
Abstract
The last three decades have seen an extensive body of literature that has investigated the prevalence of mental disorders among those in prisons and jails. A recent large scale meta-analysis of 23 000 prisoners succinctly summarized this evidence, estimating that 4% of prisoners were afflicted with psychotic illnesses, and 10–12% with major depression in the previous six months [1]. Notably, studies have consistently demonstrated that people with mental illnesses are over-represented in these institutions, and that rates of disorders in the criminal justice system are substantially higher than those found in the general population [2,3].
By contrast, the health and social needs of detainees at the front end of the criminal justice system (i.e. in police cells) are poorly understood. This is mostly because research has predominantly focused on the ‘captive population’ of prisoners within the broader criminal justice system [4]. However, it is arguably just as, if not more, important to investigate the needs of detainees being held in police cells to gain a more complete estimate of the prevalence of mental disorder and range and scale of health needs among those who come into contact with the police having committed an offence. This is because detention in police cells represents the first point of detention in the criminal justice service following the alleged commission of an offence and arrest by the police [5]. The acuity of psychiatric symptoms and prevalence of disorders and other health-related needs are likely to be significantly higher here than those found in prison due to the time lag between arrest and transfer to prison, the diversion of some offenders into mental health services [6], and the (albeit limited) available treatment opportunities possible (e.g. detoxification) if identified in police cells. Therefore rates of disorders in police cells are likely to be a better estimate of the prevalence of disorders within the offending population in the community, and are likely to be higher than those found in prisons and jails. The handful of studies that have been conducted at this interface support these propositions [7,8], and indicate an additionally vulnerable population [9–11]; however, they have been limited by the lack of systematized assessments of mental disorder and limited or no consideration of their broader health and social needs. Moreover, the deleterious effect of the police cell environment, such as the substandard conditions of police cells, further compounds the suffering experienced by those with a mental illness in custody [7,11]. As such, there remains an acute need to determine the scope of this health-related burden to help inform the potential need for partnerships between the police, primary care and mental health services [12].
Against this background, the aim of the study was to investigate levels of psychiatric disorders and individual needs in a sample of recently arrested police cell detainees. Based on previous findings of high rates of mental disorder in jails and prisons, it was hypothesized that: (1) rates of psychotic and substance use disorders would be higher among police cell detainees compared to the general population; (2) rates of mood and anxiety disorders in police cell detainees would be significantly higher than in the general population; and (3) that there would be a significant association between the presence of mental illnesses and the number of unmet needs reported by the detainees.
Methods
Participants
Participants were recruited from two police stations in metropolitan Melbourne, Australia. Melbourne is a large multicultural city with a population of just under 3.9 million people [13]. These stations were selected on the basis of a study that investigated psychiatric symptoms amongst police cell detainees in nine police stations across Victoria, Australia [14]. The two busiest police stations were identified and selected for the current study to ensure adequate sample size. Attempts were made to recruit all people meeting the inclusion criteria: (1) being at least 18 years old and (2) having spent a minimum of 12 hours in detention before interview to adjust to the environment and/or stabilize if withdrawing from substances (unless transferred from another police cell). Potential participants were excluded if they were: (1) non-English speaking, due to difficulty in organizing an interpreter, (2) detained solely for public drunkenness and disorderliness, as these individuals are kept in custody until the police determine that they are sober enough to leave (usually around 4 h), (3) transferred from prison to attend a court hearing at the local Magistrate's Court, or, (4) repeat admissions (i.e. detained again for a different offence/matter) to the cells during the time of the study.
Procedure
Detainees were approached by the researcher at the completion of a standard health screen with a custodial nurse, where information about the project was provided. If the detainee had refused to attend the health screen, they were approached in the secure clinical interview room. If consent was given, measures were administered with participants completing the consent form upon their return to the cell block due to the practical logistics of completing interviews in a secure interview room. Separate consent was also sought for access to their mental health and police records.
Measures
The Structured Clinical Interview for DSM-IV-TR (Patient Edition) (SCID-IV) was used to assess mental disorders in the past month (current) [15]. The disorders evaluated were: mood, psychotic, substance use, anxiety, and eating disorders. Other disorders, such as somatoform and personality disorders were excluded due to time constraints. The SCID has been reported to be both a reliable and valid measure [16] and has been successfully used with offender populations [17].
