
Abstract
As a method of intervention in the management of aggressive and disturbed behaviour of psychiatric patients, seclusion replaced mechanical restraints in the early nineteenth century [1, 2] and currently continues to be used worldwide [3]. Most published information regarding its use is from the USA and the UK but we note one significant Australasian study [4]. Yet, there is little research on the effectiveness of seclusion or on viable other alternatives [5–7].
There are a number of definitions of seclusion in the literature [1, 8–10]. For example, it has been defined as ‘the supervised confinement of a patient specifically placed alone in a locked room for a period at any time of the day or night for the protection of patient, staff or others from serious harm’ [9].
Several authors have discussed the indications or reasons for initiating seclusion [1, 11–17]. Prevention of harm to self or others has been reported as the primary indication for seclusion [18], other reported indications are much more controversial and include prevention of damage to property, disruptive or inappropriate behaviour, and suicidal or self-injurious behaviour. Generally, seclusion is seen by many as a measure of last resort when there are no effective alternatives.
It is not possible to directly compare seclusion practices due to the variations in definition, methods, setting and population studied in the different reports. It is its custodial nature that provokes much of the controversy and ethical debate. It is not surprising therefore that consumer advocates and some investigators are against its use in modern psychiatric care [19, 20], while others consider it as a necessary intervention to manage or contain disturbed behaviour [21–25].
In a review of relevant literature, which did not make a clear distinction between seclusion and physical restraint, Fisher [18] concluded that both are effective in preventing injury and reducing agitation.
This study examined prospectively the use of seclusion over a 9-month period in a 54-bed general adult acute psychiatric unit in the Henry Bennett Centre. It is located within Waikato Hospital and serves a population of 312 918 people of which about 21% are Maori. The
Henry Bennett Centre provides additional, but separate, forensic psychogeriatric and rehabilitation services. Seclusion is carried out in a low stimulus area which has seclusion rooms within the Intensive Psychiatric Care Unit (IPCU). The IPCU is physically locked off from the two adult acute wards but the care is fully integrated in the sense that the same key staff are responsible for the patients continuing care in either setting. Most acute patients are admitted directly to their relevant wards. Only those requiring intensive psychiatric care are transferred to the IPCU. This study was aimed at quantifying the use of seclusion, and establishing any significant correlations between specific demographic characteristics and the use of seclusion. Seclusion is defined in this study as ‘the placement of a patient in a locked room alone at any time during hospitalization’.
Method
For all newly admitted patients requiring seclusion over the study period (March 2000 to November 2000) information on aggressive behaviour using Overt Aggression Scale (OAS) [26], ICD-10 diagnosis and other characteristics of patients and details of each seclusion episode were obtained. Specific seclusion information included reasons for and the duration of seclusion, patterns and timing. Characteristics of patients included ethnicity, gender, age, marital status, length of hospital stay and the number of previous admissions. All patients admitted, over the same period but who had not been secluded, made up the comparison group. This study (audit) was done as part of services quality assurance activities, with the emphasis on feedback of the results to those involved. Hence no specific consent was sought. All of the information collected was seen as relevant to good quality management of patients. The monitoring of seclusion levels is an ongoing service performance indicator.
Statistical tests used were the chi-squared and t-tests associated with group comparisons and linear or logistic regression.
Results
Of the 539 patients admitted to the general adult unit during the study period, 84 (16%) were secluded in 129 seclusion episodes. Table 1 shows the frequency of seclusion episodes and patient characteristics.
Admitted patient demographic and psychiatric characteristics.
Analysis of the use of seclusion by gender and race revealed significant differences. Males accounted for 80% of episodes of seclusion with 23% of admitted males but only 7% of females secluded at least once. One male patient was secluded on 10 occasions. Overall 20% of Maori patients, 22% of other non-European and only 11% of European patients were secluded. These differences were statistically significant.
The age of the secluded and never-secluded groups was similar (mean 34 and 35 years, respectively).
