
Abstract
Our understanding of how partial foot prostheses function stems from static force analyses, where assumptions about the location of the ground reaction force during terminal stance have been made. While such assumptions seemed reasonably based on an understanding of normal gait, they are often illogical based on what is observed clinically. As such, the aim of this work was to evaluate the belief that partial foot prostheses are able to restore the effective foot length. Centre of pressure (CoP) excursion data were collected as part of a complete gait analysis incorporating an Advanced Mechanical Technology Inc. force platform. The CoP excursion patterns, observed in a cohort of eight partial foot amputees and matched control subjects, highlight the inability of toe fillers and slipper sockets to restore the ‘effective’ foot length in transmetatarsal and Lisfranc amputees, whereas clamshell prostheses fitted to the Chopart amputees were able to restore the effective foot length. In the transmetatarsal and Lisfranc amputees, the observed CoP excursion patterns could indicate a learned gait strategy necessary to reduce the requirement of the weak triceps surae musculature as well as spare the sensitive distal stump from extreme forces. The toe fillers and slipper sockets fitted to these amputees may not be stiff enough to support the amputee's body weight or the device may not be designed appropriately to assist the weakened triceps musculature to resist the external moments caused by loading the forefoot. The clamshell prostheses restored the ‘effective’ foot length due to the rigid toe lever and clamshell socket, which could allow and comfortably support the generation of substantial external moments during terminal stance.
Introduction
Our understanding of partial foot amputee gait and prosthetic fitting has been underpinned by static force analysis theories (Condie 1970; Mueller and Sinacore 1994; Stills 1987; Weber 1991), whereby authors have speculated about the effects of amputation and prosthetic fitting based on an appreciation of normal, non-amputee gait. While these static force analyses provide relatively simple insights into the function of the partial foot amputee and prosthetic replacement, their accuracy is based on what is known about the forces in the analysis.
Characteristics of forces depicted in these static force analyses, such as the magnitude or point of application of the ground reaction force (GRF), have not been measured. Without these data, assumptions about these parameters must be made. While it may be reasonable to assume that the magnitude of the GRF remains unchanged following partial foot amputation, other assumptions, such as the point of application of the GRF acts somewhere near the ball of the foot during terminal stance (Condie 1970; Mueller and Sinacore 1994; Stills 1987; Weber 1991), seem less convincing.
By assuming that the point of application of the GRF is near where the metatarsal heads would have been during terminal stance, as it is in normal gait, authors are unwittingly making a number of assumptions about how partial foot amputees walk and how prostheses function. For example, authors must have assumed that the prosthesis or orthosis can restore the lost foot length or toe lever such that the amputee can actually load it. This means that the peak GRF experienced during terminal stance can be applied to the prosthesis, around the area where the metatarsal heads ought to be. If this were the case, then the external torques developed about the ankle would be comparable to normal gait; assuming the magnitude of the GRF remains comparable to normal. For the amputees to walk in this way, there must exist a reasonable coupling between the stump and prosthesis—almost a rigid link, whereby the torques caused by loading the toe lever could be comfortably transmitted to the stump. The calf musculature must also be strong enough to moderate the external ankle moment, or in cases of muscle weakness the prosthesis needs to be able to produce this moment.
However, what is typically seen clinically is that the stump rotates within the shoe/prosthesis and is not a rigid coupling. Most partial foot prostheses do not have a socket or a large contact area with the stump, so how can the forces caused by loading to toe lever be transferred to the stump comfortably? Most devices fitted to partial foot amputees do not incorporate a stiff toe lever, so there is no way that GRF can progress to the prosthetic forefoot without the device collapsing under the amputee's body mass. Significant atrophy of the triceps surae musculature, characteristic of disuse atrophy, is often observed in this population, which may be indicative of an inability to moderate large external ankle moments let alone produce sufficient concentric activity to drive the foot into plantarflexion. This may, at least in part, explain the limited plantarflexion observed during gait.
