clinician decided that foot-drop was inhibiting foot clearance in the swing phase of gait. A literature review revealed a paucity of evidence upon which to base orthotic prescriptions for people with ankle weakness due to any neuromuscular condition. Thus this pilot study was initiated to seek user opinion about the Ligaflex (Figure 1) and Leafspring (Figure 2) splints and to measure walking speed as a simple measure of gait efficiency (Wade 1992) and thus improve understanding of the factors of importance to patients and thus direct clinical practice and further research.

A Ligaflex ankle support.

A Leafspring orthosis.
Method
The study received local ethical approval. A convenience sample of subjects was recruited from the muscle clinic and gave informed consent to participate. Inclusion criteria included a diagnosis of a neuromuscular condition, dorsiflexor weakness resulting in foot-drop (unilateral or bilateral), difficulty with controlling ankle position during walking and an age over 12 years. Subjects who were not independently ambulant were excluded.
10 metre walking tests
Each subject was assessed each using three types of support in turn, namely: (i) their own shoes: Condition A; (ii) Ligaflex with the same shoes: Condition B; and (iii) Leafspring with the same shoes: Condition C.
Ligaflex is a “universal” off-the-shelf elasticated ankle support (i.e. for left or right foot) with straps which can be applied to limit inversion and plantarflexion or eversion and plantarflexion, dependant upon the patient's own specific/presenting needs. It is available in three sizes.
The Leafspring is an AFO. The design used in this study was made from polypropylene and is available in four sizes. The Leafspring orthosis resists plantarflexion and assists the return of the plantarflexed ankle to a neutral position thus limiting foot-drop and tripping. It does not prevent the foot from pronating or supinating.
All subjects walked between two tape strips measured 10 m apart on a level carpeted floor in a hospital outpatient department. Each subject walked five times in Conditions A, B and C. The order in which each patient undertook the 10-m walk for each condition was randomized, so as to overcome order effect either fatigue or a practice effect with each subject. Each subject rested for 5 min between each set of five walks.
The time taken to walk 10 m five times for each device was measured with a stopwatch by the same investigator. All data were collected on one day for each subject. The mean times for each subject for each condition gave data for repeated measures ANOVA to determine significant differences of timed walks.
Range of movements and proprioception
Each subject was examined to determine the range of motion (measured with a goniometer) and muscle strength (MRC grades) in plantarflexion, dorsiflexion, inversion and eversion. The median MRC grade for each muscle group tested is reported. Light touch (by brushing with cotton wool), joint position sense and vibration awareness (using a tuning fork) was tested at the knee and below. Proprioception and sensory awareness were graded as normal, reduced or absent.
User opinion
Following the walking tests the subjects were asked to complete a questionnaire (Appendix). The main objectives of the questionnaire were to answer the following questions:
How comfortable the patient feels when wearing the orthoses? The subject was asked to score comfort on a scale 1 – 5 where 1 is the most comfortable and 5 the least comfortable;
How stable the patient feels when wearing the orthoses? Each subject was asked to score stability on a scale 1 – 5 where 1 is the most stable and 5 the least stable;
What mobility difficulties does the patient perceive?
Is the subject able to put the splints and shoes on unaided?
Does the subject use a splint at present and, if so, which type of splint and when is it used?
Does the splint help or hinder activity?
Results
Subjects
The nine subjects, (five men and four women) included one patient with limb girdle muscular dystrophy (LMD), four CMT patients, one FSH patient, one MyoD patient and one patient with hypobetalipoproteinaemia suffering a peripheral axonal neuropathy. One male patient with CMT (subject 5) used a different style of orthosis on a regular basis so his results have not been included in this report. The subject's age range was 14 – 63 years (mean 34.5 years).
