
Abstract
Keywords
One of the most interesting intercultural findings of the recently published Te Rau Hinengaro: the New Zealand Mental Health Survey was the apparent high rate of bipolar disorder in M
Apart from substance use/abuse-related disorders, the single diagnostic category that had the greatest cultural variation was bipolar disorder, for which the apparent rate for M
The other large New Zealand mental health project funded by the National Mental Health Research and Development Strategy in recent years was the Casemix Outcome Study (CAOS) [4, 5]. That project, based on current service users, included particularly those with episodes of hospitalization during a 6 month period in 2002. The contribution of the CAOS project and other refereed publications reflecting on M
In particular, comparison by culture/ethnicity of those treated for bipolar disorder in the inpatient services during 2002 may give information to inform the debate necessary to understand the findings of Te Rau Hinengaro with regard to the apparent community prevalence of bipolar disorder. By comparing, between the different cultural/ethnic groups, more detailed, standardized, descriptions of their clinical phenomena during treated illness episodes we may better understand those apparent community prevalence findings. Particularly to elucidate whether the results do indeed represent a reliable and valid difference in the rates in different ethnic groups or reflect a lack of cultural sophistication in assigning diagnosis by the CIDI, or an even more conceptually global inadequacy in the definitions of the phenomenon underpinning psychiatric diagnoses in the context of different cultures [3, 6].
Our aim in this brief paper is to compare aspects of the clinical profiles of M
Method
In the CAOS project, information was collected on the costs of episodes of care, service user characteristics and aspects of services provided. A total of 19 239 episodes of care were studied. These were for both inpatients and community patients.
Incidence and prevalence figures cannot be extrapolated from these findings and applied to the general population because the participating services were simply those that volunteered, representing approximately one-third of those in New Zealand.
Among the patient characteristics reliably recorded was the profile of clinical psychopathology as reflected in the HoNOS [7, 8]. These HoNOS data give a reliable recording of the observations made on 12 particular items, for 96% of the service users who had an episode of care during that 6 month period.
HoNOS profiles are compared between two self-identified cultural groups: M
We looked at two categories: bipolar/manic and bipolar/depressed episodes. There were 407 episodes for the first and 3954 for the second.
Results
Data for the HoNOS items dealing with clinical psychiatric phenomena of the diagnosed manic patients are presented in Table 1, for the two ethnic groups. The mean ratings for self-harm and cognition in both ethnic groups do not reach clinically significant levels given that they are >1. Item 1, which summarizes behavioural features concerned particularly with overactivity, shows a clear difference between European and M
Selected HoNOS items for mania
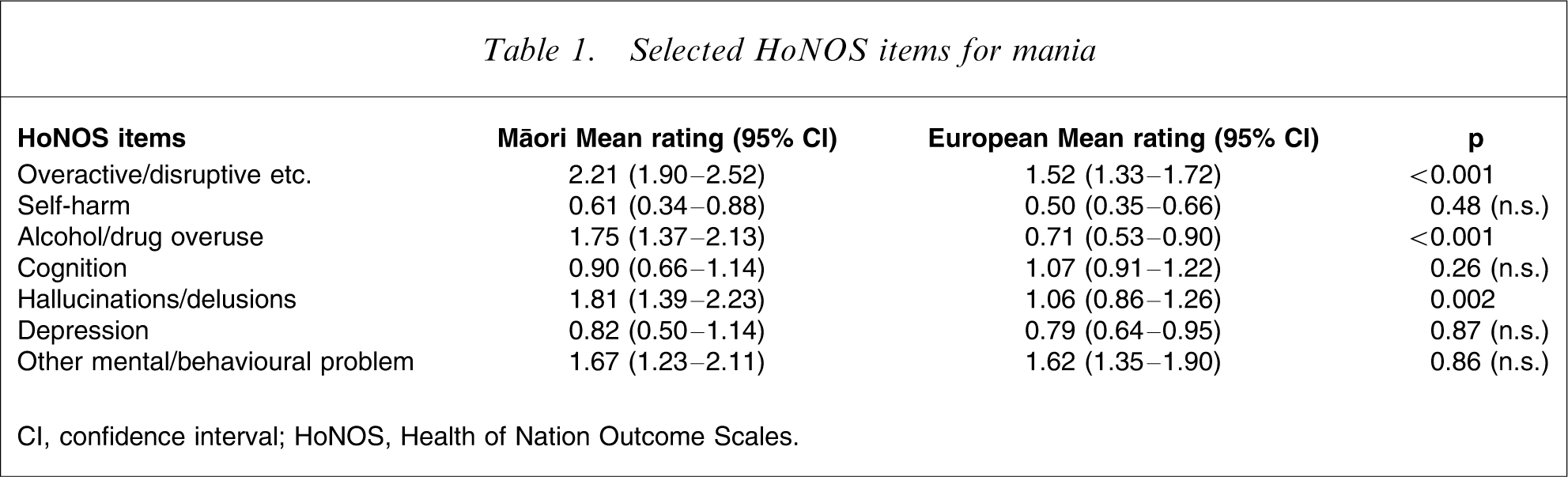
CI, confidence interval; HoNOS, Health of Nation Outcome Scales.
