
Abstract
The long posterior flap technique is an established technique for trans-tibial amputation in ischaemic limbs. Despite its success, it has a few drawbacks. It may be time-consuming and requires considerable planning, and at times the dog-ears cannot be avoided. The suture line passes over the distal end of the stump, which is usually a problem during prosthetic use. The skew flap technique retains the advantages of the long posterior flap technique and eliminates the difficulties of prosthetic fitting. The equal skin flaps are skewed so that the flaps become anteromedial and posterolateral, whereas the calf muscle flap remains long underneath the skewed skin flaps. The posterior muscles are brought anteriorly covering the cut ends of the bones and are buried in between the tibia and its anterior periosteum, by suturing their margins with the periosteum. The skew flap procedure was perceived in 1980 and was started at the Artificial Limb Centre, Pune in 1983 by the author. This procedure underwent many changes during the initial 5 years and by the end of April 1992, 85 trans-tibial amputations were performed using this technique. A 9-year follow-up of these patients, who had been using prostheses with ease and without any discomfort or problem, had been exceptionally good. Encouraged by the results, this technique is now being practised as routinely. By March 1998, a total of 125 such trans-tibial amputations had been performed in 119 patients, with excellent results.
Introduction
The long posterior flap technique is an established procedure of trans-tibial amputation in ischaemic limbs (Burgess et al. 1971). It has improved the rehabilitation prospects by saving the knee joint in the ischaemic limb, which otherwise could not have been saved by conventional methods. However, there are a few drawbacks. The operation is time-consuming and requires considerable planning; even in experienced hands, sometimes the dog-ears cannot be avoided. The stump, in the initial stages, is usually unsuitable for prosthetic fitting due to stump oedema, and subsequent bandaging to reshape the stump causes a considerable delay in prosthetic fitting.
Even after the above-mentioned difficulties are overcome, the main drawback is the suture line, which passes over the distal end of the tibia. This remains vulnerable to trauma due to the high pressure generated on this area while using the prosthesis. The skew flap method of trans-tibial amputation not only retains the advantages of the long posterior flap technique but also reduces difficulties faced by the patient, the surgeon, and the prosthetist.
Principle
The skew flap procedure was perceived in 1980 and was started at the Artificial Limb Centre, Pune, in 1983 by the author (Jain et al. 1988). This procedure underwent many changes during the initial five years, and by the end of April 1992, 85 trans-tibial amputations were performed using this technique. A nine-year follow-up of these patients had been exceptionally good (Jain 1993). The principle of the skew flap technique is based on the observations that thermographic mapping of the leg shows a higher temperature profile on the anteromedial as well as the posterolateral aspect (Figure 1). This finding indicates a better blood flow, or say better nutrition, of the anteromedial as well as the posterolateral areas below the knee joint. This was also determined by the transcutaneous measurement of partial pressure of oxygen (TC pO2) by the author (Jain 1982), confirming a better blood flow in these areas below the knee joint. Coddington and Dewar (1981) also noticed similar findings. The skew flap technique is based on these observations. The skin flaps correspond closely to the characteristic warm pattern of skin and underlying tissues.
Patients and methods
Wherever feasible, the skew flap technique was used for all patients at the Artificial Limb Centre, Pune who required trans-tibial amputation between January 1983 and March 1998. No specific selection of patients was made. The operation was normally performed under general anaesthesia; spinal anaesthesia was also used whenever the patient was not considered suitable.
Pre-operatively, one dose of antibiotic was routinely given to all patients. Post-operatively, antibiotics were continued for 5 days.
The skin flaps were marked by the following procedure. A circumferential marking was made 20–25 cm below the knee joint line. This was bisected equally, keeping one end at a point 2.5 cm lateral to the tibial crest, with the opposite point coming on the posteromedial aspect. Semicircular flaps were then marked from these points, keeping the length of the flaps at least one-quarter of the circumference (Figure 2).