Clinical examination
Clinical examination revealed that all subjects had some limitation of range of dorsiflexion and reduced strength in the ankle dorsiflexor musculature (median MRC grade 4). Plantarflexor range and power was relatively well preserved. Range was altered, but power was reduced in the invertor muscle group at median MRC grade 4 but more reduced in the evertors at R median MRC grade 4 and L median MRC grade 3. Proprioceptive testing showed that one subject was normal, four subjects were affected at knee level, two subjects were affected bilaterally and two subjects were affected unilaterally. At the ankle level a further two subjects affected bilaterally. At the great toe only three subjects were unaffected by proprioceptive loss.
Walking velocity
Subjects tended to walk more slowly than the walking velocity of normal subjects reported by Findley and Cody (1970) (1.37 m/s ± 0.22 males and 1.23 m/s ± 0.19 females). Subject 4 walked more slowly than the other subjects recording a mean velocity in shoes of 0.4 m/s, Ligaflex 0.59 m/s and Leafspring 0.43 m/s. The results for remaining seven subjects gave mean values in shoes only 1.14 m/s, with Ligaflex 1.12 m/s and with Leafspring 0.99 m/s.
Table I shows the mean time taken to walk 10 m for each subject in each of the three conditions. With the exception of subject 4 who walked slowest in shoes, the subjects walked slowest when wearing a Leafspring orthosis and shoes.
Mean times for each subject in each condition.
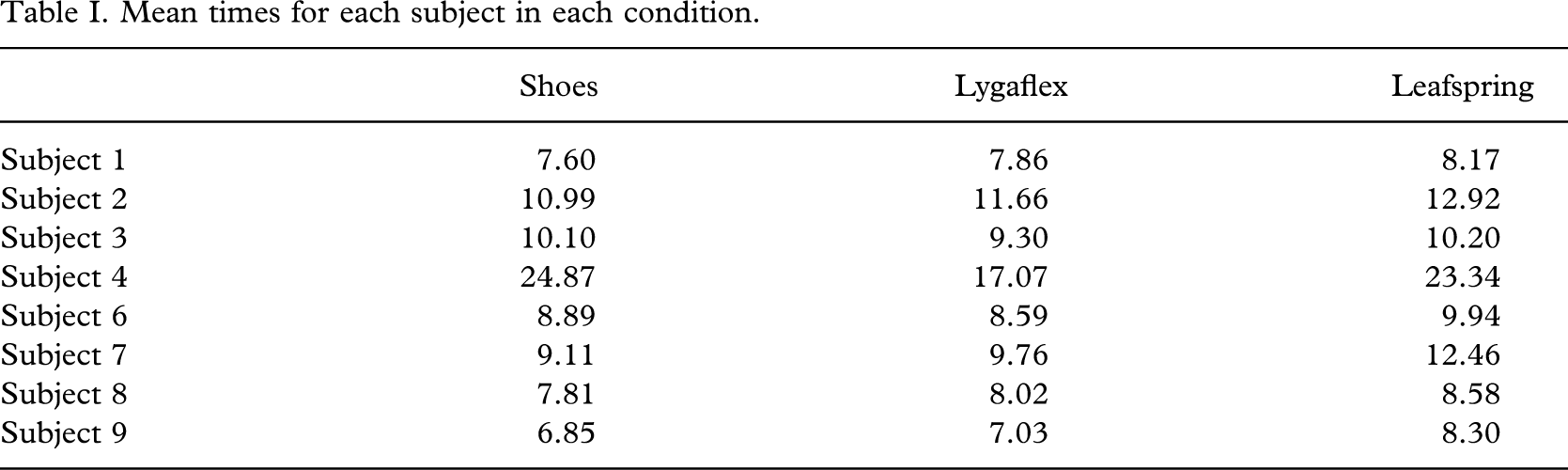
The Ligaflex and shoes produced shorter walking times than the Leafspring and shoes. In seven out of eight instances the Leafspring produced the longest walk times. The walk times for Ligaflex and shoes produced similar walk times with respect to each other. Four subjects walked faster in shoes, three faster in Ligaflex and one achieved the same speed in shoes and Ligaflex.