Table 2 summarizes characteristics of seclusion events. Eighty-eight (67%) of the seclusion events were initiated in the first week of the patient's admission. Fifty-two per cent were initiated during the evening shift and 29% and 19% during day and night shifts, respectively.
Characteristics of seclusion events
The mean time spent in seclusion was approximately 14 hours (median 14; minimum, 0.67, maximum, 100 hours). The mean duration of seclusion initiated during the day shift was comparatively longer (21 hours) compared to 15 and 12 hours for evening and night shifts, respectively. Most (74%) of the patients in the secluded group were secluded only once. Thirteen per cent (11 patients) twice, 13% (11 patients) more than three times, and 6% (5 patients) were secluded four or more times. Figure 1 shows length of seclusion events.
Length of seclusion events.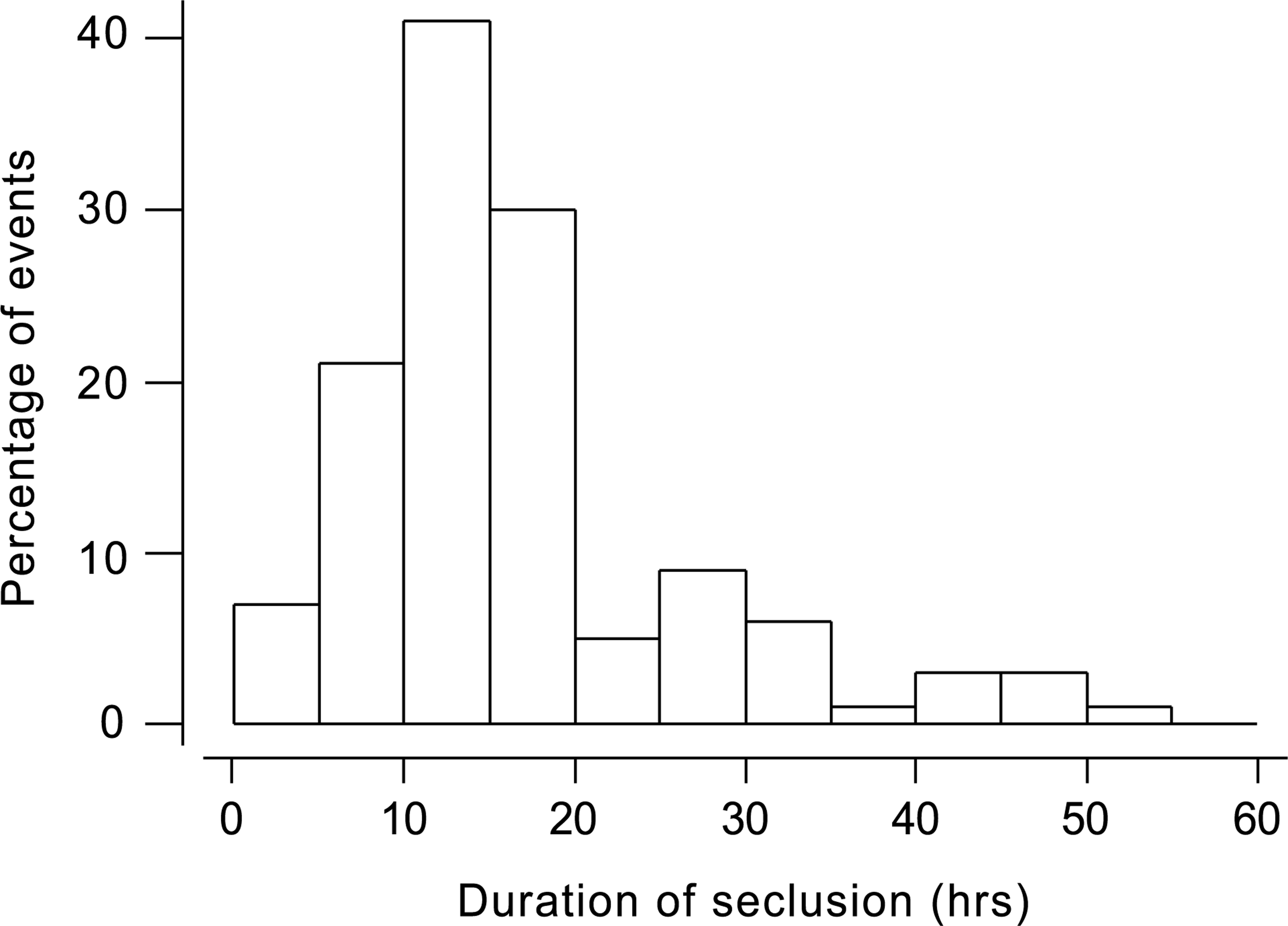
Patients who required seclusion had a significantly longer total length of stay (median 14 days) than the non-secluded (median 7 days). There was no strong association between number of previous admissions and seclusion rate.
