
Abstract
Keywords
Despite a considerable overlap in phenomenology, descriptive studies have indicated a broad range of symptomatic differences between unipolar and bipolar depression [1]. Somatic symptoms and atypical features (e.g. hypersomnia, hyperphagia or rejection sensitivity) are relatively common in bipolar depression, but weight loss is less common and episodes tend to be briefer [2]. Distinct characteristics of bipolar depression may pose a practical problem in assessing bipolar depression with regard to rating scales focused on the phenomenology of unipolar depression [3, 4].
In light of the need to assess the clinical characteristics of bipolar depression, Berk et al. developed the Bipolar Depression Rating Scale (BDRS), which contains 20 items on clinical variables associated with the depressive states of bipolar disorders [5]. The item structure of the BDRS was designed to cover mixed features and atypical symptoms. The depression items were strongly correlated with the 21-item Hamilton Depression Rating Scale (HAM-D) and Montgomery–Äsberg Depression Rating Scale (MADRS), thereby indicating the utility of the BDRS in assessing depressive symptomatology [5]. A statistically significant correlation between the YMRS and the mixed subscale was also observed. Hence, it is possible that the BDRS may serve as a useful tool in evaluating the effectiveness of therapeutic agents in treating bipolar depression.
Psychopathological studies on the continuity of psychosis have been conducted using the Positive And Negative Syndrome Scale (PANSS) [6], and both excitement and depression factors have been repeatedly identified in a widely accepted five-factor solution of the PANSS [7]. In this regard, affective component of the PANSS has been used as the outcome measures in clinical trials for bipolar disorders [8, 9]. In terms of the continuity of psychosis, assessing bipolar depression using affective components of the PANSS may provide additional information in bipolar depression [10].
Second-generation antipsychotics (SGAs) are widely used in managing all phases of bipolar disorders, regardless of the presence of psychotic symptoms [11]. Compared to patients with schizophrenia, patients with bipolar disorder have been reported to be more sensitive to antipsychotic treatment in terms of treatment-emergent adverse effects including extrapyramidal symptoms (EPS) [12]. In addition, despite the low risk of EPS associated with mood stabilizers, EPS have been observed in patients on long-term maintenance therapy with lithium or valproate [13]. Regardless of the type of SGAs, parkinsonian symptoms and akathisia frequently occurred in patients with bipolar disorders, thereby complicating mood status [14]. It has been also reported that the patients with akathisia may suffer from dysphoria and tension [15]. Thus, in order to evaluate the depressive states of bipolar patients receiving antipsychotic treatment, the effects of EPS on depressive symptoms should be considered [16].
In the present study, the overall objective was to explore whether the internal structure of the BDRS is suitable for assessing clinical characteristics of patients with bipolar depression receiving pharmacotherapy. Although the validation of the BDRS has already been performed [5], the utility of the BDRS is still of concern in relation to psychopathological characteristics and EPS.
Methods
Subjects
Subjects with bipolar disorder were recruited through clinical referral from the Bipolar Disorder Clinic at Seoul National University Hospital (SNUH). This study was in accordance with the latest version of the Declaration of Helsinki. The study procedures were described in detail and written informed consent was obtained before subjects participated in the study. The study protocol was reviewed and approved by the Institutional Review Board for SNUH. Sixty outpatients with DSM-IV bipolar I or II disorder, aged 19–61 years, meeting DSM-IV criteria for a major depressive episode were included in the study. Of these, 33 (55%) were male and 27 (45%) female. Patients with comorbid DSM-IV Axis I diagnosis or medical conditions were excluded. Patients were excluded if there was any evidence of severe cognitive impairment. Patients receiving non-psychiatric medications potentially affecting mood symptoms were also excluded (e.g. anti-hypertensives, steroids).
Measures and procedures
Depressive symptom measures
To evaluate the utility of the BDRS as a rating instrument for depressive symptoms, two observer-rated depression scales, the 17-item HAM-D [17] and the MADRS [18], and the depression subscale of the Positive and Negative Syndrome Scale (PANSS-D) were used.