The Camberwell Assessment of Need – Forensic Short Version (CANFOR-S) was used to measure individual needs across 25 common domains, considering both needs that are met by current interventions and those that remain unmet and ongoing problems despite any help being received [18,19]. Training was provided for the administration of the SCID-IV and CANFOR-S. All interviews were completed by one of the authors (G.B.), with discrepancies and ambiguities for individual items discussed and agreed upon with the other authors.
A standard coding sheet was developed to record general background characteristics such as gender, age, employment status, marital status and time spent in cells at the time of the study interview.
Formal contact histories with mental health services and the police
A state-wide public mental health database, the Client Management Interface – Operational Data Store (CMI-ODS), was consulted to obtain documented histories of contact with the public mental health system. This database is more commonly referred to as the Victorian Psychiatric Case Register (VPCR). The VPCR is one of the oldest and most comprehensive psychiatric case registers worldwide. It was established in 1961 as a purpose-built database that annually extracted data from an independent patient management system (Patient Management Information System) [20]. The VPCR covers all specialist mental health care in the public sector, except for specialist drug and alcohol services. Data regarding contact with public mental health services, admissions to public psychiatric hospitals and community treatment orders (CTO; these are outpatient involuntary treatments under the Mental Health Act) were extracted using three types of personal identifiers: name (first, middle and last), date of birth and gender. The VPCR, however, does not capture contacts with the private system, such as privately practising clinicians or general medical practitioners. It is now estimated that private clinicians account for 20% of all community mental health contacts, consisting primarily of people with high prevalence disorders (e.g. mood disorders) [21,22].
The Law Enforcement Assistance Program (LEAP) database, maintained by Victoria Police, was also consulted to obtain documented histories of all contacts with the police (as suspects, offenders and victims). Data were extracted from this database using the same personal identifiers listed above (name, date of birth and gender). Offences were coded using an adaptation of the Cormier-Lang system for quantifying criminal history [23]. This system was chosen as it was based on the Criminal Code of Canada which is based on British Common Law, as are the criminal codes of Australia. This system allowed multiple offences to be categorized according to the severity of the offence. The categories in order of severity were: homicide, sexual assault, violence, kidnapping, weapons offences, threats of violence, property damage, stalking, drug offences, deception offences, theft offences, breach of legal order and bad public behaviour. Full histories were extracted at the end of data collection in April 2009. Twenty-four of the participants did not consent to access their criminal records. Data on offences and charges were not available for those who did not participate.
Ethical considerations
Ethical approval was obtained from the Monash University Standing Committee on Ethics in Research involving Humans, the Victorian Government Department of Human Services Human Research Ethics Committee and the Victoria Police Human Research Ethics Committee. Detainees were fully informed of study requirements, limits to confidentiality, and were given a consent form and an explanatory statement. Interviews were conducted in secure clinical interview rooms without police presence.
Statistical analysis
Statistical Package for Social Sciences (SPSS) version 17 was used to characterize the sample, with chi-square tests and t-tests used to test for group differences. Participants were grouped according to those with and without mental illness by separating those that met and did not meet criteria for Axis-1 diagnoses, excluding substance use disorders. Estimated rates of psychotic disorders were compared to 1-month estimated rates from a community control sample [24], and estimated rates of mood, anxiety and substance use disorders were compared to 12-month rates from the most recent Australian household survey [25]. History of mental health contact with the public mental health system was compared with estimated rates obtained from a control sample using the same methodology [22]. Rates of disorders from the current study and estimated rates from these comparison samples were used to tabulate and then calculate odds ratios, with 95% confidence intervals determined using Miettinen's approach [26].
Results
Of 259 eligible detainees initially approached, 150 agreed to participate in the study, corresponding to a recruitment rate of 57.9%. Ninety-four (36.3%) detainees declined to participate, and 15 (5.8%) detainees started the interview but did not complete assessments due to being taken to court and released. A further 60 detainees were not approached as police requested not to approach due to unstable mood and/or behaviour, or where the detainee was taken to court and released. There were no significant differences between consenters and refusers according to age or gender (p = 0.14 and p = 0.74 respectively).