While static force analyses allow many of the problems of partial foot amputee gait and prosthetic function to be easily understood, they are based on assumptions that are not supported by clinical observation. Despite obvious problems with these force analyses, they have perpetuated an understanding of how partial foot amputees walk and prostheses function which is based on an understanding of normal gait; leading to the longstanding perception within the literature that partial foot prostheses are able to replace the lost foot length (Condie 1970; Mueller and Sinacore 1994; Pullen 1987; Rubin 1984; Stills 1987; Weber 1991; Sanders 1997; Sobel 2000), which seems unreasonable.
As such, the aim of this work was to evaluate the belief that partial foot prostheses are able to restore the ‘effective’ foot length.
Method
Cohorts of eight partial foot amputees and eight normal, non-amputee (control) subjects were recruited. Participants provided informed consent as required by the University Human Research Ethics Committee of the Queensland University of Technology. Minimal exclusion criteria were applied to the amputee sample due to the limited number of subjects available, and as such, the amputee cohort was quite variable in terms of amputation level, years since amputation, number of limbs affected, and types of prosthetic fitting (Table I). Subjects were excluded if they ambulated with the use of any gait aids, had concomitant health problems, such as ulceration, or had neuromuscular/musculoskeletal conditions that might affect their gait.
Characteristics of the amputee subjects.
Bi: bilateral; Uni: unilateral; SD: standard deviation; MTP: Metatarsophalangeal; TMT: Transmetatarsal.
Gangrene secondary to frostbite.
Gangrene secondary to water burns.
The gait of each amputee subject was considered relative to the normal, non-amputee cohort. In this way, the gait of any amputee subject could be compared with the mean and 95% confidence interval of a normal population rather than to the idiosyncratic pattern of locomotion of a single control subject with similar anthropometric characteristics. The mean age, stature, and mass of the control sample, including standard deviations in parentheses, were 41.13 years (±14.81), 1.74 m (±0.08) and 77.11 kg (±6.83), respectively. Comparable data for the amputee cohort have been presented in Table I.
The gait of amputee subjects was evaluated while wearing their current prosthetic replacement (Table I). No prostheses were fabricated especially for this investigation. Both amputee and control subjects walked along a level 10 m walkway at their self-selected walking speed until seven trials were obtained for each lower limb.
Centre of pressure (CoP) excursion data were collected as part of a complete gait analysis using a Peak 3D motion analysis system (Peak Performance Technologies. Englewood, CO) and an AMTI force platform (Advanced Mechanical Technology Inc. Waterton, MA). Force platform data were sampled at 1000 Hz with subsequent data processing done using custom derived Matlab software (Mathsworks Inc., Englewood Cliffs, NJ). Externally measured force data were filtered using a zero lag, fourth-order Butterworth digital filter with a 125 Hz cutoff frequency and accounted for differences from absolute zero due to errors associated with balancing the bridge excitation voltage (Dillon 2001). Data were then sub-sampled to match the kinematic sampling rate of 50 Hz. Instances of initial contact and toe-off were determined using a 10 N threshold criterion based on the changing magnitude of the vertical GRF (Dillon 2001). CoP excursion data were normalized by shoe length, and GRF data were normalized by body mass. For all subjects, data obtained from multiple trials were averaged for each limb.
