
Abstract
This retrospective study was designed for the period 1982 – 2002 to collect the basic data on the demography, level and side of the amputation, involved limbs, age, gender, and prosthetic functional level in children with limb loss. A total of 232 children were assessed through their prosthetic records. Seventy-two percent (195 children) presented lower-limb involvement, and 28% (77 children) had upper-limb loss. The age of the children varied between 1 and 15 years with a mean age of 9.90 ± 2.32 years. Results of the study revealed that the leading amputation cause in children was congenital limb absence. The most frequent levels were determined as trans-tibial and trans-radial in lower and upper limbs, respectively. Findings showed that more boys (60%) were affected, and 84% of all amputations were found to be unilateral. It was also seen that right-side amputations (54%) were more common than left-side amputations (46%). The outcome of the study showed that 96% of children with lower-limb loss reached a functional gait pattern without any aids, while the percentage of independence in activities of daily living was found to be 88% in upper-limb loss.
Introduction
Demographic studies have established the preponderance of congenital limb loss to acquired limb loss as 2:1 (Masada et al. 1986; Vannah et al. 1999). The precise cause of congenital limb deficiencies is unknown, and defects of upper limbs are twice as common as those of the lower limbs (Hirons et al. 1991).
Congenital limb loss is classified as being either transverse, which is similar to an amputation stump, or longitudinal, in which some distal skeletal elements remain. The incidence of acquired limb deficiency is not known (Day 1991; Krebs et al. 1991). Seventy-five percent of acquired amputations in children were due to trauma, and the rest were due to disease process (Bryant and Pandian 2001).
International literature shows that traumatic amputations in children are mainly caused by power tools and machines, vehicular accidents, gunshot wounds, and thermal or electrical injuries (Krebs et al. 1991).
Tumours are the primary disease cause leading to acquired amputations in children. Other disease-related causes are vascular malformations (rheumatoid vasculitis), neurogenic problems, and some rare diseases such as chickenpox (Carnegie 1999; Pandian et al. 2001).
Patients and methods
Some 232 children with limb loss were evaluated for their demographic characteristics and functional achievements. In their initial visit, a physiotherapy assessment was performed to determine whether there was an ability to bear weight through the skeleton and to determine the power, range, and stability of the joints (Carnegie 1999; Esquenazi and Meier 1996).
In post-operative and pre-prosthetic phases, a rehabilitation programme focusing on positioning, bandaging, and strengthening was given to the children with acquired limb loss with the aim of preparing them for prosthetic fitting. Children with congenital limb deficiency were treated to improve the functional use of the residual and intact limbs, in order to enhance their activities of daily living with and without prostheses. The design of the prostheses and selection of the prosthetic materials were carried out, considering individual needs depending on the level or type of the limb loss. Children with lower-limb deficiency, except those distal to trans-tibial amputations, were provided with modular lower-limb prostheses with a SACH foot, and children with upper-limb deficiency were given modular or mechanical functional upper-limb prostheses with voluntary opening prosthetic hands.
Prosthetic knee joints were not used for each child with lower-limb deficiency until the child could walk safely. For the trans-femoral level, the initial prosthesis did not employ a functional knee module. The shank and foot are made as one piece from rigid Pedilen foam by mixing an equal amount of Rigid Pedilen Foam with Pedilen hardener and pouring it into a polypropylene conic cylinder made to fit the socket dimensions at one end and approximately 12 cm in anteroposterior diameter at the other end for the foot.
Since it is not cost-effective to store feet smaller that 15 cm long which are used for 3.5- to 4-year-old children, a method was devised of fabricating prostheses for toddlers. From 4 years old onward, a standard prosthesis is fabricated.
In the beginning of the prosthetic phase, the stump – socket fit was checked, and the lower attachments were performed. After static biomechanical alignment of the prostheses, a dynamic evaluation was carried out to see whether there were any skin irritations or breakdowns and difficulties during the use of the prostheses. Following realignment or socket modification procedures, the children were given prosthetic training.
In children with lower-limb loss, prosthetic training started with free walking and continued with balancing, weight-shifting and ambulation activities (walking, ascending and descending stairs and inclines, crossing obstacles, picking up objects from the floor, getting on and off a vehicle).
Teaching the opening of the prosthetic hand was the first step in rehabilitation of children with upper-limb deficiency. Grasp and release activities were followed by activities of daily living (ADL) training including self-care such as dressing, brushing teeth/hair, feeding activities, and other skills such as holding a telephone receiver or a paper, or opening or closing doors.