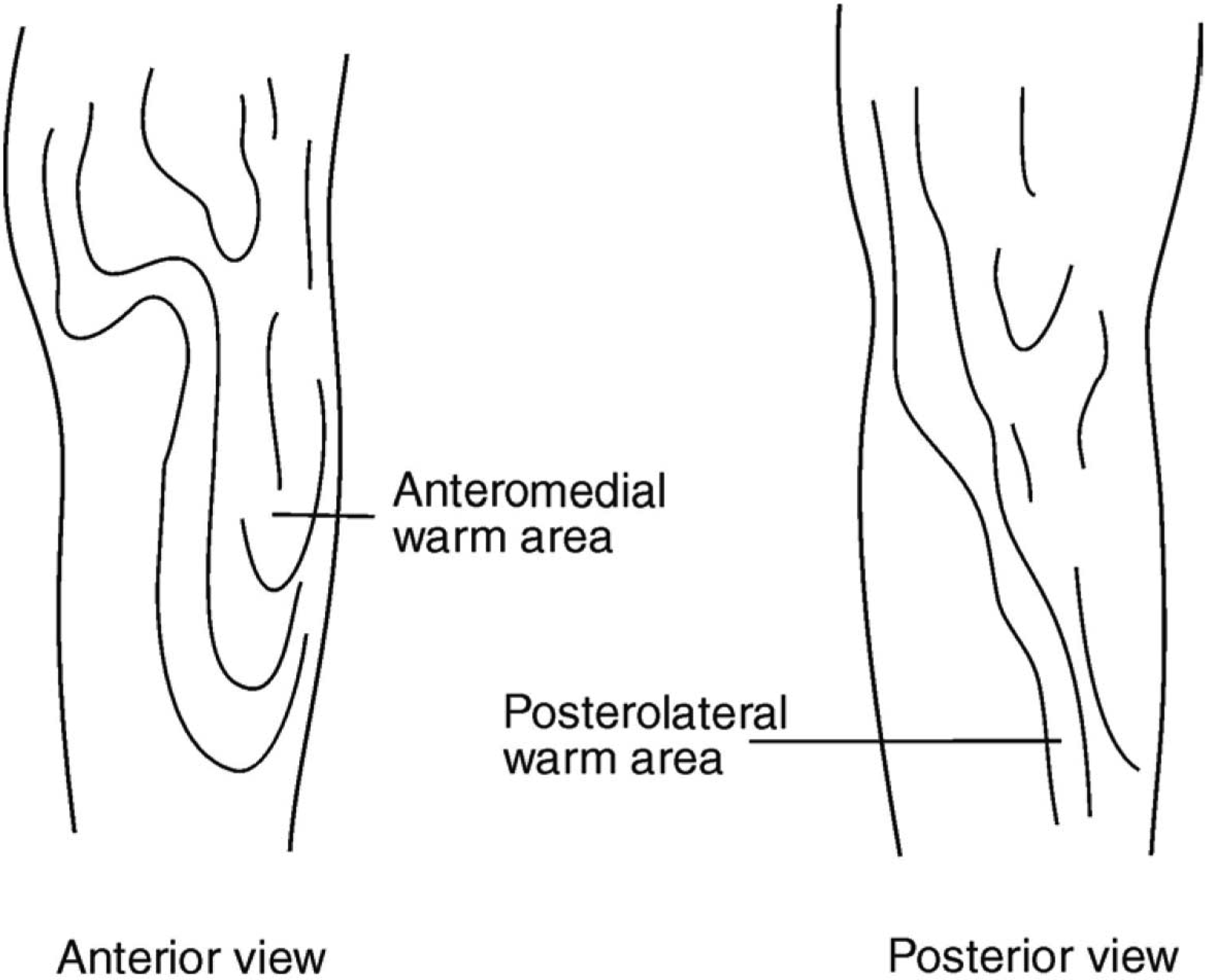
Thermographic imaging of leg showing a higher temperature on the anteromedial as well as the posterolateral aspect.