Results
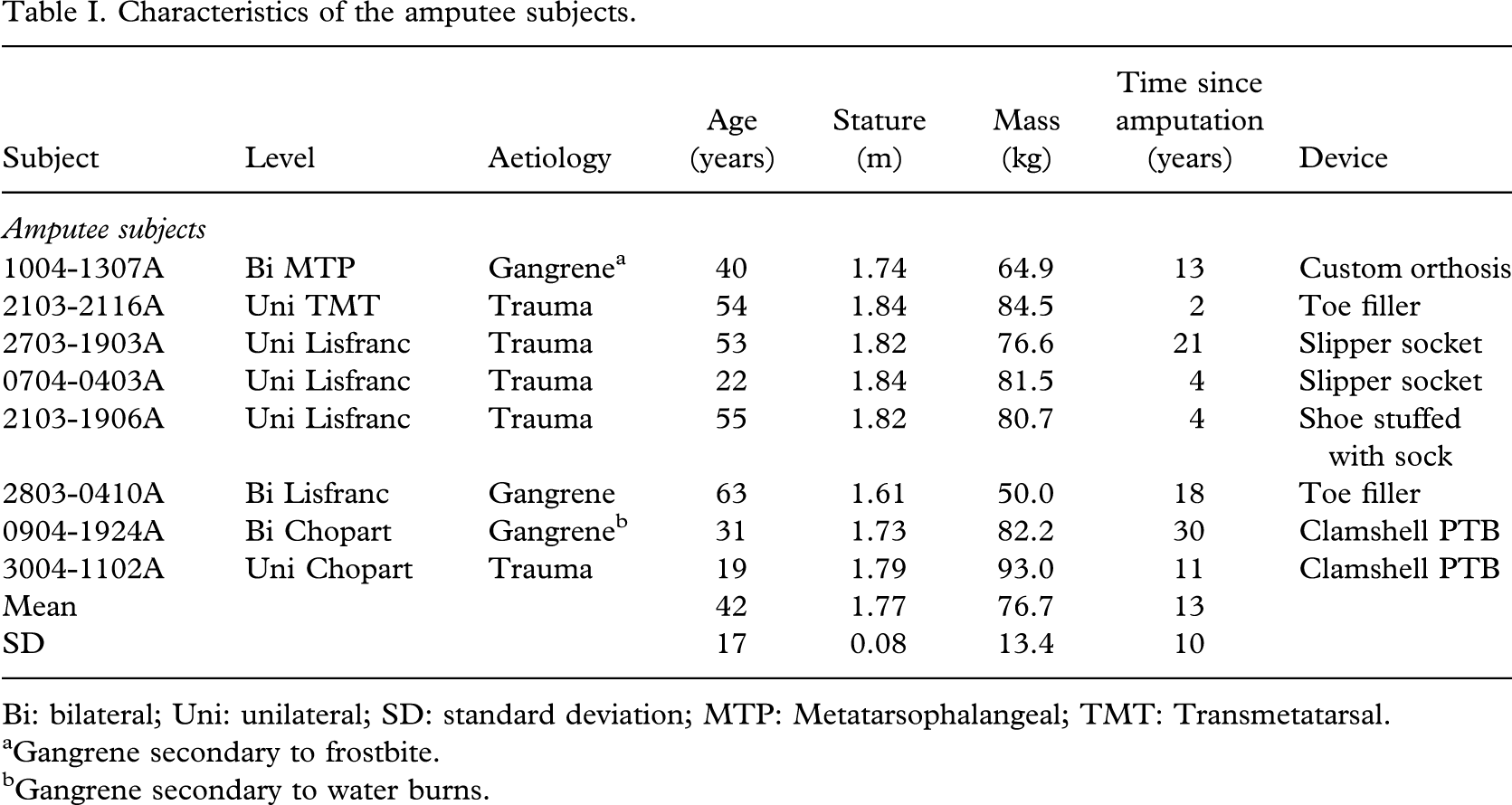
In the metatarsophalangeal (MTP) amputee, the CoP progressed relatively normally along the length of the remnant foot during the initial portion of stance phase (Figure 1). Following loading response, the CoP did not move as distal along the length of the foot as typically observed in the normal population (Figure 1). This was the same pattern observed in the transmetratarsal (TMT) and Lisfranc amputees, only more pronounced (Figure 2).
Centre of pressure excursion for the affected limbs of the metatarsophalangeal amputee. CHC: contralateral heel contact; CoP: centre of pressure expressed as a proportion of shoe length (SL); the distal end of the stump is located at approximately 78% of shoe length.