All the children received prosthetic treatment for three weeks, 4 h a day. At the end of the training period, the children were assessed for their ability to perform ADL on a four-point scale as follows:
4—independent: activity was performed without using any aid/assistance;
3—independent with the help of a device: activity was carried out independently with the aid of a walking or self-help device;
2—partially independent: the activity could only be performed with the assistance of someone else;
1—the activity could not be performed at all.
Results
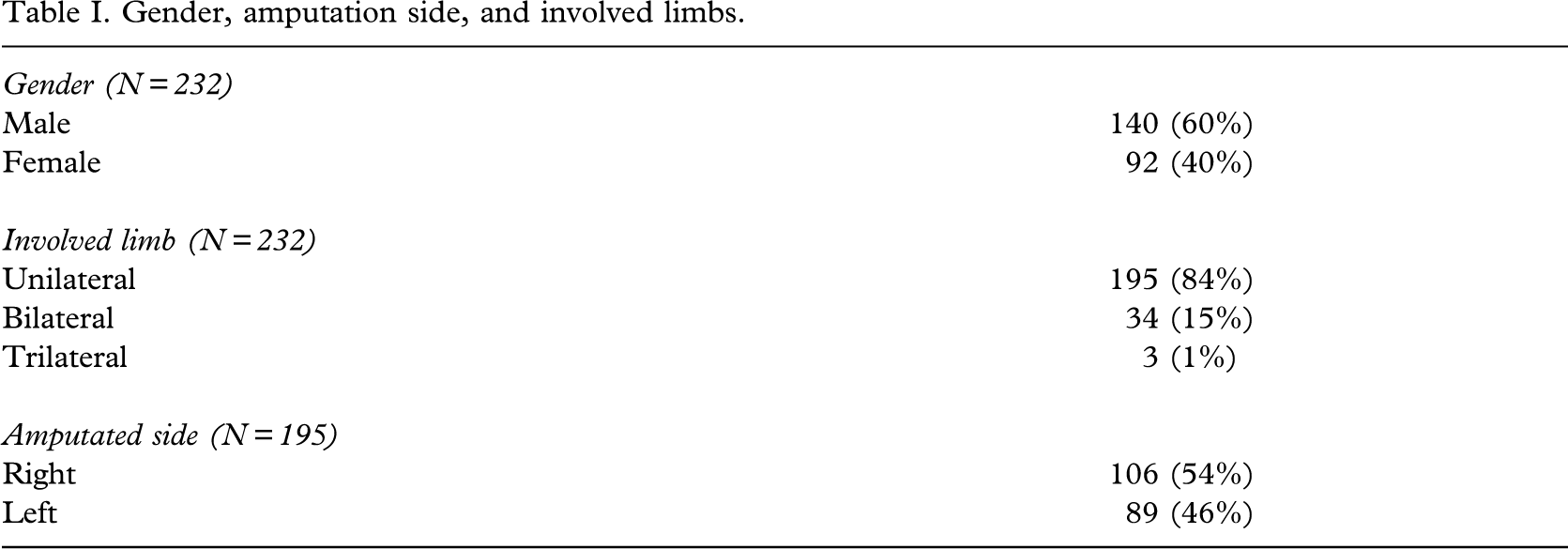
The records of 232 children were examined, comprising 92 (40%) girls and 140 (60%) boys. Ages of children varied between 1 and 15 years. The mean age was 9.90 ± 2.32 years in girls and 10.50 ± 1.92 years in boys. The male-to-female preponderance was found to be 1.5:1 (Table I).
Gender, amputation side, and involved limbs.
The principal cause of childhood limb absence was found to be congenital limb deficiency, while the next most common cause was noted as traffic accidents (Figure 1). Seventy-five children (32%) of the study group presented with congenital limb deficiency, while 157 children (68%) had acquired limb loss. The preponderance of congenital limb loss to acquired limb loss was 1:2. Out of the 157 children with acquired limb deficiency, lower-limb loss was determined in 112 (71%), and upper-limb loss was found in 45 (29%).