Thirty per cent of patients diagnosed with schizophrenia, bipolar, or substance abuse were secluded, compared with fewer than 10% in other categories. However, because of the diagnostic distribution of all admissions, schizophrenia accounted for 48%, bipolar affective disorder 27% and substance abuse 14% of the total number secluded.
Among reasons for seclusion, threats of violence involving staff were the most frequently cited and accounted for 55% of all episodes; actual violence to staff accounted for 24%; threats of violence to other patients was 5%; and to property, 2% while rates of actual violence to other patients and property were 9% and 12%, respectively. Other reasons, for example, threats to other people or disorganized or agitated behaviour accounted for 26%. Multiple reasons were recorded in 10 seclusion episodes.
In addition to seclusion, other forms of intervention were used for 69 (54%) episodes. These include talking and/or holding the patient, immediate administration of medication either orally or intramuscularly, time out and attention for injury.
Restraint was used in association with 35 (27%) of the seclusion episodes. The form of restraint used was in the form of physically holding (restraining) the patient by nursing staff specially trained in using calming and restraint techniques. In 79 cases (61%) additional neuroleptic medication was given as required (prescribed PRN). Medication was not given in 44 (34%) episodes. There was no relationship between the use of psychotropic medication and other factors such as sex, race, diagnosis, OAS rating, or duration of seclusion. Duration of seclusion did not appear to be related to the OAS score.
Discussion
This study provides further information concerning the use of seclusion in one, busy, acute general adult psychiatric unit. Other characteristics of the Waikato Mental Health Service have been reported elsewhere [27]. Most previous studies could be criticised for their retrospective nature. The prospective design of this study and the setting choice, which aimed at sampling a more representative general adult psychiatric group, may have improved its validity and added to its inferential value.
Previously reported rates of seclusion vary widely between 4% and 66% [1]. This variation between studies may be related to differences in methods, setting and populations. Staff attitude and experience may also be important factor [15]. The seclusion rate in this sample (16%) is considerably higher than those reported by some authors [11, 15, 28], but lower than others [22, 23, 29, 30]. Oldham et al. [13] reported a somewhat similar seclusion rate of 18%. Notably, most of those studies were 15 or more years ago.
Our finding that more males than females were secluded is consistent with other reports. The finding that Maori and other non-European patients are more likely to be secluded than European patients is difficult to explain but may reflect more severe disturbances or psychopathology in the non-European patients or suggests that non-European patients may be selectively perceived as more dangerous. Perceived danger may be related to stereotype or bias and is more likely to be responded to in pre-emptive or defensive ways by the staff. That is also consistent with recent New Zealand findings on prescribed neuroleptic drug dose [Wheeler et al. unpublished data, 2000]. Ethnic variations in seclusion have also been noted in some other studies [11, 31].
In contemporary New Zealand, Maori patients already have a higher rate of admissions particularly for schizophrenia and substance abuse, but are less often diagnosed with depression compared with Europeans. This may be a contributory factor to their apparent higher rate of seclusion.
It is generally agreed that seclusion should be used for the least amount of time as possible. The average duration of seclusion reported by some previous studies varies widely between 2.5 hours and 25.6 hours [8]. However, it would seem that duration of seclusion in our study (median 14 hours) is somewhat long. Duration of seclusion may generally be related to the hospital setting and also to the patients and staff involved. In our study there was no relationship between duration of seclusion and reasons for seclusion including aggressive behaviour as measured by OAS rating. This is a matter for ongoing inspection, discussion and monitoring within the service.