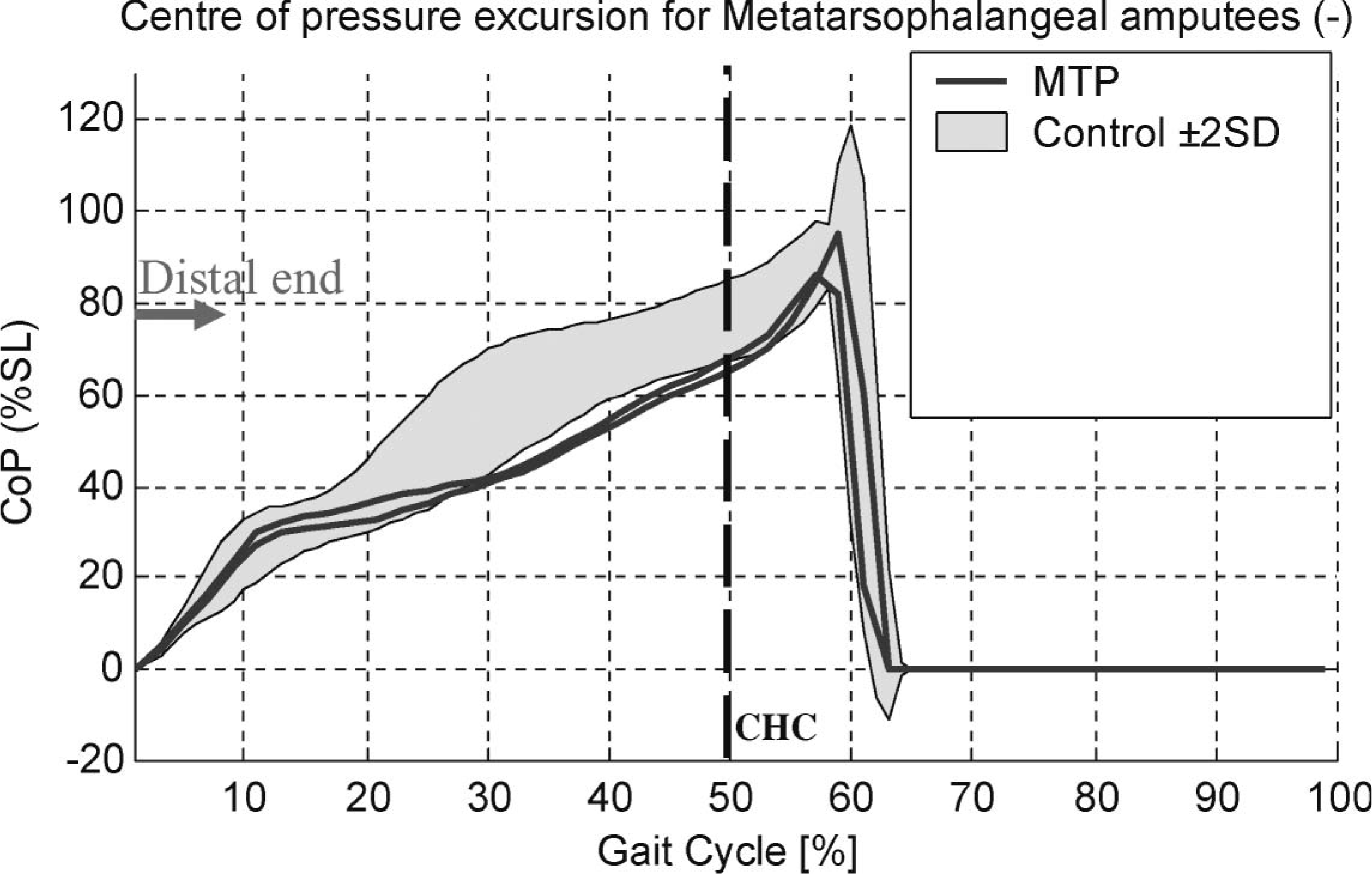
Centre of pressure excursion for the affected limbs of the transmetatarsal and Lisfranc amputees. CHC: contralateral heel contact; CoP: centre of pressure expressed as a proportion of shoe length; the distal end of the stump is located between 58 and 65% of shoe length depending on the length of the metatarsals left intact.