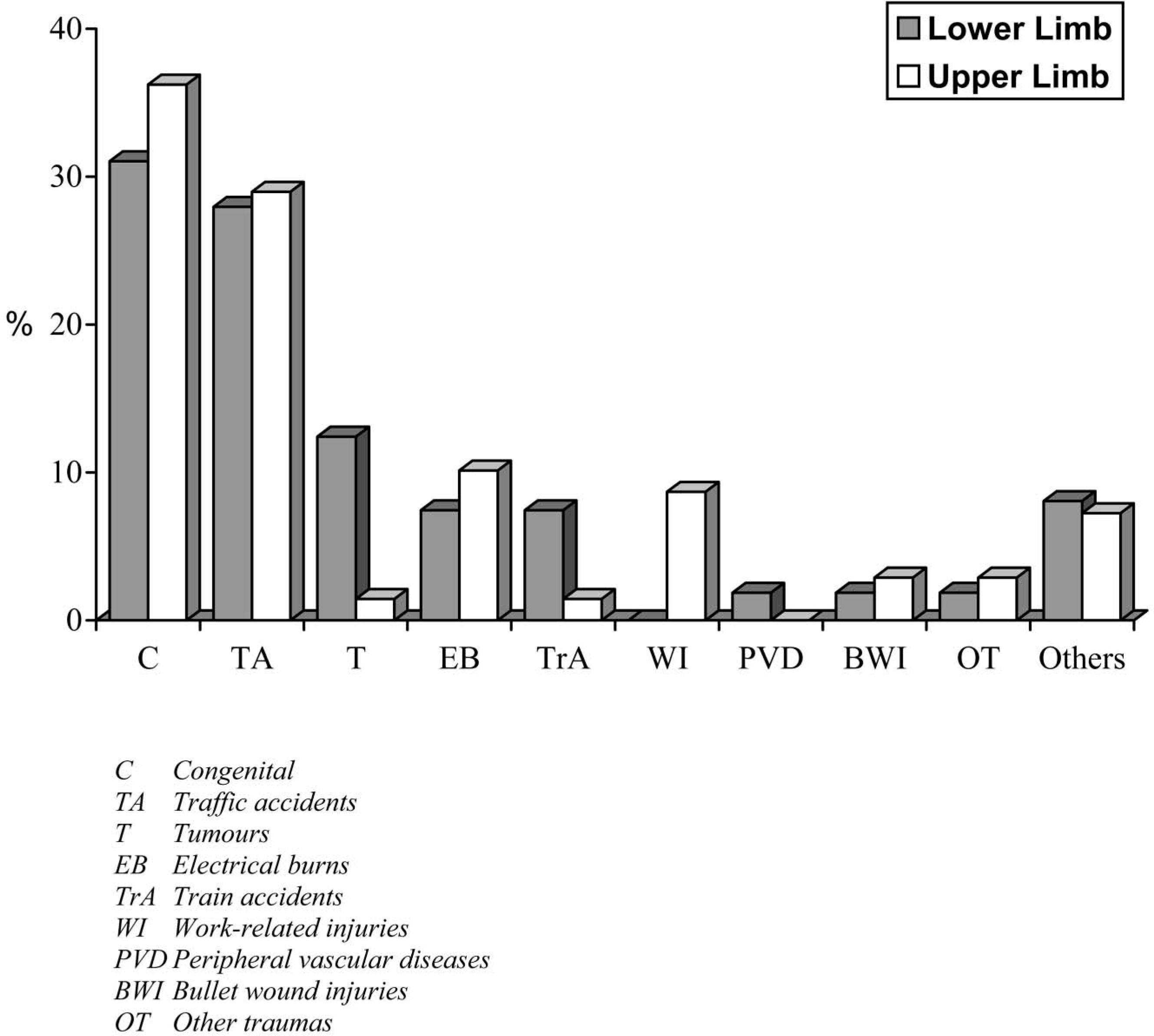
Causes of amputation.
Of the 195 children with unilateral limb loss 139 (71%) presented with lower-limb deficiency while 56 (29%) had upper-limb involvement (Table I).
The majority of the children (54%) had right-sided limb loss (Table I). The most frequent level of limb deficiency was trans-tibial (43%) in children with lower-limb loss and trans-radial (44%) in children with upper-limb deficiency (Figures 2 and 3).