The HAM-D was originally developed to assess the effectiveness of antidepressant treatment, and became the most widely used measure of depression severity for clinical trials of antidepressants or mood stabilizers [19]. The Korean version of the HAM-D showed good internal consistency (Cronbach's α = 0.76) and interrater reliability (r = 0.94, p < 0.001) [20].
The MADRS is a 10-item rating instrument developed for the assessment of treatment-induced change in depressive symptoms. Principal component analysis indicated a more uniform internal structure of the MADRS compared with the HAM-D [21]. The Cronbach's alpha of the Korean version of the MADRS was acceptable (α = 0.79). The total score of the Korean version of the MADRS significantly correlated with the total score of the Korean version of the HAM-D [22].
The PANSS is a 30-item, 7-point (1–7) rating instrument designed to assess schizophrenia symptoms [6], and the PANSS-D is often considered as one of the five main factors of the PANSS internal structure [23]. The PANSS-D is composed of four items: somatic concern (G1), anxiety (G2), guilt feeling (G3) and depression (G6). Significant correlation was observed in patients with schizophrenia between the PANSS-D and the HAM-D [24]. For the Korean version of the PANSS, the test–retest correlations of the three subscales in the PANSS ranged between 0.89 and 0.95, and the Cronbach's alpha for the positive, negative and general psychopathology was 0.73, 0.84 and 0.74, respectively. The factor analysis using the principal axis factoring produced five components: cognitive, excitement, depression, positive, and negative [25].
Manic symptom measures
To measure the severity of manic-like syndrome in patients with bipolar depression, the Young Mania Rating Scale (YMRS) [26] and the excitement subscale of the PANSS (PANSS-E) [27] were used.
The YMRS is the most widely used observer-rated rating scale in clinical trials of mania from children to adults [28, 29]. The Cronbach's alpha of the Korean version of the YMRS was acceptable (α = 0.73), and the discriminant function analysis showed that manic and non-manic patients were correctly discriminated (73.7%) by the Korean version of the YMRS [30].
The PANSS-E is composed of four items: excitement (P4), hostility (P7), uncooperativeness (G7), and poor impulse control (G14). The item structure of the PANSS-E was supported by confirmatory factor analysis. The change in the total score of the PANSS-E significantly correlated with the change in the total score of YMRS in patients with bipolar disorder [27].
EPS measure
Treatment-emergent EPS were assessed on the Drug-Induced Extrapyramidal Symptoms Scale (DIEPSS) combined rating scale quantifying the severity of drug-induced parkinsonism, akathisia, dystonia, and dyskinesia [31]. The DIEPSS is a nine-item, 5-point (0–4) rating instrument designed for the overall assessment of EPS in patients receiving psychopharmacotherapy. For the Korean version of the DIEPSS, the interrater reliability of the individual items was high in terms of the intraclass coefficient (0.76–0.96). The total or subscale scores of the Korean version of the DIEPSS were significantly correlated with the scores of the other EPS measures (Simpson–Angus Scale, Barnes Akathisia Rating Scale, and the Abnormal Involuntary Movement Scale; Spearman's ρ, 0.88–0.97) [32].
Procedures
All participants were interviewed by a psychiatrist (JSC, HJP or SHK), and one other trained researcher (HYY), using the BDRS, HAM-D, MADRS, PANSS-D, PANSS-E and YMRS. The investigators all received interrater reliability training in using all the rating scales, with outpatient interviews. The interrater reliability for six instruments, as determined by intraclass correlations, ranged from 0.84 to 0.95, and the test–retest correlations reached between 0.90 and 0.97. Data coding was performed by a trained researcher (HYY), who was blind to psychiatric treatment and patient identity, and the variables containing identity information were deleted prior to statistical analysis (JSC).
Statistical analysis
The demographic variables and the baseline scores of rating instruments were described and compared using χ2, Fisher exact, and t-tests, as appropriate. In order to measure the relationship between the scores of the rating instruments while controlling for the effects of treatment-emergent EPS, partial correlations were used.