Background and self-reported clinical characteristics
As indicated in Table 1, the mean age of participants was 30.4 years (SD = 8.95). Eight participants (5.4%) identified themselves as being of Indigenous Australian descent. Overall, participants had spent an average of 32.1 hours in the police cells at the time of the interview (SD = 24.55; median: 23.5; range: 3–144 hours). The most commonly reported lifetime medical illnesses for the participants were: mental illnesses (e.g., depression, anxiety, and psychosis), broken bones/head injuries, and hospitalizations/operations.
Demographic and self-reported clinical characteristics of sample
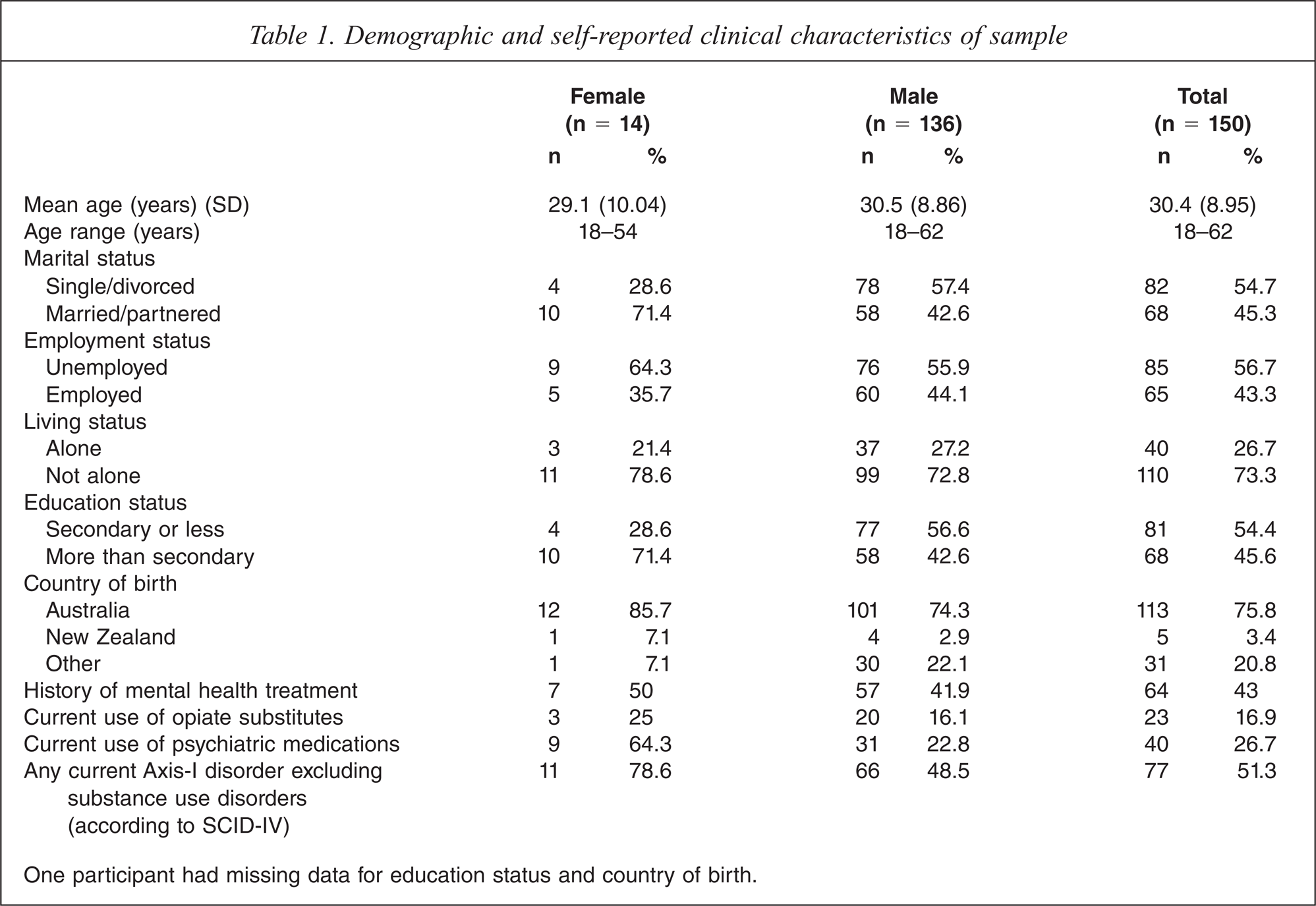
One participant had missing data for education status and country of birth.