A repeated measure ANOVA was performed using SPSS 11. When α = 0.05 there is a significant difference between mean walking speeds in Ligaflex and shoes and Leafspring orthoses but not between shoes only and Ligaflex and shoes or shoes only and shoes and Leafspring orthoses. When α = 0.1 there is also significant difference between mean walking speeds in between shoes only and shoes and Leafspring orthoses but not between shoes only and Ligaflex and shoes.
Questionnaire findings
All subjects admitted to walking difficulties; six tripped, five fell, seven had difficulty with slopes and stairs, four found windy conditions difficult and five found walking tiring. Subject 2 had no orthoses; subject 4 had a Leafspring orthoses whilst the remaining six subjects had Ligaflex orthoses. Three subjects were unable to apply the Leafspring and another subject was unable to apply the Ligaflex.
User opinion
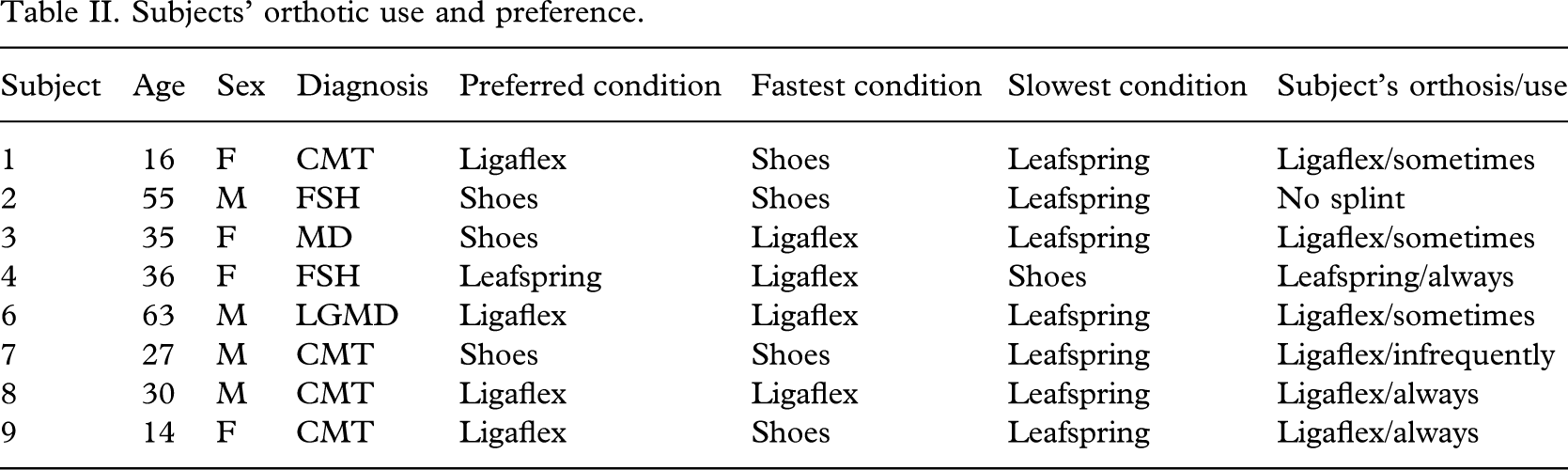
In Table II the subjects' preference for walking in shoes only or with splints is indicated; four subjects preferred the condition which permits fastest walking, two preferred their shoes when there was no significant difference between walking speed in shoes or Ligaflex. Just one subject preferred shoes when walking in a Ligaflex was significantly faster. For the CMT subjects, three preferred Ligaflex and one shoes: the latter could walk significantly faster in shoes alone whereas for those subjects preferring Ligaflex there was no significant difference between their speeds in shoes with or without Ligaflex. Three subjects sometimes, two always and one infrequently used their Ligaflex outdoors. Subject 4 had a Leafspring orthosis that was always used out of doors. Two subjects found that their orthoses hindered them on slopes and stairs. One subject reported hindrance with standing but all were subjectively helped with walking in their orthoses.
Subjects' orthotic use and preference.