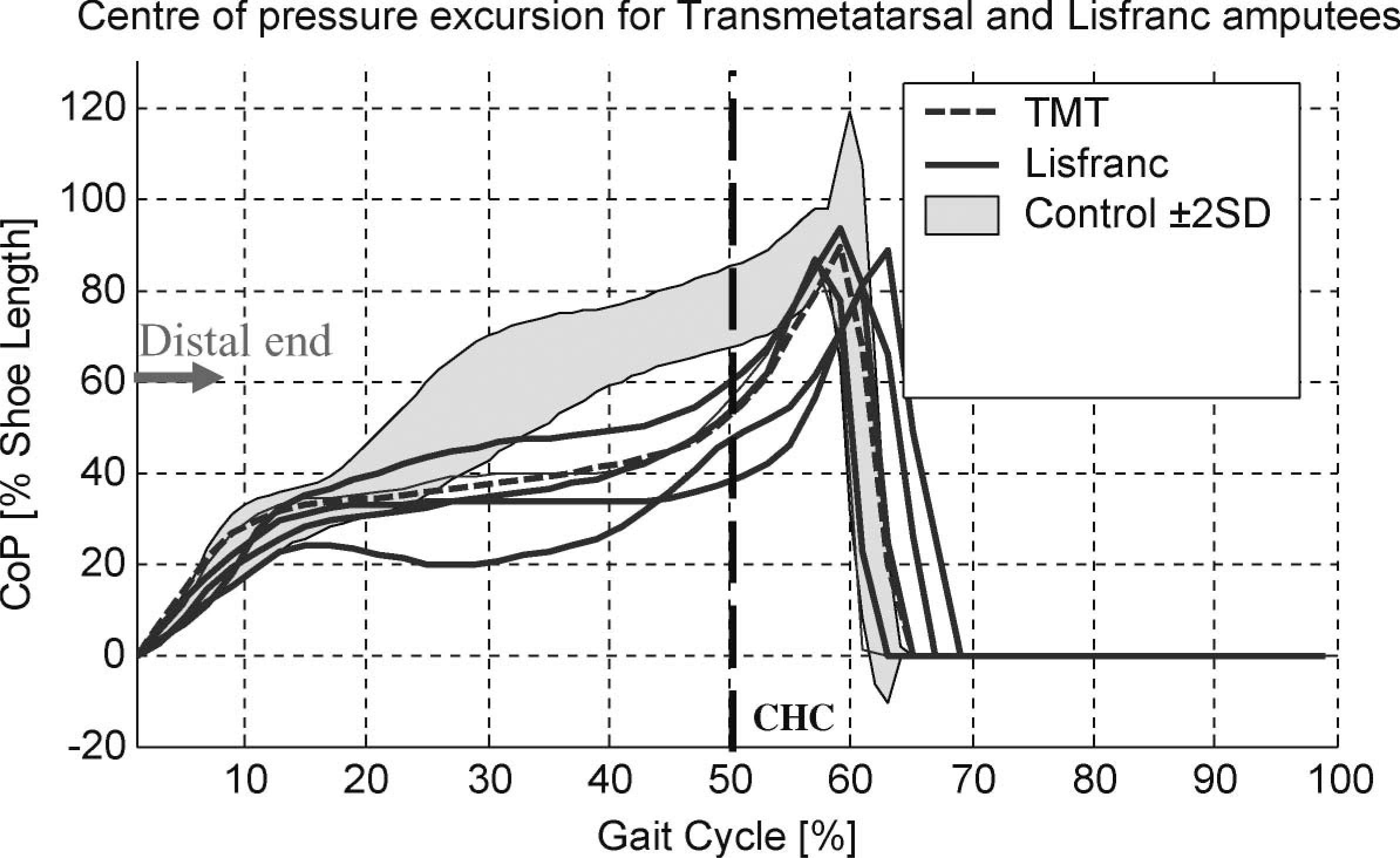
Once the metatarsal heads had been amputated, dramatic changes in the progression of the centre of pressure were evident following loading response, where the GRF did not continue to progress distally along the length of the residuum but remained well behind the distal end throughout most of stance phase (Figure 2). In the TMT and Lisfranc amputees, the distal end of the stump was located at 58 – 65% of shoe length, depending on the length of the remnant metatarsals. At about 45% of the gait cycle when the largest vertical GRF occurred during the later half of the stance phase (Figure 3), the CoP was located well behind the end of the stump and did not progress past its distal end until after contralateral heel contact (CHC) when body weight was shared between both limbs in double support (Figure 2). The CoP did extend the entire length of the shoe; however, when the CoP was located distal to the end of the stump, within the prosthetic forefoot (Figure 2), the magnitude of the GRF was relatively small and rapidly declining (Figure 3).