Incision was made as marked and deepened, dividing the deep fascia. On the anterior aspect, the periosteum over the subcutaneous surface of tibia was also divided. The periosteum was cleared all round the tibia and then reflected up to a point just above the proposed line of bone section. All the muscles of anterior tibial compartment, peroneal muscles, and long flexors of the toes were divided at the level of bone section, while the full length of the calf group of muscles was preserved.
The fibula was exposed and divided 1 cm above the proposed tibial section. The tibia was then divided. The distal tibial portion was pulled down to expose and separate the gastrocnemius-soleus muscle mass from the bone as shown in Figure 3. The distal skin was also cleared from these muscles, which were then divided transversely, freeing the lower portion of leg.
Haemostasis was achieved carefully by doubly ligating major vessels. The nerves, anterior tibial and peroneal, were pulled distally and ligated as proximal as possible. They were then divided and allowed to retract. This is an important step.
The distal sharp end of the tibia was properly bevelled and smoothened with the help of a rasp. This was an important step in the operation and should be done with care. Sharp projections from the fibula were also smoothed.
The calf muscles were then dealt with. Their length below the cut end of tibia had to be slightly longer than the diameter of the leg. This extra length of gastrocnemius-soleus was required to cover the whole of the distal end of the stump reaching up to a point at least 1 cm above the anterior tibial margin.
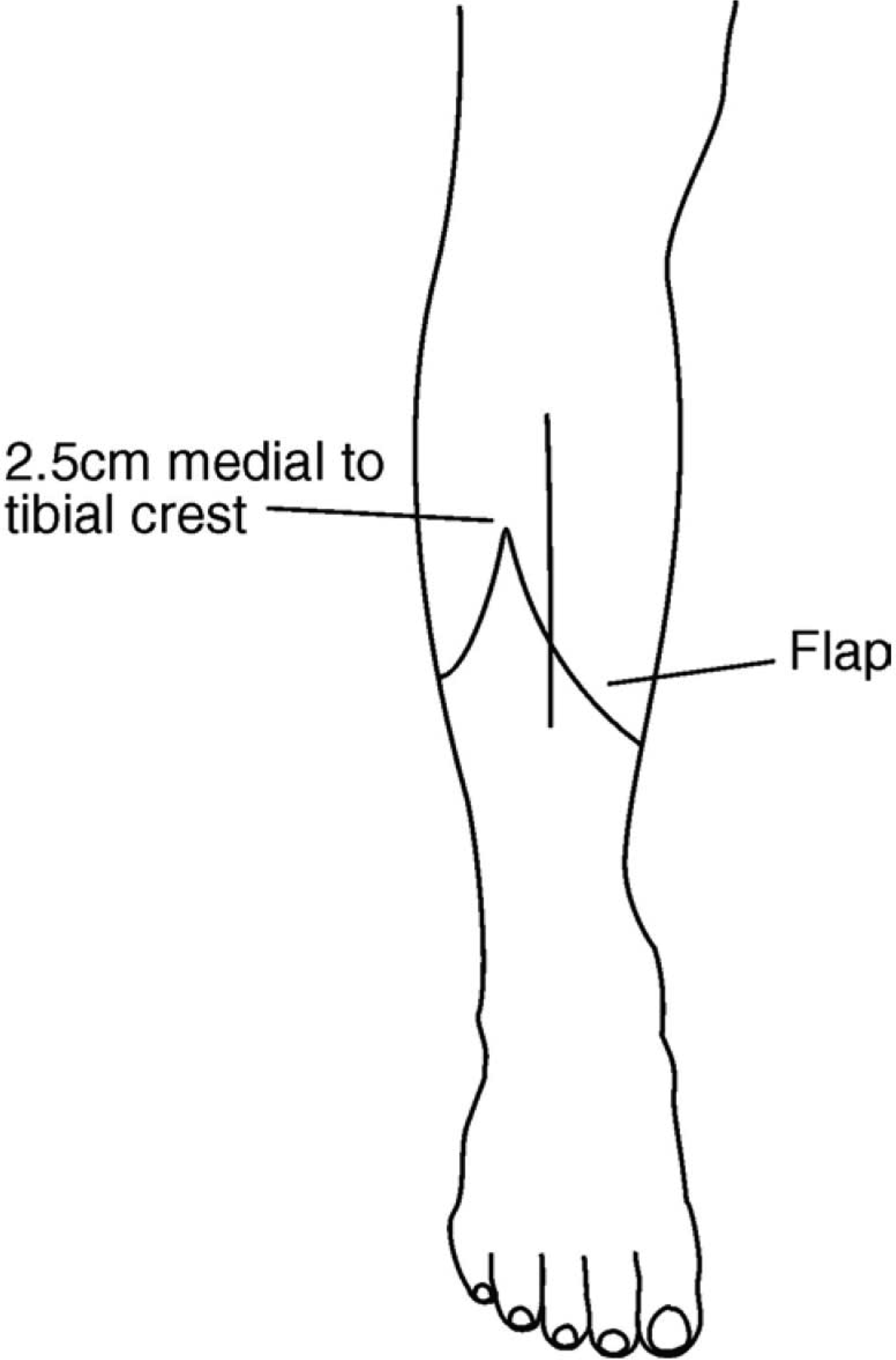
Marking of flaps.
The anterior tibial periosteum was reflected up to 1 cm from the tibial end. It was also freed from the skin. The distal margin of the posterior muscle flap was pushed in between the periosteum and tibia, and sutured with the periosteum as high as possible with the help of two or three mattress sutures, resulting in a double breasting, as shown in Figure 4. Care was taken to maintain the natural tension of the calf muscles, to achieve optimal function.
A drainage tube, preferably suction, was placed underneath the muscle flap. The deep fascia of the opposite flaps was sutured together meticulously. The skin was then closed.
Post-operatively, crêpe bandaging was done in such a way that there was no constrictive effect. The stump was elevated either with the help of a fracture board or by raising the foot end of the bed. A pillow under the knee or stump was never used. The stump was