In quantitative research, as is the case with most psychiatric rating instruments, the rating instruments with a large number of items often undergo one or more procedures of data reduction prior to data interpretation. Among various statistical techniques, either descriptive (exploratory) or analytical (confirmatory), hierarchical cluster analysis (HCA) and multidimensional scaling (MDS) can produce heuristic illustrations of the relationship between diverse items or rating instruments, giving useful information unattainable through the significance tests based on numerical summary measures [33–35].
The primary objective of HCA in the present study was to clarify the non-overlapping cluster structure of the BDRS items through agglomerative processes. During agglomerative processes, all the variables are successively combined into clusters, which maximize both internal homogeneity (within-cluster variation) and external heterogeneity (between-cluster variation) [36]. Because clinical data are prone to noise points disturbing hyperspherical cluster formation, Ward's method, which is designed to minimize the variance within clusters, and is advantageous in the conditions of cluster overlap over other agglomerative algorithms, was used as an agglomerative method of HCA. This method is based on the objective function known as the within-group sum of squares or the error sum of squares [37, 38]. In HCA with Ward's method, the emerging cluster is determined by the least increase of the sum of squared Euclidean distance, thereby reducing the information loss associated with cluster fusion.
In addition to the cluster structure produced by HCA, MDS was used to assess the geometric properties of cluster structure. Through a set of computational procedures, the degree of dissimilarity between two variables can be converted into the geometric distance between two points on the MDS map [39]. Although MDS is not probabilistic or deterministic, it can present a graphical display of the data structure, which is much easier to understand than a table of numbers [40]. In addition, MDS solutions have facilitated the visual exploration of the psychological structures by providing the most parsimonious model with the least possible dimensions [34]. By modelling variables as points in a geometric MDS