Vertical ground reaction force for the affected limbs of the transmetatarsal and Lisfranc amputees. Fz: vertical ground reaction force normalized by body mass. CHC: contralateral heel contact.
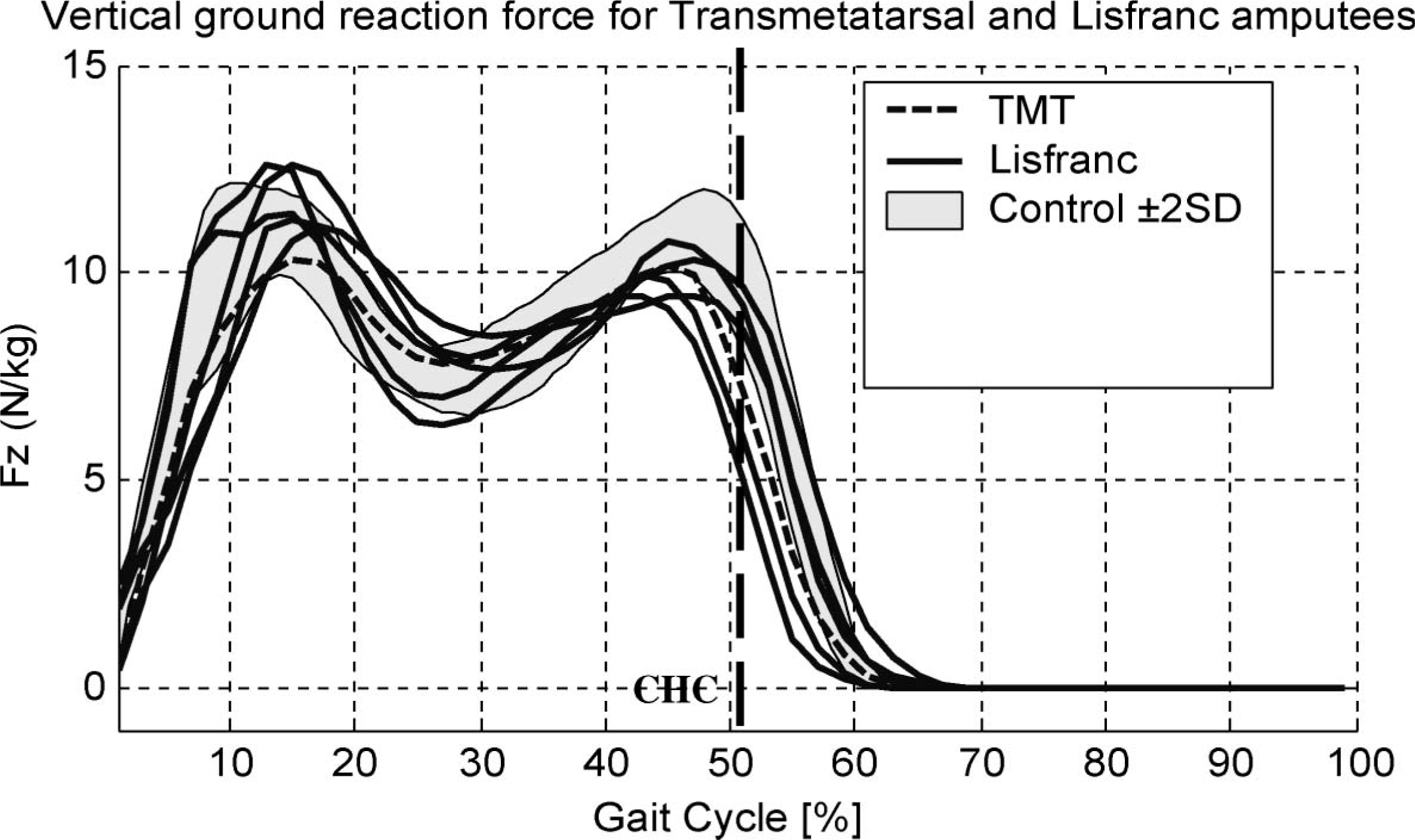
In the Chopart amputees, the CoP was able to progress well beyond the distal end of the stump, at 40% shoe length (Figure 4), commensurate with the second peak of the vertical GRF which occurred at 45% of the gait cycle (Dillon 2001). In this way, the amputees were able to apply a substantial load to the prosthetic forefoot during terminal stance in a manner much more akin to that observed in the normal population.