Formal police contact
The offences that led to arrest at the time of this study were mainly non-violent (n = 88, 69.8%), such as obtaining property by deception, failing to answer bail, and theft. Violent offences, including making threats to kill, threatening to inflict serious injury, and recklessly causing serious injury had been committed by 38 of the participants (30.2%). The majority of the sample had an offence history (n = 121, 96%), of whom two thirds (n = 86, 68.6%) had committed violent offences.
Formal psychiatric history
Over half the sample (n = 69, 54.8%) had been registered with a mental health service according to the VPCR database at some point during their lives, a slightly higher proportion compared to self-reported data (n = 64, 43%). The mean number of contacts was positively skewed at 146.98 (SD = 273.10; median: 39; range: 1–1482). Thirty-two (25.4%) had been admitted on at least one occasion to a psychiatric hospital (mean = 4.16; SD = 5.03; median: 2; range: 1–25). Eleven (8.7%) of the participants had previously been on a community treatment order (CTO). Of these, eight (72.7%) participants had completed a CTO, 7 (63.6%) participants had a CTO revoked, four (36.4%) had a CTO extended, and two (18.2%) participants had an ongoing CTO.
Psychopathology
According to the SCID-IV, three-quarters of the sample (n = 114, 76%) met diagnostic criteria for at least one disorder (see Table 2). Substance dependence disorders were the most common, followed by mood disorders. Women were more likely than men to be diagnosed with anxiety disorders (χ2 = 7.33, p = 0.007) and mood disorders (χ2 = 9.57, p = 0.002). A third (51, 34%) were diagnosed with both mental and substance use disorders.
Comparisons between police cell detainees and the general population: Rates of psychiatric disorders, odds ratios and 95% confidence intervals
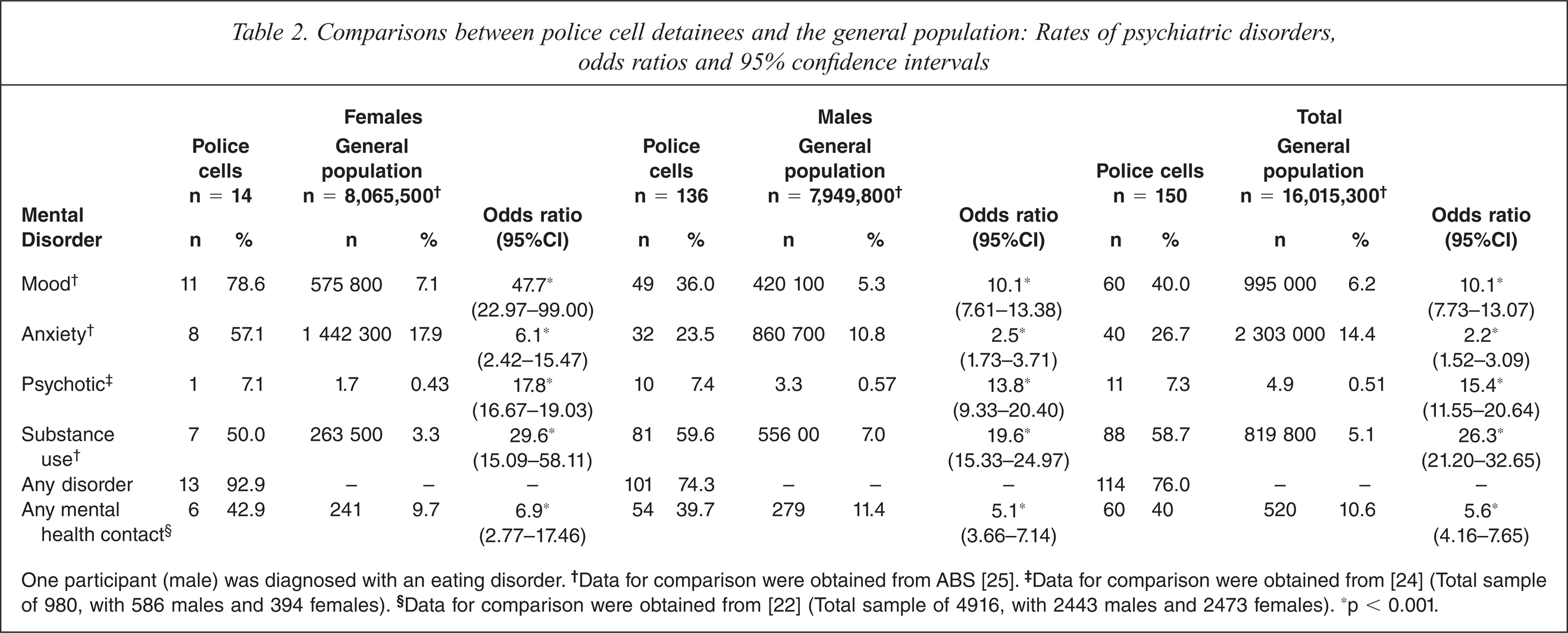
One participant (male) was diagnosed with an eating disorder. †Data for comparison were obtained from ABS [25]. ‡Data for comparison were obtained from [24] (Total sample of 980, with 586 males and 394 females). §Data for comparison were obtained from [22] (Total sample of 4916, with 2443 males and 2473 females). ∗p < 0.001.