The mean length of hospitalization for patients who were secluded was significantly greater than that of patients who were never secluded. Prolonged hospitalization of secluded patients and lack of association with the number of previous admissions suggest that acuity of the disorder rather than chronicity may be relevant to seclusion. Neither age nor marital status was significant in distinguishing seclusion from non-seclusion patients.
Our finding that about two-thirds of the seclusion events were initiated in the first week of the patient's admission is consistent with the literature and is most likely due to a greater degree of acuity in the patient. Furthermore, there is significant diurnal variation, with 52% of seclusion episodes occurring during evening shift and 29% and 19% during day and night shifts respectively. At night all patients are in single rooms and many are asleep, both factors presumably limiting the need for more formal seclusion. Anxieties associated with still ambulant patients but lower staffing levels may explain the high rates of seclusion initiation in the evenings. The higher threshold for initiating seclusion on day shift may explain the associated longer mean duration of those episodes. In addition to diurnal variation, peaks in the frequency of seclusion initiation occurred at certain times. One between 16.00 hours and 18.00 hours, and the other around 22.00 hours. The former coincides with the change of shift (end of day shift and hand-over to evening shift) and medication time while the latter with bed time where patients would be directed to switch off the television and radios etc. It can be speculated that at these times there may be increased verbal interaction, confrontation and or tension between some staff and some patients. It is also possible that the number of staff members available to patients is lower than at any other time due to staff meeting (handover). Diurnal variations and peaks in the frequency of seclusion initiation suggest that seclusion may also be related to the hospital milieu.
It has been previously reported by some, but not all authors, that younger patients tend to be secluded more frequently [13, 15, 22, 23, 25]. We did not find an age correlation. Studies that have reported some age effect on seclusion have included adolescent patients. Patients in our study were exclusively adult, aged between 18 and 59 years. This could explain the lack of age correlation in our findings but it is also possible that age may not be a significant determinant of seclusion.
Diagnosis had a significant effect on whether a patient would be secluded. Patients with schizophrenia, mania and those with substance abuse tended to be secluded more frequently than others. Several studies have reported that persons with schizophrenia and mania are more likely to be secluded than others [13, 15, 22, 28], unlike our study, those failed to control for the disproportionate number of people with schizophrenia in the population studied. In our study, patients with a primary diagnosis of substance abuse involving mainly cannabis accounted for 12% of the seclusion episodes. It is worth mentioning that since personality disorders are not generally thought of as being legally incompetent, it was reassuring that none of these patients had seclusion forced upon them.
Threats of violence to staff, patients or property were the cited reason in 62% of the episodes and actual violence to the same three categories accounted for 45% of seclusion episodes. These figures indicate that seclusion was used mainly in association with risk of, or actual, violence. Under such circumstances there is high risk to self or others that would necessitate some form of intervention. Furthermore, in many countries such imminently dangerous situations would probably also provide the legal grounds for emergency intervention. However, whether it is appropriate to use seclusion as the main or only means of intervention is open to discussion. Even if this point is perfectly valid it would be difficult to justify the use of seclusion for prolonged periods or as part of a planned treatment. Even when seclusion is seen as removal of patients from the environment contributing to the disturbance, and as such may have some advantages particularly in the management of patients with learning disabilities [24], such intervention when applied to general adult psychiatric patients does not necessarily guarantee the restoration of the therapeutic environment [15]. Other reasons for seclusion included threats to other people or disorganized or agitated behaviour which was cited for 26% of cases. The possible contributions to seclusion rate of alternative management strategies could only be speculated upon. For example, the use of more intense specialling (one staff to one patient), alterations in ward milieu or staff attitudes. These are all subjects of further Waikato staff discussion and planning.
Footnotes
Acknowledgements
We thank the Waikato Mental Health hospital staff for their help.