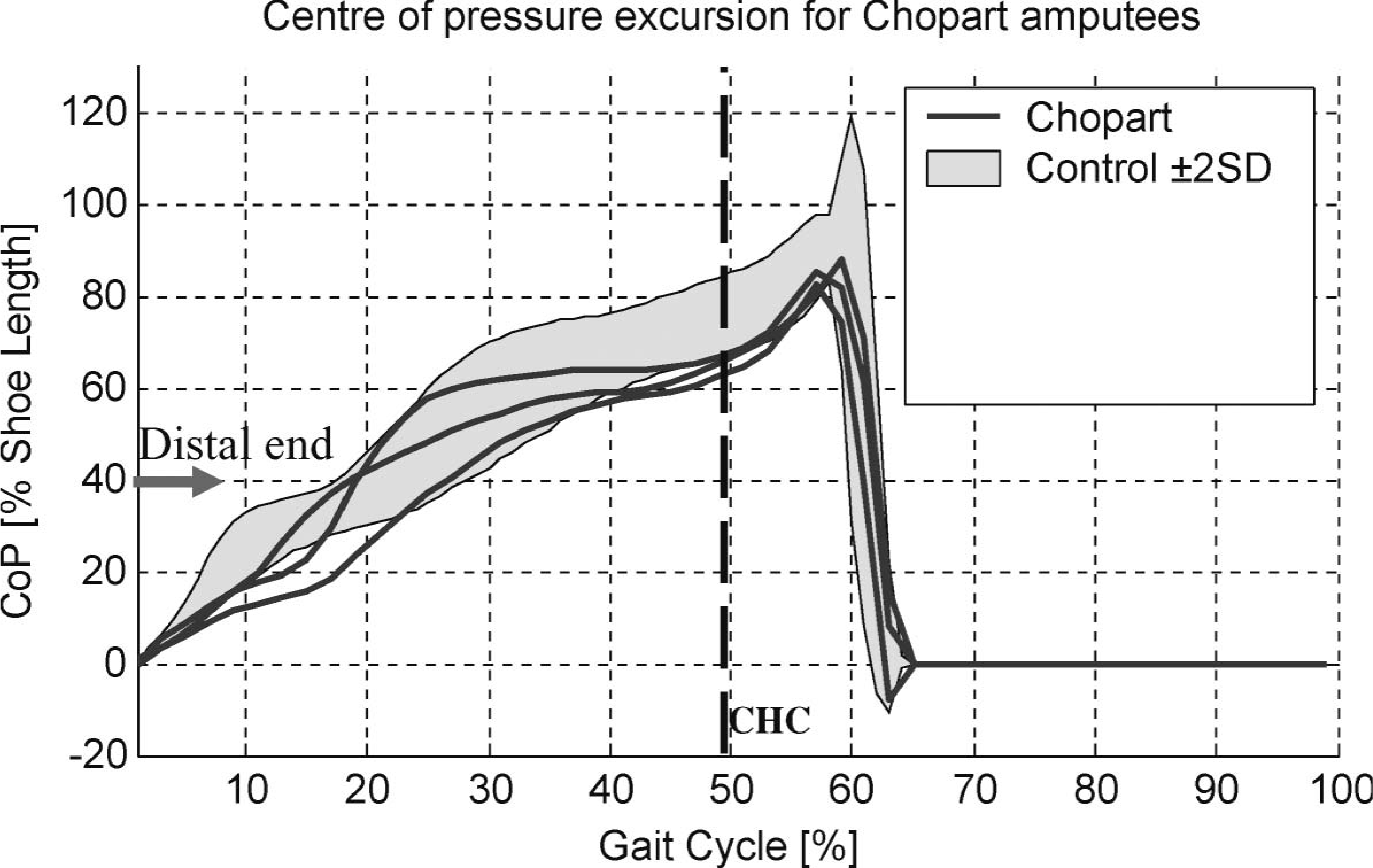
Centre of pressure excursion for the affected limbs of the Chopart amputees. CHC: contralateral heel contact; CoP: centre of pressure expressed as a proportion of shoe length; the distal end of the stump is located at approximately 40% of shoe length.