The ethnic differences for item 1 (overactivity) in either bipolar phases are illustrated in Figure 1. The same higher ratings for overactivity for M Mean Health of Nation Outcome Scales ratings for ‘overactive/disruptive’ in the two bipolar diagnostic groups.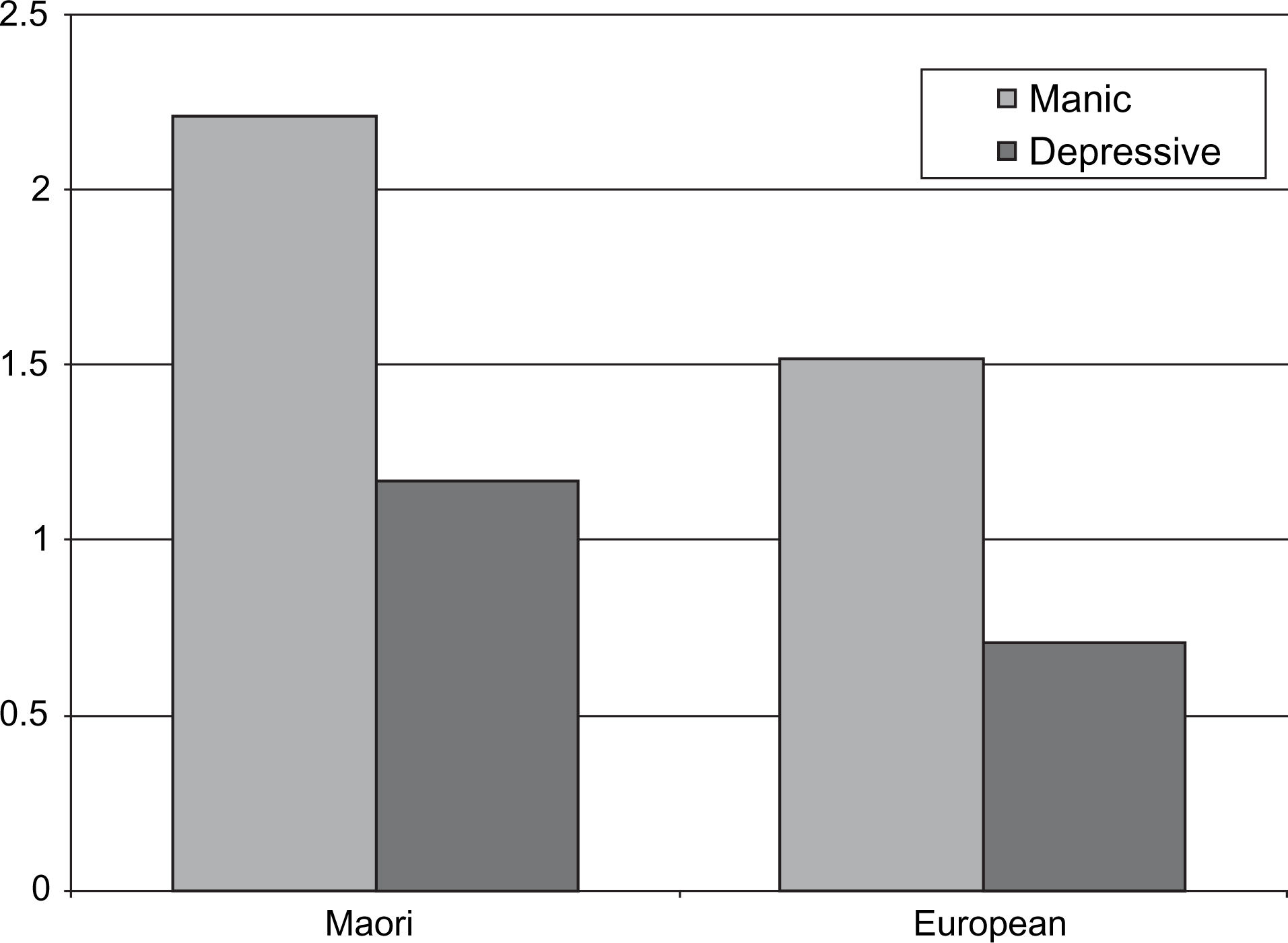
Selected HoNOS items for bipolar depression
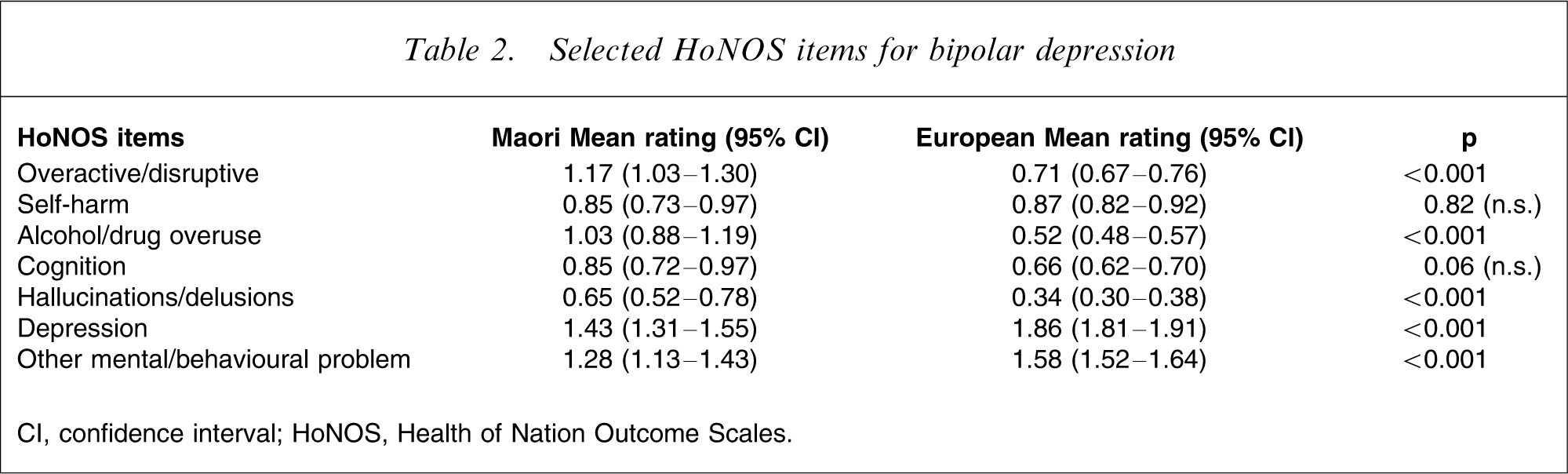
CI, confidence interval; HoNOS, Health of Nation Outcome Scales.
Discussion
Concerns about the mental health of Maori and also Pacific people have been highlighted in many publications [1, 2, 5, 6, 9]. Analysis of the full CAOS data has demonstrated that M
The findings of the more recent study Te Rau Hinengaro: the New Zealand Mental Health Survey[1, 2, 10] not only provide further information about the prevalence of mental illness in New Zealand but also seemed to confirm previous findings of higher rates of mental illness and severity among Maori and Pacific people, similar to the elevated rates in the UK ethnic minority groups [1, 2, 10, 11]. Those results, however, have attracted some debate and criticism [3, 12]. In particular, Jorm was concerned about diagnostic thresholds and proliferation of diagnoses in relation to the use of CIDI and the current categorical as compared with the dimensional diagnostic system [3]. Hickling et al. demonstrated that comparing cross-cultural and iso-cultural raters resulted in apparently similar prevalence rates but that the diagnostic groups were contributed to by different individuals [13].
Item 1 on the HoNOS examines problems with overactive, disruptive, agitated, or aggressive behaviour. Rating rules stipulate that all types of behaviour must be rated, regardless of intention, insight or awareness, and context must be considered. The rating rules are clear in terms of how specific behaviours should be rated but without considering possible causes of such behaviours.
The striking differences for item 1 (overactivity) in both bipolar phases are of interest. M