kept at rest for at least 3 days, followed by gradual passive movements. Active exercises were started during the second post-operative week onwards. Patients were asked to do exercises in the bed, including upper limbs strengthening and deep breathing exercises. They were gradually mobilized on crutches
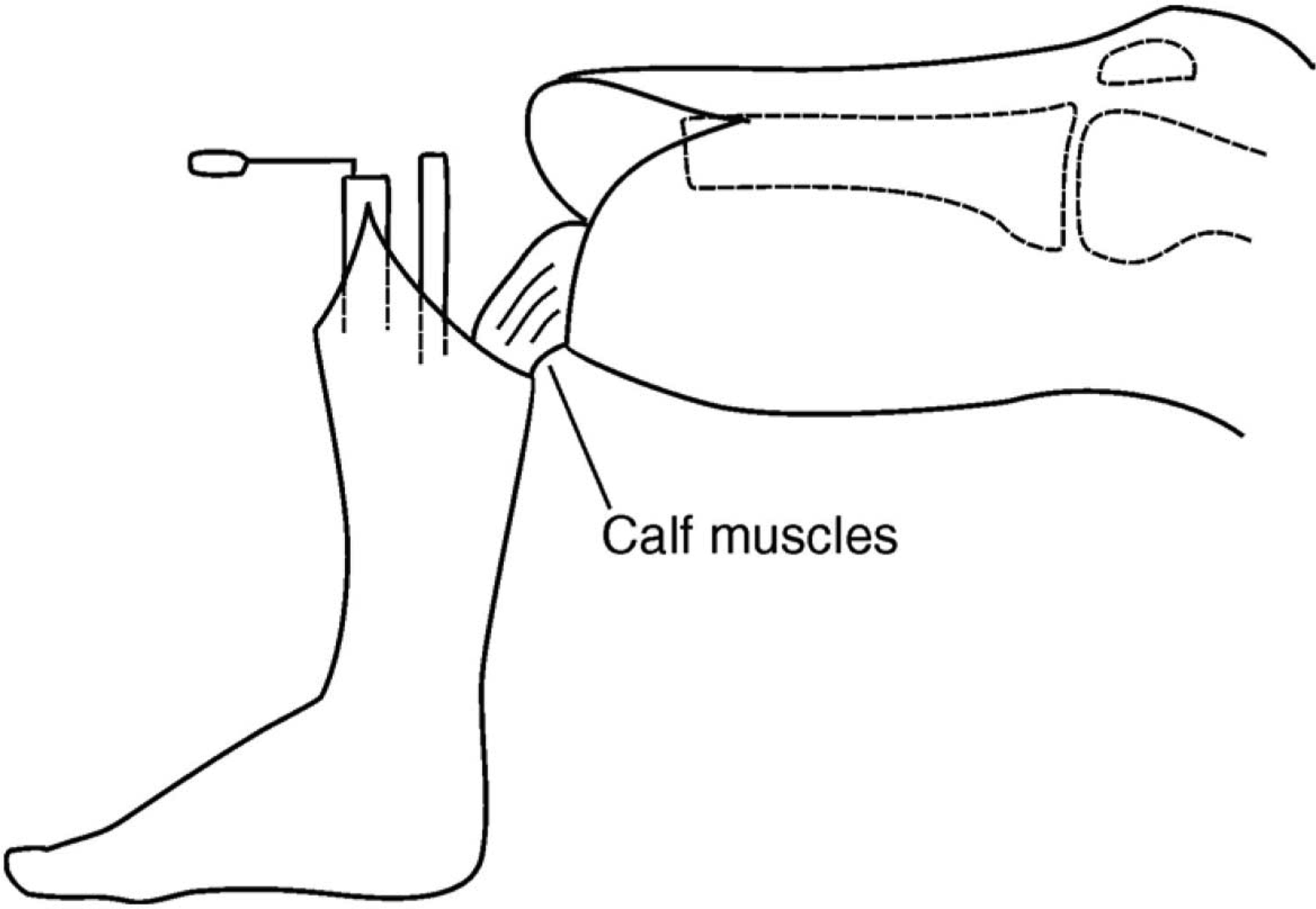
Removal of distal portion of leg preserving the calf muscles.
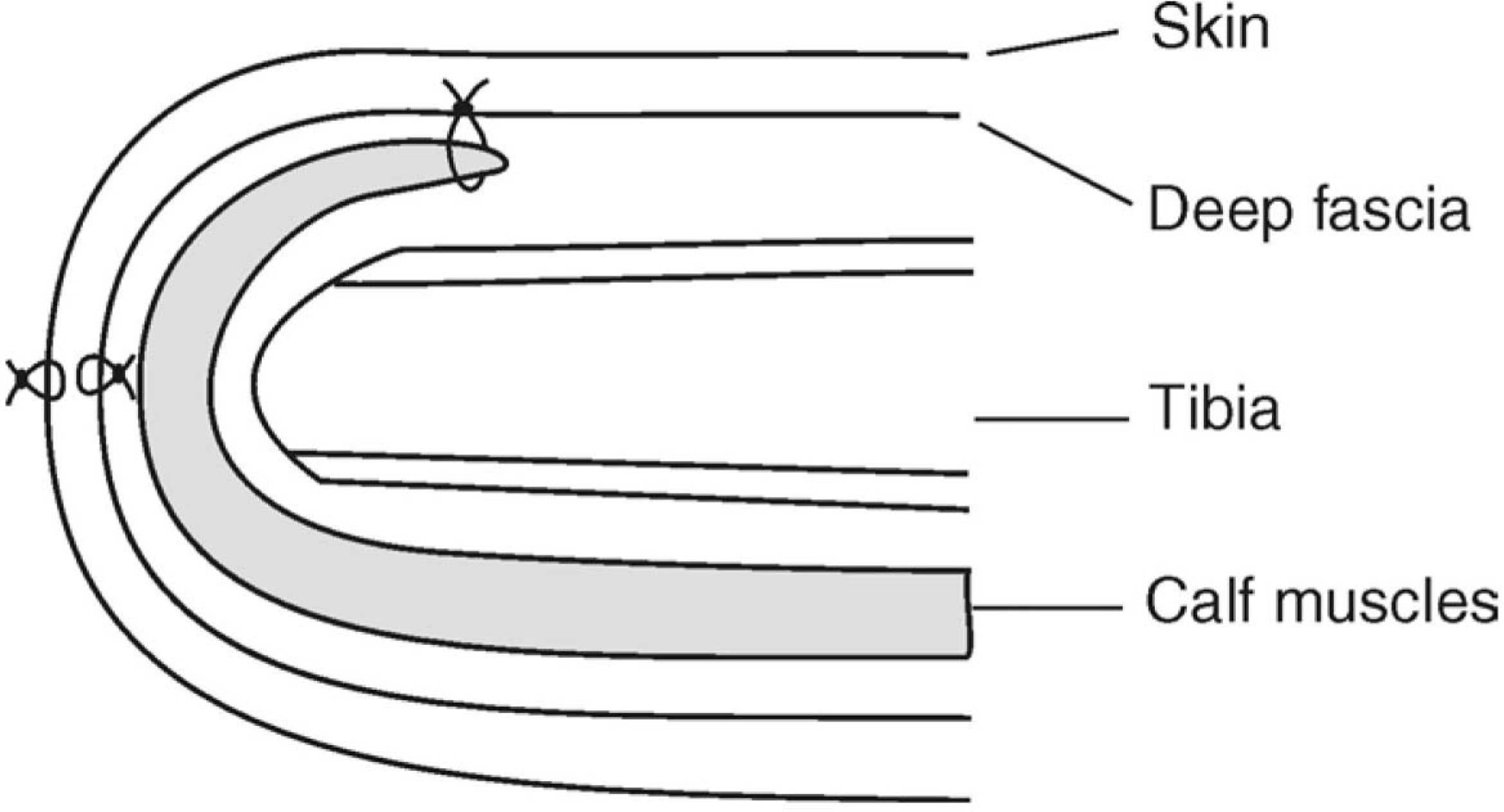
Schematic diagram showing the posterior muscle flap burying in between the tibia and anterior periosteum.
All amputees were followed up for a period of 5–15 years. The state of rehabilitation was assessed as excellent, good, fair, and poor depending upon the comfort and ease of wearing and using the prosthesis. Amputees who could not use the prosthesis were kept in a separate group. Amputees who used the prosthesis for over 12 h a day were termed as excellent, whereas limb users for over 6 h (but less than 12 h) and under 6 h were grouped as good and fair, respectively. Patients who used the prosthesis for a short period or used it only for cosmetic purposes were termed as poorly rehabilitated.
Observations
From January 1983 to March 1998 a total of 125 trans-tibial amputations had been performed using the skew flap technique in 119 patients, six of whom were double amputees. A follow-up for 5–15 years was carried out. Out of the 119 patients, 111 were male, mostly young.
The age distribution of the patients, who underwent amputation by the skew flap technique, is shown in Table I. The average age was 35 years. The predominant age group was 21–40 years (65.5%), whereas only 11% amputees were above 50 years of age.
The causative factors are shown in Table II. The commonest cause of amputation was trauma (56%). If the frostbite group were combined with trauma, since this is also a type of injury, the number of amputations due to trauma would increase from 70 to 91 (72.8%). Some 21.6% of amputations were due to ischaemia.
The post-operative complications are shown in Table III. Five patients died within 1 month of operation, two due to underlying disease and three due to advancing age. Antibiotics controlled wound infection, which was seen in 21 cases. Wound disruption was seen in eight cases, which required reamputation at a slightly higher level. Flap necrosis was present in three cases, and trans-femoral amputation had to be performed. Six stumps developed knee contracture, of which only four could be relieved by physiotherapy. In the remaining two cases, the contracture was accommodated in the prosthesis.