Overall, the most common disorders diagnosed were major depression (n = 48, 32%), alcohol dependence (n = 32, 21.3%), opioid dependence (n = 32, 21.3%), post-traumatic stress disorder (n = 20, 13.3%), schizophrenia (n = 4, 2.7%) and schizoaffective disorder (n = 4, 2.7%). The other psychotic disorders diagnosed were psychotic disorder NOS (n = 2, 1.3%) and substance induced psychotic disorder (n = 1, 0.7%).
The chances of meeting diagnostic criteria were significantly higher for the current sample as compared to the general population for all psychiatric disorders. For example, the odds of meeting diagnostic criteria for psychotic disorders was 15.4 times higher (95%CI = 11.55–20.64, p < 0.001) in the current sample than in the general population. For men, the odds were highest for substance use disorders (OR = 19.57; 95%CI = 15.33 – 24.97, p < 0.001), while for women, the odds were highest for mood disorders (OR = 47.69; 95%CI = 22.97–99.00, p < 0.001) (see Table 2).
Individual needs
Participants reported having an average of 4.91 needs of a possible 25 needs (SD = 3.54); a large proportion of which were considered to be unmet (M = 3.06, SD = 2.71), thus representing ongoing difficulties for the participants. The most commonly presenting needs reported by participants were benefits (n = 75, 58.1%), accommodation (n = 75, 57.7%), and money (n = 69, 53.5%). The most common unmet needs reported were money (n = 62, 48.1%), company (n = 40, 31%), daytime activities (n = 40, 30.8%), drugs (n = 40, 30.8%), and intimate relationships (n = 39, 30.2%).
Those who met diagnostic criteria for a mental illness had a significantly higher number of needs overall (t(114.23) = −5.51, p < 0.001) and unmet needs (t(110.26) = −5.07, p < 0.001) compared to those without a mental illness (see Table 3), but the profile of needs between the mentally ill and those without mental illness were similar. That being said, those with a mental illness presented with unique unmet needs in two domains: psychological distress and safety to self. That is, more than half (n = 33, 51.6%) of those with a SCID diagnosis presented with unmet needs for psychological distress (compared to n = 4, 6.1% of those without mental illness), and one in four (n = 17, 26.6%) of those with mental illness presented with unmet needs in regard to safety to self (as compared to n = 1, 1.5% of those without mental illness). There were no differences in the presence of needs between different diagnostic groups.