The findings on alcohol and drug usage are in the same directions for the service user (patient) group as in the community-based survey. The higher ratings for overactivity in the current patients could be seen as consistent with work on the use of neuroleptics in these New Zealand groups [14], and the rate of use of seclusion in a New Zealand inpatient unit [15]. This has also been noted for specific phenomena, such as hallucinations [16].
Those patients who contributed data to the CAOS study when in the depressed phase of a bipolar disorder show the same intercultural variation as for the pure manic patients, in particular, higher rates of overactivity and substance use/abuse and less display (or recognition) of depression.
Whether these are cultural variations in how depression or dysphoria are experienced or displayed lacks currently available proof, but must at least support the view of Jorm [3], and challenge the cross-cultural robustness of a nomothetic instrument such as the CIDI.
The CAOS data did not find any difference in the rates of diagnosis of bipolar disorder when examined by ethnicity/culture. Yet it is clear that the clinical profile of the M
Conclusions
Clinical profiles indicate that Maori patients in both categories are considered/perceived to be overactive. This is consistent with previous findings regarding use of seclusion and neuroleptic medications. It is possible that lay interviewers are picking up ethnically or culturally based activities, which allows the CIDI decision tree to generate the diagnoses of bipolar disorder. We believe that CIDI will not replace the experience and wisdom of psychiatrists who would normally consider the bigger picture when making such diagnoses. It is reasonable to conclude that there is a need to develop a culturally sensitive and robust assessment tool that can take into account cultural variation in symptom reporting, and the use of phenomenological constructs as would psychiatrists. When the distribution of diagnoses in mental health service users is less culturally idiosyncratic than in community research, we need to be confident we are comparing like with like, before accepting the findings as knowledge.