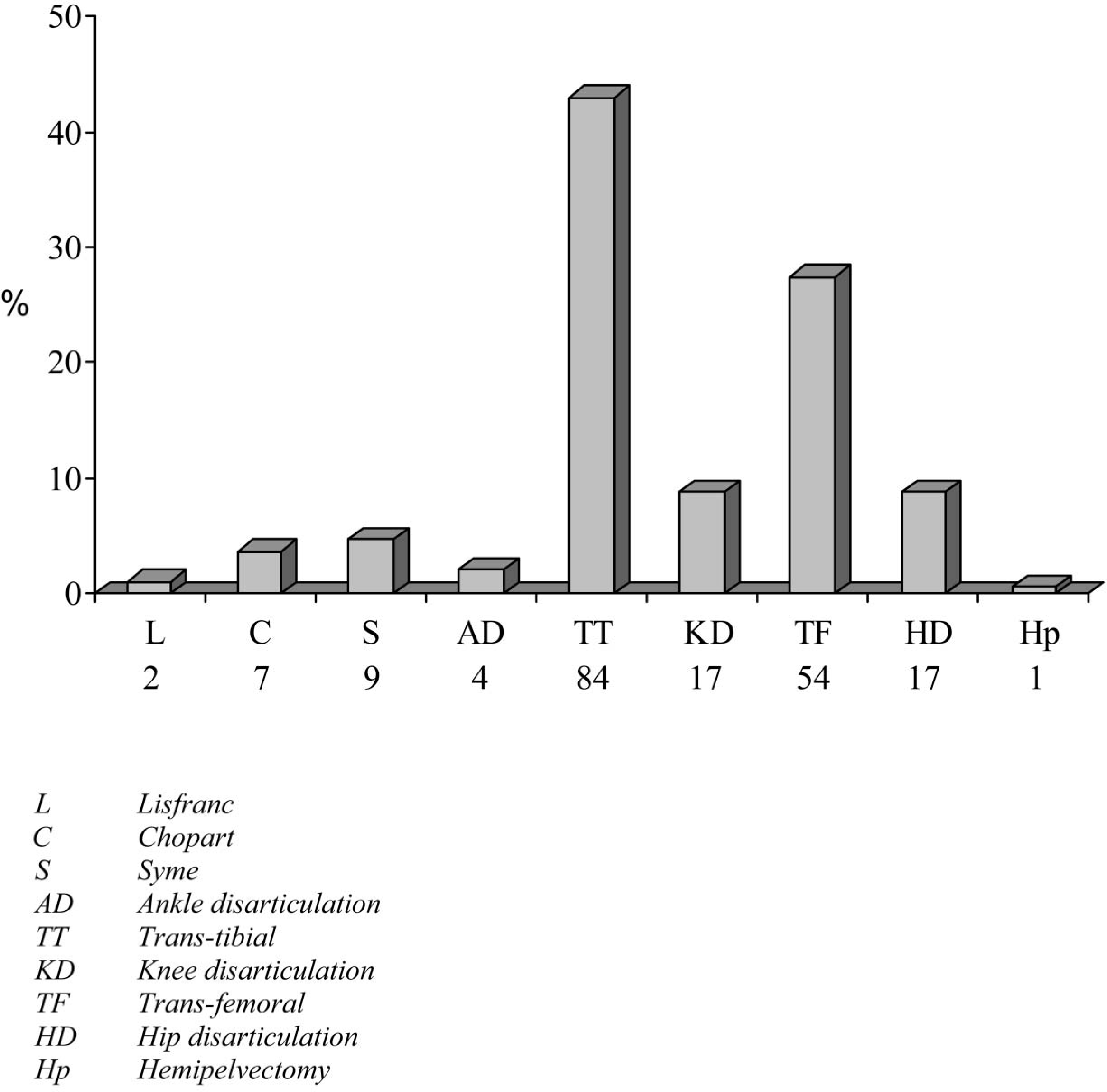
Amputation levels in the lower limb, including bilateral and trilateral amputees.