Comparison of total and unmet needs between mentally ill and non-mentally ill
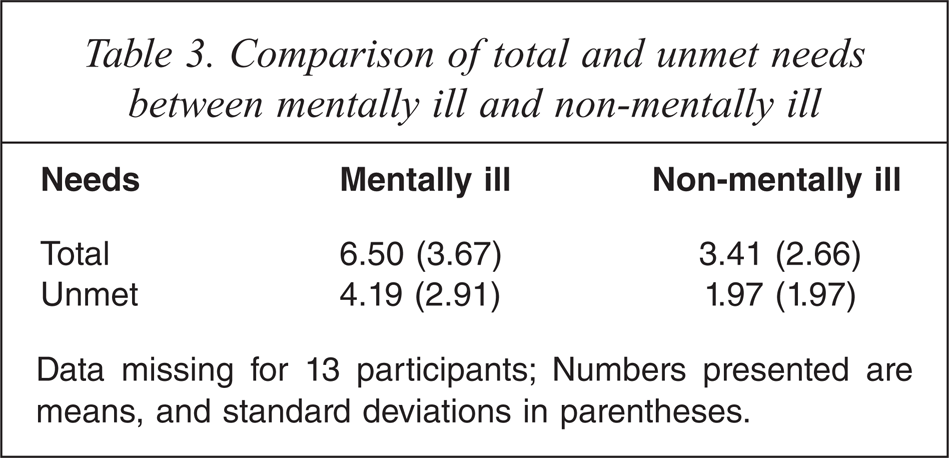
Data missing for 13 participants; Numbers presented are means, and standard deviations in parentheses.
Discussion
The current study found that one quarter of police cell detainees had a prior admission to a psychiatric hospital and that three quarters met the DSM-IV-TR diagnostic criteria for at least one Axis-I disorder in the month prior to the study interview. One third met diagnostic criteria for both a mental illness and a substance use disorder. Consistent with community surveys of mental health [27], substance use disorders and mood disorders were the most frequently seen psychiatric disorders.
The first and second hypothesis, that rates of psychotic, substance use, mood and anxiety disorders would be significantly higher among those detained in police cells as compared to those in the community, was supported. Results of the current study suggested that rates were between 2 and 26 times higher among detainees as compared to the general population. This was evident across all of the diagnostic category types and was consistent with high rates of mental disorder found among prisoners [2]. Indeed, rates of disorders from the current study were higher when compared to sentenced prisoners [17] and similar to a remand population [2]. The high rates of mental disorders, coupled with the deleterious effect of the police cell environment [7], such as the lack of basic facilities and services and the substandard conditions of police cells [11], has the net effect of compounding the suffering experienced by people with mental illnesses in police custody.
The difficulties experienced by those with a mental illness were further demonstrated by the finding that they reported higher total and unmet needs as compared to those without mental illness, supporting the third hypothesis. Moreover, individuals experiencing mental illness had a higher proportion of ongoing difficulties in the areas of psychological distress and suicidal concerns than those without a mental illness. These suicidal concerns, together with the stresses of being held in police custody, such as the impending legal proceedings and the restricted family visiting times, can increase the vulnerability of detainees experiencing mental illness. The extent to which psychological distress and suicidal concerns are related to substance abuse, mental illness or the police cell environment remains unclear, but is the subject of a separate paper currently under review (details available from the authors). The fact that there was a high level of unmet need in social and welfare domains amongst this sample, particularly for those experiencing mental illness, suggests the need for close collaborations between mental health, social and welfare services in the community to better address these needs.
These findings are in line with previous studies [10] and suggest that of a group of people coming into contact with police through their criminal offending, those with a mental illness are disproportionately represented and are particularly vulnerable in police custody. These findings have significant clinical implications for those responsible for providing psychiatric services to the police cell population, and suggest that there is a pressing need to evaluate standardized screening tools for mental disorders to identify those in need of further assessment and treatment. Currently, some jurisdictions use detailed assessment tools (albeit non-standardized) to help identify detainees with mental illnesses, while others have no formal screening instrument at all [28]. While it may not be possible to conduct comprehensive mental heath assessments with every person coming into police cells, use of an effective screening tool can facilitate the identification of those who may require comprehensive medical and/or psychological evaluation and perhaps diversion into treatment services [28,29]. Effective screening of mental illnesses in police cells could also assist to identify and re-engage those individuals who may have lost contact with their health care providers [30,31], and highlight the need for effective linkages between criminal justice and community-based care [32]. While the use of standardized screening tools in police custody may lead to better detection of those experiencing mental illness, it is also unavoidable that this process will be over-inclusive and identify some who may be regarded as false positives. Therefore, in a very much more practical sense, this initial screening would need to be followed by a second tier triage assessment to further refine and prioritize those in most need of treatment [33,34].