In Table III, it is apparent that five subjects found just shoes most comfortable, whilst seven subjects using the Ligaflex found it most stable. With the exception of subject 4, all found the Leafspring the most uncomfortable and the least stable.
Subjective comfort and stability.
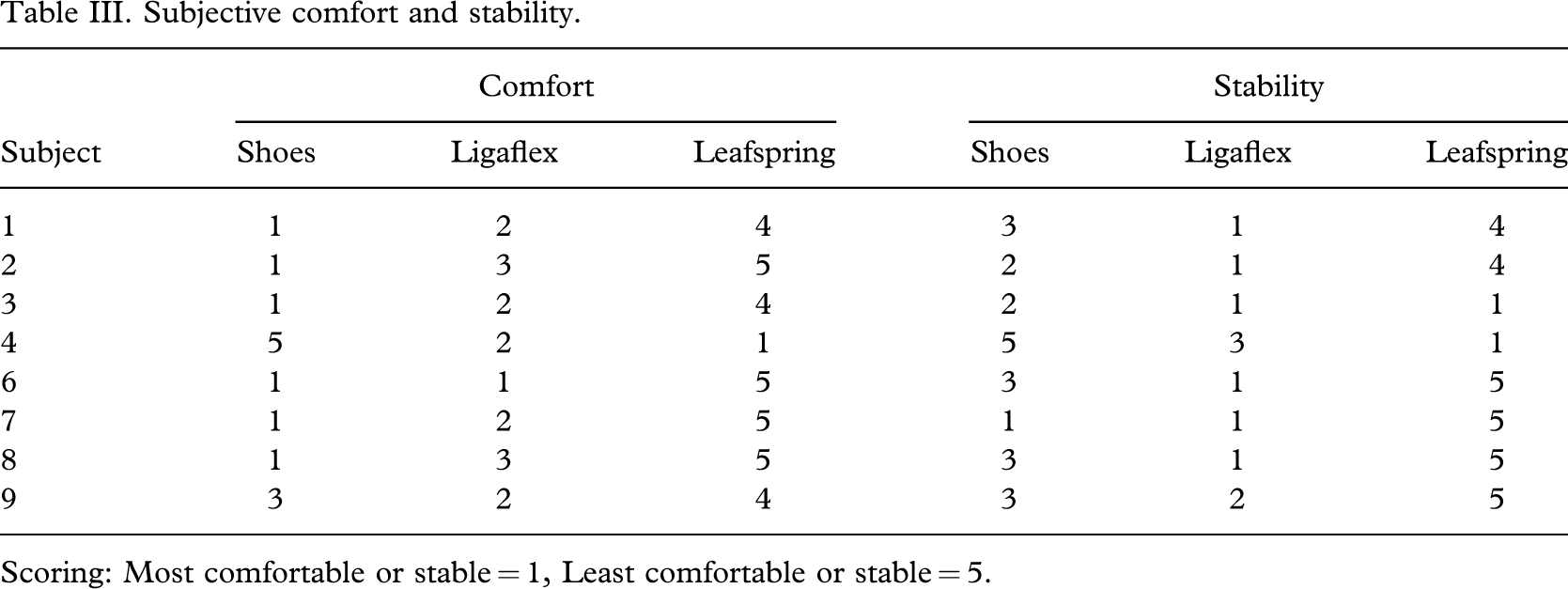
Scoring: Most comfortable or stable = 1, Least comfortable or stable = 5.
Discussion
Walking speed was adversely affected when wearing the Leafspring for all the subjects who were unfamiliar with this splint. There appears to be tendency to prefer splints/or shoes that do not adversely affect walking speed.
Familiarity with either Ligaflex or Leafspring may have been a biasing factor in the subjects' preference but despite his preference for his Leafspring, the Leafspring user actually walked quickest in the Ligaflex.