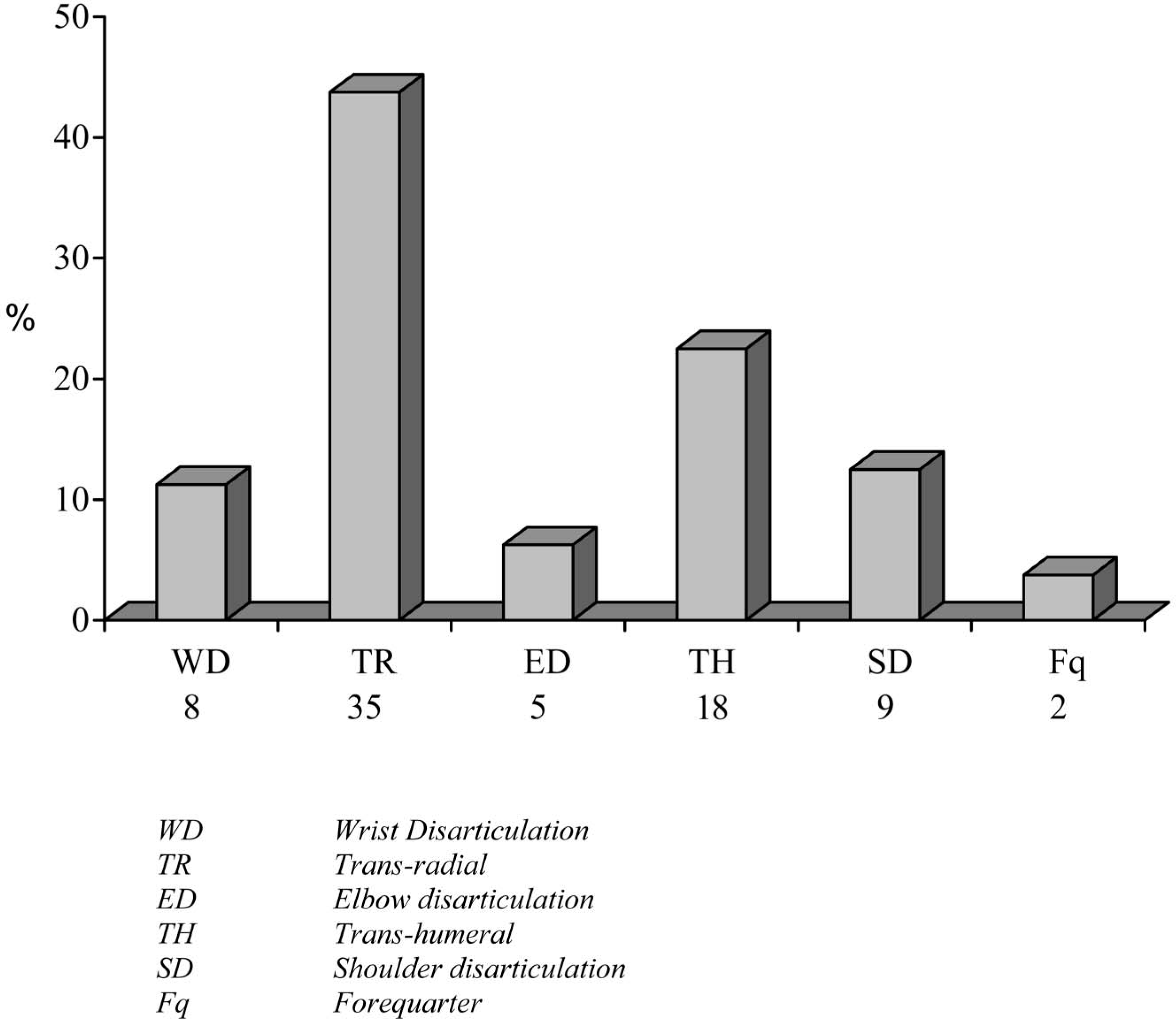
Amputation levels in the upper limb, including bilateral and trilateral amputees.
Twenty-nine out of 75 children with congenital limb deficiency were under 5 years of age, while the ages of the other 46 children with congenital deficiency varied between 7 and 13 years. Some 11 out of 29 children with congenital limb deficiency were 1–3 years of age while, the rest (18 children) were 3–5 years of age. Longitudinal limb loss was determined in 16 children with lower-limb deficiency and 11 children with upper-limb deficiency children.
Out of 75 children with congenital deficiency, there were 16 with longitudinal lower-limb loss and 11 with longitudinal upper-limb deficiency. Transverse lower-limb loss was present in 33 children, while 15 children had transverse deficiency in the upper limb (Table II).
Deformity type of children with congenital limb deficiency (n=75).

The age at first prosthetic fitting varied between 12 months and 15 years in children with lower-limb deficiency and between 5 months and 10 years in children with upper-limb deficiency. It was found that seven children were provided with prostheses around 12 months of age. Four children were supplied with passive upper-limb prostheses.
From the records, it was found that 14 children were fitted with their first prosthesis at 13–15 years of age. Amputation causes in these children were occupational trauma in six, neoplasm in five, train accident in two, and a bullet wound in one (Figure 1).