The results from the current study make a valuable contribution to our knowledge of mental illness among a sample of arrestees in Australia. This is because they highlight that providing treatment for this population in the community has far reaching complexities. If their needs were to be considered more specifically, then resources could be targeted that address the key challenges facing police cell detainees. The most common unmet needs were found to be in broad life domains, such as money, company, daytime activities, drugs and intimate relationships. These unmet needs, intertwined with high rates of mental illness and substance use problems, represented major ongoing difficulties from the perspective of the detainees; some of which have been highlighted as risk factors for criminal offending [35]. These results confirm the need to further develop and strengthen functional interagency collaborations across the criminal justice, health and social systems that provide a range of targeted and concerted services that meet the consumer's individual needs [36].
By way of example, one participant in this study reported ongoing problems with depression, substance use problems, budgeting money and paying bills and occupational difficulties. As this detainee was due for release on bail, one potentially viable option may be for an out-reach service worker from the local area mental health service to make contact with the detainee in the police cell to help case-manage an effective transition back to the community. However, given the often high levels of non-compliance amongst this population and their generally poor levels of engagement with services, it may be necessary to consider an intense case-management model of working, such as the use of assertive community treatment teams. These teams, common in general mental health services, may help contribute to better outcomes for detainees [37], especially when complemented with additional criminal justice components [38]. The development of such an arrangement is clearly not without substantial service provision implications. Given the sheer breadth and diversity of needs representing ongoing challenges for the detainees, a number of elements would need to be set in place, such as a level of information sharing across systems, adequate services in the community, and an integration of services across the varied systems and agencies [39]. Whilst such an integrated approach is not without its complexities, not least of which would be the initial financial burden and manpower logistics, it would serve to improve the appropriate identification of the complex needs of this vulnerable population, facilitate access to appropriate community services and supports, and thereby contribute to better health-related outcomes for these additionally vulnerable groups. Study findings also reinforced the additional considerations required for women who are being held in police custody, especially in relation to their general medical and psychiatric treatment needs. Further, more specialized service responses may also be indicated for this group.
A number of limitations must be noted. It may be possible that exclusion of those brought in for public drunkenness may have biased the sample. The state of Victoria is one of the last states to decriminalize public drunkenness, so efforts were made to recruit a sample representative of all states and territories [40]. In fact, the exclusion of these individuals may have led to an underestimate of the prevalence of mental disorders as they are likely to have co-morbid psychiatric and substance use disorders, thus further highlighting the potential importance of the current study findings. A further limitation of the study was the difficulty in recruiting a representative sample of detainees. It must be considered that the generalizability of the results may have been limited due to the large number of individuals who declined to participate or were unavailable due to police decision making. However, support for the generalizability of the study findings was demonstrated in that key demographic characteristics were broadly similar to other studies of police cell detainees with higher consent rates [8,41]. It must also be considered that selection of the two busiest inner city sites may have posed a selection bias. A further limitation concerns the inclusion of a limited number of psychiatric conditions in the assessment interview. Limits due to time, capacity of the detainees and location of the interviews precluded a more thorough or detailed assessment. For example, it is arguably clear that future research should investigate levels of acquired brain injury in this population, as there is emerging evidence that there is a relatively high prevalence of brain injury in offender populations [42,43]. Such findings will have further implications for health care providers, such as screening, assessment and service provision. Finally, while it may have been more appropriate to compare rates of mental disorders from the current sample to a similarly disadvantaged group from the community, they were compared with rates from the general population as they provided the best estimates currently available.
In conclusion, the current study highlights the significant psychiatric morbidity found in the police cell population, and the pressing need to evaluate standardized screening tools for mental illnesses to provide timely access to assessment and treatment services. Such recommendations cannot be taken lightly, not least because of the additional burden this kind of service overhaul would place on the police and health care providers. Any procedural changes can and would require substantial planning and investment from both criminal justice and mental health systems. However, exactly this kind of functional interagency collaboration needs to be developed across government systems and agencies in order to better meet individual needs and contribute to improved health and justice related outcomes.
Footnotes
Acknowledgements
The research team comprised James Ogloff, Stuart Thomas, Paul Mullen, Trish Martin, Jonathan Clough, Christine Tye, Ashley Dickinson and Ken Lay. We also acknowledge the project managers Stefan Luebbers and Lisa Warren, and the input of Leanne Sargent, David Bradley and David Ballek at Victoria Police. We thank the participants for giving us their time in a difficult circumstance, police officers for making these interviews possible and custodial nurses for their operational guidance.