Previous studies discussed the difficulties that arise due to uncomfortable ill-fitting splints including “off-the-shelf” AFOs but it was noted that subjects found bespoke hinged AFOs comfortable (Tyson and Thornton 2001). In this study the ‘off-the-shelf’ Leafspring was rated the least comfortable but the range of sizes and elasticity of the Ligaflex produce a relatively comfortable support which could be worn inside the users' footwear. This may contribute to the acceptability and utility of the Ligaflex.
At the start of this study the plantarflexed foot position in swing phase was thought by clinicians to be the main cause of gait tripping. Subjects are, however, able to compensate for distal weakness causing foot drop by increased flexion of swing limb hip and knee. The subjects found the Ligaflex more stable probably because it supports the ankle in the medio-lateral plane in the presence of weak evertors. This leads us to suppose that users find the stance phase ankle support helpful. It limits trips and falls as it stabilizes the ankle thus contributing to the control of the multi-segment linkage of the lower limbs so enabling ground clearance with the opposite swing limb foot. Thus the dorsiflexion assist in swing phase may be of less importance than providing stance phase stability.
If it is accepted that compensation for dorsiflexor and evertor weakness is of importance, this might be more effectively provided with intimate fit and support by custom fabricated braces. This could take the form of a Lycra sock or of hinged AFO incorporating an adjustable dorsiflexion assistive spring. The benefits of such an individualized prescription would need to be considered in relation to the ‘costs’ of the device both in terms of item price, and time taken to and ease of fitting the device. There may also be differences on the durability of elasticated and polypropylene orthoses. Size, skin condition, oedema or poor circulation may affect the choice of orthosis.
The Ligaflex is as an active splint, the elastic straps assisting weakened muscle action with proprioceptive input enhanced by compression facilitating positional awareness. The type of orthosis and timing of introduction should be considered as a proactive rather than reactive measure, introducing the Ligaflex as part of the rehabilitation process after any ankle injury, even mild to reduce tripping.
Conclusion
The ‘off-the-shelf’ Leafspring AFO was poorly tolerated as it proved uncomfortable and slowed walking. The Ligaflex elastic orthosis was however well tolerated and was perceived to improve stability without adversely affecting patient walking speed.
Orthoses will be underused when they are uncomfortable and thus the patient will derive little if any benefit from the device itself. Optimal effectiveness will be lost. Although subjects did not find the Ligaflex as comfortable as their own shoes they did report using the Ligaflex.
During this study the issue of stance phase stability emerges so that future studies should attempt to observe and measure frontal plane motion. This information could be useful to determine the importance or otherwise of enhancing mediolateral orthotic control in future orthotic designs.
Clearly this small study was undertaken with few subjects but has provided some useful insights into the orthotic users' perspective. It was unexpected that the Ligaflex would be deemed more stable and the Leafspring AFO prove so uncomfortable. Foot stability and comfort need to be enhanced by future development and research. Nevertheless, the evidence presented in this short study suggests that the Ligaflex is a useful device to assist subjects with dorsiflexor and evertor weakness due to neuromuscular disorders.
Footnotes
Acknowledgements
The authors thank all nine subjects involved in this study, without whom the testing of the orthoses could not have been undertaken.
None of the authors has had or presently obtains any benefit in kind or remuneration from any of the orthosis manufacturers or distributors.
Appendix
Splinting preference questionnaire
This questionnaire is to help us to understand the factors which are important to you in the use of ankle splints.
What do you find is the main problem with walking.
Please circle your answer
Do you use a splint at present?
If yes, please tick which type of splint it is
When do you use this splint?
Please circle your answer
Are there activities which are helped or hindered by using your splint?
Please tick the appropriate column
What factors influence your decision when to wear your splint?
During the walking you have done today you have used 2 types of splint and just your shoes.
Which did you find most comfortable?
Please score 1 for most comfortable and 5 for least comfortable
Which did you find most stable?
Please score 1 for most stable and 5 for least stable
Which could you put on yourself?
Please circle your answer
You have walked in your
If there are any other factors about using splints which are important to you please indicate below.
Thank you for completing this questionnaire.