Functional assessment results following prosthetic treatment showed that 96% of children with lower-limb deficiency performed ambulation activities independently. Two patients required walking aids.
Eighty-eight percent of children with upper-limb deficiency performed activities of daily living independently. Nine of them showed independence with self-help devices; these were the children with proximal amputations/deficiencies or bilateral involvement.
Discussion
The results of this study showed that the primary cause of the limb deficiency is congenital, as reported in the international literature (Kuyper et al. 2001; Scotland and Galway 1983).
This present study showed the preponderance of congenital limb loss to acquired limb loss as 1:2, while this has been established as 2:1 in international literature. The higher number of children with acquired limb loss may be because there are more educationally and economically challenged children in the studied population leading to a greater exposure to work accidents. The children with congenital limb deficiencies try to overcome their disabilities by using their residual and intact limbs, and they do not undergo medical and prosthetic care. More emphasis must be given to this issue in a future planning project.
From the previous study on congenital malformations carried out in this department, family history records pointed out that marriage between close cousins was still traditional in Turkey (Sener et al. 1999). This result is of great importance in relation to planning educational community health programmes.
The findings showed that 71% had unilateral lower-limb loss, while 29% had unilateral upper-limb involvement. However, researchers have found that upper-limb loss is more common (Kuyper et al. 2001; Scotland and Galway 1983). The results of this study indicated that lower-limb loss causes more difficulties in daily living, and the parents are more sensitive to lower-limb involvement because of the loss of locomotor function.
From the family history, it was recorded that children showed a tendency to crawl on their knees to ambulate if they had not received prostheses.
In unilateral upper-limb loss, activities of daily living could be performed with less assistance. Thus, parents need to make much more effort to cope with the disability of their children having lower-limb loss.
Results of the study revealed that the second most common cause of limb loss in children was traffic accidents. This is not surprising when one considers the lack of parental and community health care education and insufficient organization in designing safe/protected playgrounds and sports facilities.
Researchers state that unilateral involvement is around 90% in acquired limb loss in children of which 60% of present with lower-limb loss. Acquired amputations show a 2:1 male-to-female preponderance (Bryant and Pandian 2001; Vannah et al. 1999). In the present study, 84% showed unilateral involvement, and 60% were boys. This result probably arises from the more active nature of boys and greater exposure to trauma, compared with girls.
International literature points out that unilateral lower-limb loss is the most frequent involvement in adult amputees, while multiple limb loss is seen in 20% of children with limb deficiency. These deficiencies mostly consisted of complex congenital malformations such as proximal focal femoral deficiency (Bryant and Pandian 2001; Hirons et al. 1991; Kuyper et al. 2001). According to the authors' results 34 (15%) children presented with bilateral deficiency, and three (1%) children showed trilateral deficiencies.
The present study found that the most common limb-loss levels were trans-radial (44%) and trans-tibial (43%) in upper and lower limbs, respectively. The next most common levels were determined to be trans-femoral (27%) and trans-humeral (23%). These results are also parallel to previous studies (Bryant and Pandian 2001; Kuyper et al. 2001).
Only a minority of the children (eight) used walking aids, while 96% of children with lower-limb deficiency were completely independent in ambulation. Some 88% of upper-limb amputees were shown to be independent in activities of daily living, while 10 children required self-help devices. These were the children with bilateral upper-limb loss.
In the views of the authors, the results attained from the study showed that children became functional prosthesis users. The reason for this outcome is the ease in motivating the children when trying to improve their functional capabilities during prosthetic treatment (Pruitt et al. 1999).
Literature concerning prosthetic rehabilitation shows that children with all kinds of limb loss could be supplied with prostheses. In multiple limb deficiencies and proximal levels, the children can be trained to compensate with the head, trunk, or existing limbs (Kuyper et al. 2001, Sener et al. 1999). However, automatically developed compensatory skills lead the child to perform daily living tasks easily. In the adolescence period, the cosmesis becomes the first need of the child, and if this is not provided in the prosthesis, acceptance will be difficult. The functional outcome gained by the children in this study is very important for their school and social adaptations.
Although the majority of the children in this study were given prostheses in a late period, they were found to be successful in activities of daily living and accepted their prostheses easily.
Rehabilitation with well-fitted prostheses is the key point of an active life style, which is the primary requirement of children.