The state of rehabilitation and follow-up for 5–15 years has shown excellent and encouraging results. Only 92 patients were observed and analysed, since seven patients died, and 20 were not available for assessment and follow-up. After excluding these 27 patients, 81.5% amputees showed good to excellent results, whereas 18.4% performed poorly (Table IV).
It was observed that this technique has produced a smooth, well-padded stump without any dog-ears on either side. The end of the tibia remained well padded by the muscle flap.
Age distribution of patients (n = 119).
Causative factors (n= 125).
Post-operative complications (n = 125).

State of rehabilitation (n = 92 excluding patients not available for follow-up).
Measurements for the definitive prosthesis could be taken within 3–4 weeks of operation in most of the cases. The average period of stay in the hospital was 35–40 days.
Discussion and results
The long posterior flap technique had changed the management and rehabilitation of patients with ischaemic limbs, since its inception in 1956 (Kendrick 1956). This resulted in an increase in the number of trans-tibial as compared with trans-femoral amputations. The procedure was popularized by Burgess et al. (1971) in the late 1960s and became an accepted procedure for ischaemic limbs (Vitali et al. 1986).
The posterior flap technique has its own problems. Upward folding of the posterior flap jeopardizes the circulation and also results in dog-ears on either sides of the scar and makes the distal end bulky. An attempt to reduce the dog-ears further effects the circulation and viability of the flaps, which are already ischaemic. Invariably, the scar lies over the anterior terminal end of the stump and remains susceptible to injury while using the prosthesis due to generation of high pressure on this area.
These disadvantages have been overcome by the skew flap technique. Equal skin flaps avoid dog-ears. Terminal end of the bones remains well padded by the muscles without making the stump bulky. The scar becomes oblique anterolateral to posteromedial and passes in between the terminal ends of tibia and fibula. Thus, the vulnerable area over the lower anterior aspect of the stump is formed by normal skin and can bear high pressure, generated at this area while using the prosthesis. Harrison et al. (1987) and Ruckley et al. (1991) also noticed similar advantages of the skew flap technique over the long posterior flap technique. Allcock and Jain (2001), in their series of 445 trans-tibial amputations during 1987–1996, performed the skew flap procedure in 50 patients. They considered the long posterior flap technique to be better than the skew flap technique. In a recent Cochrane review, Tisi and Callam (2004) did not find any advantage of one technique over another.
It has been observed by thermographic mapping that the blood flow is better on the anteromedial and posterolateral aspect, as indicated by the warmer surface temperature on these areas below the knee (McCollum et al. 1985). This finding has also been confirmed by the transcutaneous measurement of partial pressure of oxygen (Robinson et al. 1982; Jain 1987). The skewed flaps correspond more closely to the characteristic warm pattern and also the better oxygenation pattern of skin and underlying tissues.
Bevelling of tibia is an important step (Robinson 1991); if not done properly, the skin over the end of the tibia will be crushed between the socket from outside and bone from inside, as shown in Figure 5.
Burying the terminal portion of calf muscle in between the tibia and its anterior periosteum has been achieved after many trials of various methods to prevent sagging of calf muscles, which leaves the end of the tibia absolutely bare. The procedure of burying the margins of the calf muscles in between the tibia and anterior periosteum has now overcome both these difficult problems. The calf muscle does not sag, and the end of the tibia remains well padded with muscles. The tone of the calf muscle is also well maintained. Since the distal margin of the calf muscle is sutured with the anterior tibial periosteum proximally, the distal remaining end of the anterior periosteum is available for approximation with the opposing deep fascia. This approximation is necessary to keep the scar supple.