Discussion
Particularly in the TMT and Lisfranc amputees, the CoP remained well behind the distal end of the stump until after CHC occurred when the superincumbent mass could be supported by the contralateral lower limb during double support. In this way, the CoP was able to progress past the distal end when the magnitude of the GRF was rapidly declining as body weight was shifted to the contralateral limb.
The TMT and Lisfranc amputees may have adopted this gait pattern for a number of reasons. It is difficult to determine whether the primary reason was:
to spare the sensitive distal stump from the extreme forces typically observed during terminal stance by not allowing the CoP to progress across the distal end until after CHC when the magnitude of the GRF was rapidly diminishing;
to reduce the requirement of the triceps surae musculature by moderating the distal excursion of the CoP, thus reducing the external moment and the internal muscle/prosthetic requirements; or
due to the limitations of prosthetic design.
In terms of prosthetic design, the toe fillers, foot orthosis, and slipper sockets fitted to the TMT and Lisfranc amputees were unable to restore the ‘effective’ foot length, indicating that the amputees were unable to utilize the prosthetic forefoot for substantial weight bearing. There may be a number of possible explanations. The toe fillers and foot orthoses did not incorporate a socket which could rigidly couple the stump and prosthesis. The slipper sockets did incorporate a true socket but may not have been able to comfortably transmit the forces caused by loading the toe lever to the small surface area of the Lisfranc stump. The toe levers in all these devices were likely to have been too flexible, given that they were manufactured from either plastazote or polypropylene of little more than a few millimetres in thickness.
In contrast, the clamshell devices fitted to the Chopart amputees were able to effectively restore the lost foot length, thus enabling the amputees to adopt a gait pattern, whereby the peak GRF occurred commensurate with the CoP being located well beyond the distal stump. The clamshell prostheses seemed well suited to the task because they incorporated a rigid toe lever, of either thick carbon fibre or the distal half of a prosthetic foot bonded to the socket, and a substantial socket capable of comfortably managing the external torques which occurred by loading the prosthetic forefoot.
The static force analyses which are endemic within the literature have incorrectly depicted the point of application of the GRF during terminal stance for TMT and Lisfranc amputees using toe fillers or slipper sockets; suggesting that these devices are able to restore the lost foot length, such that the GRF is well advanced into the prosthetic forefoot when the second peak of the vertical GRF occurs. Results from the current investigation do not support this contention but suggest that these static force analyses should depict the GRF well behind the distal stump when the magnitude of the GRF is largest during terminal stance. Literature illustrating static force analyses for Chopart amputees using clamshell type prosthesis, such as that provided by Condie (1970), accurately describe the point of application of the GRF during terminal stance.
Conclusion
The aim of this work was to evaluate whether partial foot prostheses were able to ‘effectively’ restore the lost foot length. This investigation reports that the TMT and Lisfranc amputees adopted a gait pattern consistent with an inability to ‘effectively’ utilize the prosthetic forefoot of devices such as toe fillers and slipper sockets. While these amputees may have adopted this gait pattern to protect the sensitive distal residuum or reduce the requirement of the triceps surae musculature, there would appear to be a number of limitations inherent with existing devices designed to allow ankle motion given that the clamshell prostheses were able to ‘effectively’ restore foot length in the Chopart amputees. The static force analyses, so endemic within the literature, accurately describe the point of application of the GRF for clamshell devices during terminal stance but should be amended to illustrate that the GRF remains proximal to the distal residuum in MTP, TMT, and Lisfranc amputees using toe fillers and slipper sockets.