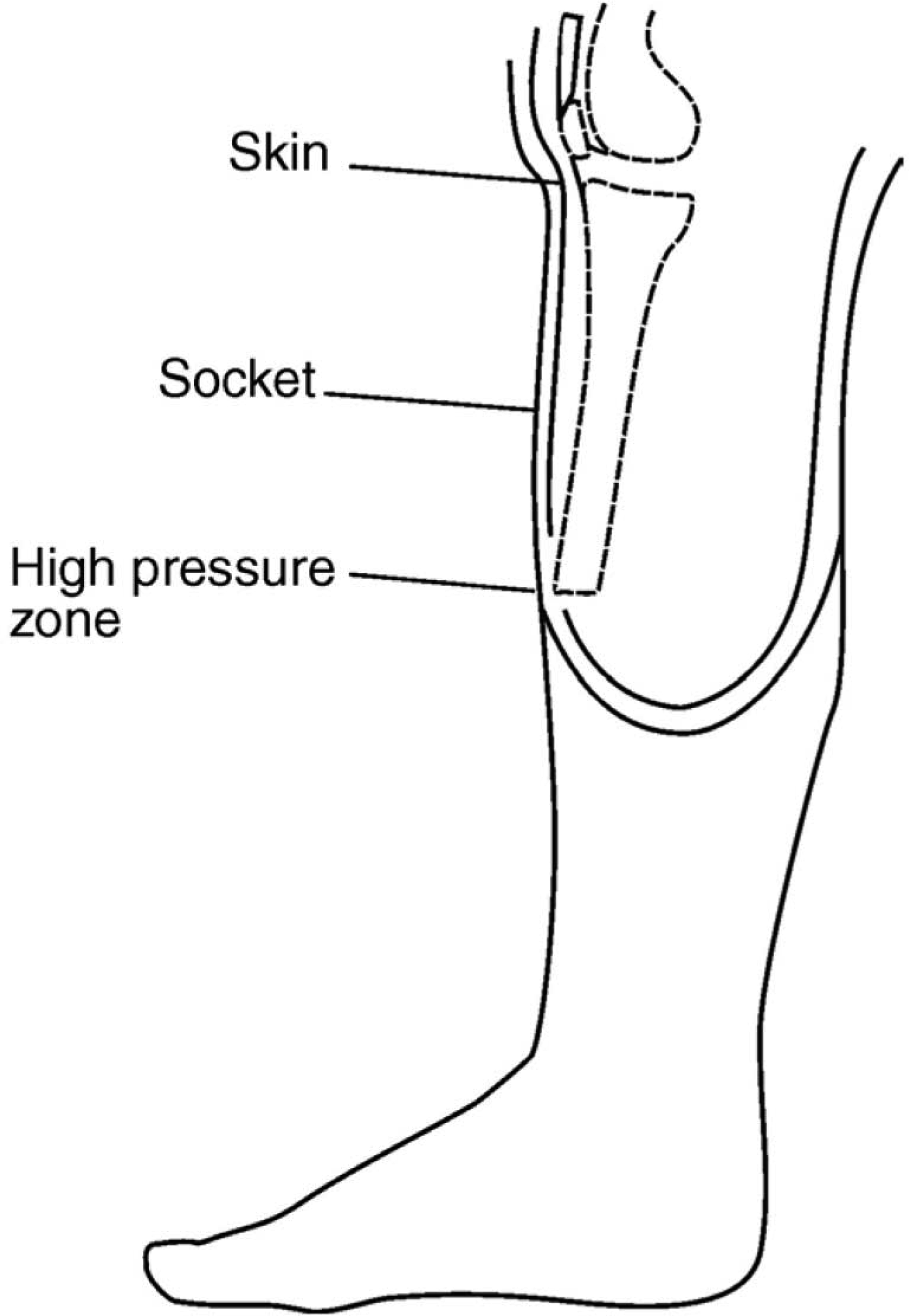
Skin crushed between the sharp tip of the tibia and the socket.
Biomechanical principles governing the stump/socket (PTB) interactions also indicate that the skew flap technique is scientifically sound and effective, compared with the conventional long posterior flap technique. Patients who have undergone a trans-tibial amputation by this technique, and have been using the prosthesis for 5–15 years, have also affirmed this finding.