space, the clusters can be compared with regard to essential properties including density, variance, shape, and separation; density is a thickness of variable swarm in a geometric space; variance is the degree of dispersion of the variables from the centre of the cluster; shape is the arrangement of variables in the space; separation is the degree of cluster overlap [37]. Because MDS solutions require that each dissimilarity value be precisely mapped onto its corresponding distance with the least possible dimensions, ‘errors of representation’ are inevitable in MDS models. Therefore, to select the optimal number of dimensions, the S-Stress level (Stress) is widely used as a badness-of-fit measure and the R-squared index (RSQ) as a goodness-of-fit measure, both of which range from 0 (perfect fit for the Stress; worst possible fit for the RSQ) to 1 (worst possible fit for the Stress; perfect fit for the RSQ). Stress < 0.2 or RSQ > 0.6 is generally acceptable in terms of the data interpretability and information loss [39, 41].
Results
Demographic and clinical characteristics
Subject characteristics
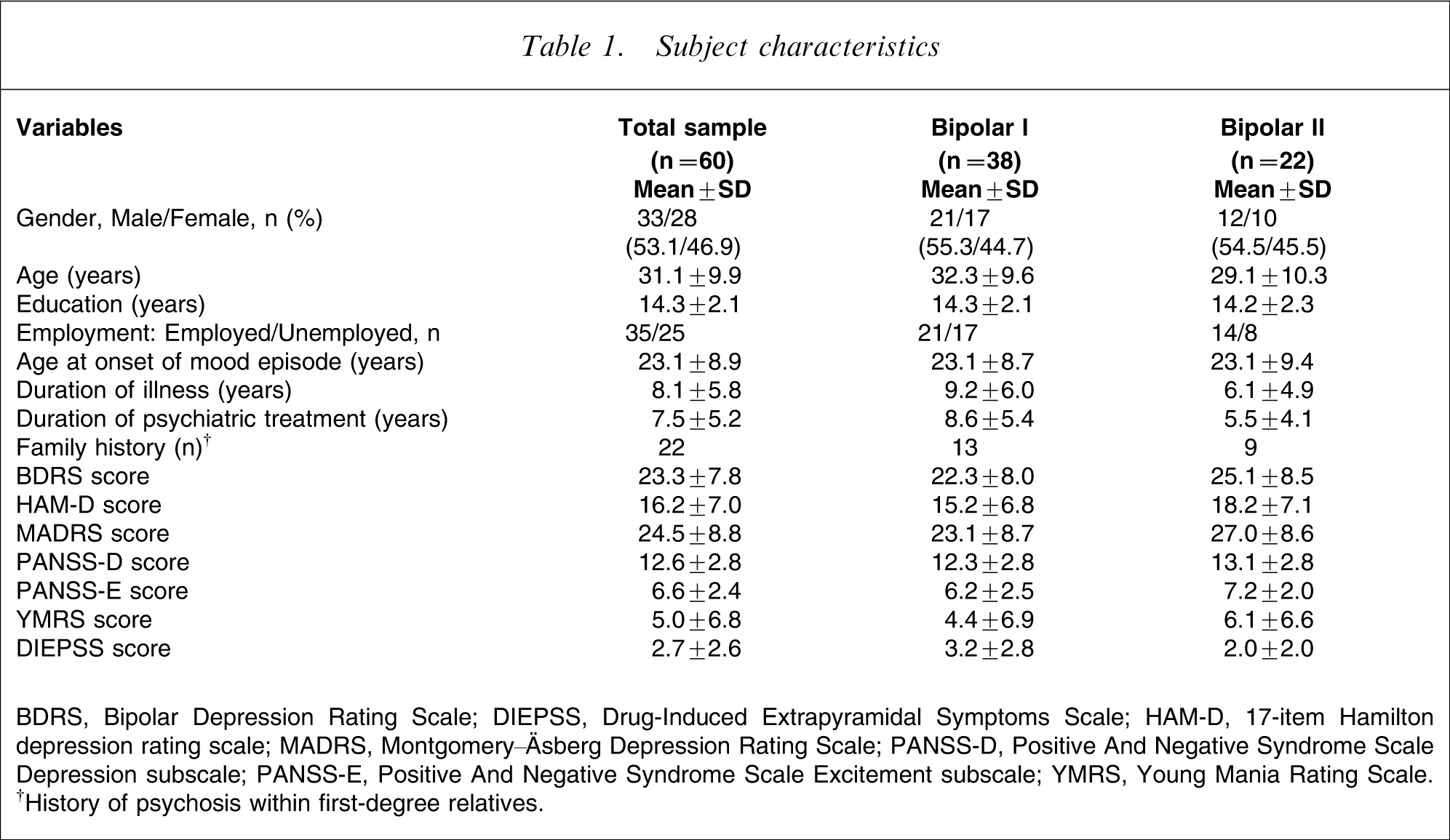
BDRS, Bipolar Depression Rating Scale; DIEPSS, Drug-Induced Extrapyramidal Symptoms Scale; HAM-D, 17-item Hamilton depression rating scale; MADRS, Montgomery–Äsberg Depression Rating Scale; PANSS-D, Positive And Negative Syndrome Scale Depression subscale; PANSS-E, Positive And Negative Syndrome Scale Excitement subscale; YMRS, Young Mania Rating Scale. †History of psychosis within first-degree relatives.
Cluster structure of the BDRS
As shown in Figure 1, the HCA with Ward's method indicated a two-cluster structure of the BDRS. The dendrogram depicts the successive pattern of cluster fusion. The level of dissimilarity between items is reflected on the horizontal axis. The first cluster includes 12 items of depressive symptoms similar to other depression rating scales (depressive symptom cluster). The second cluster includes eight mixed symptoms items (mixed symptom cluster). The overall cluster structure did not suggest the presence of an entropy group (i.e. a group of heterogeneous items), which may be detrimental to the parsimonious modelling of the BDRS.
Ward's method dendrogram, which depicts 20 items on the Bipolar Depression Rating Scale (n = 60).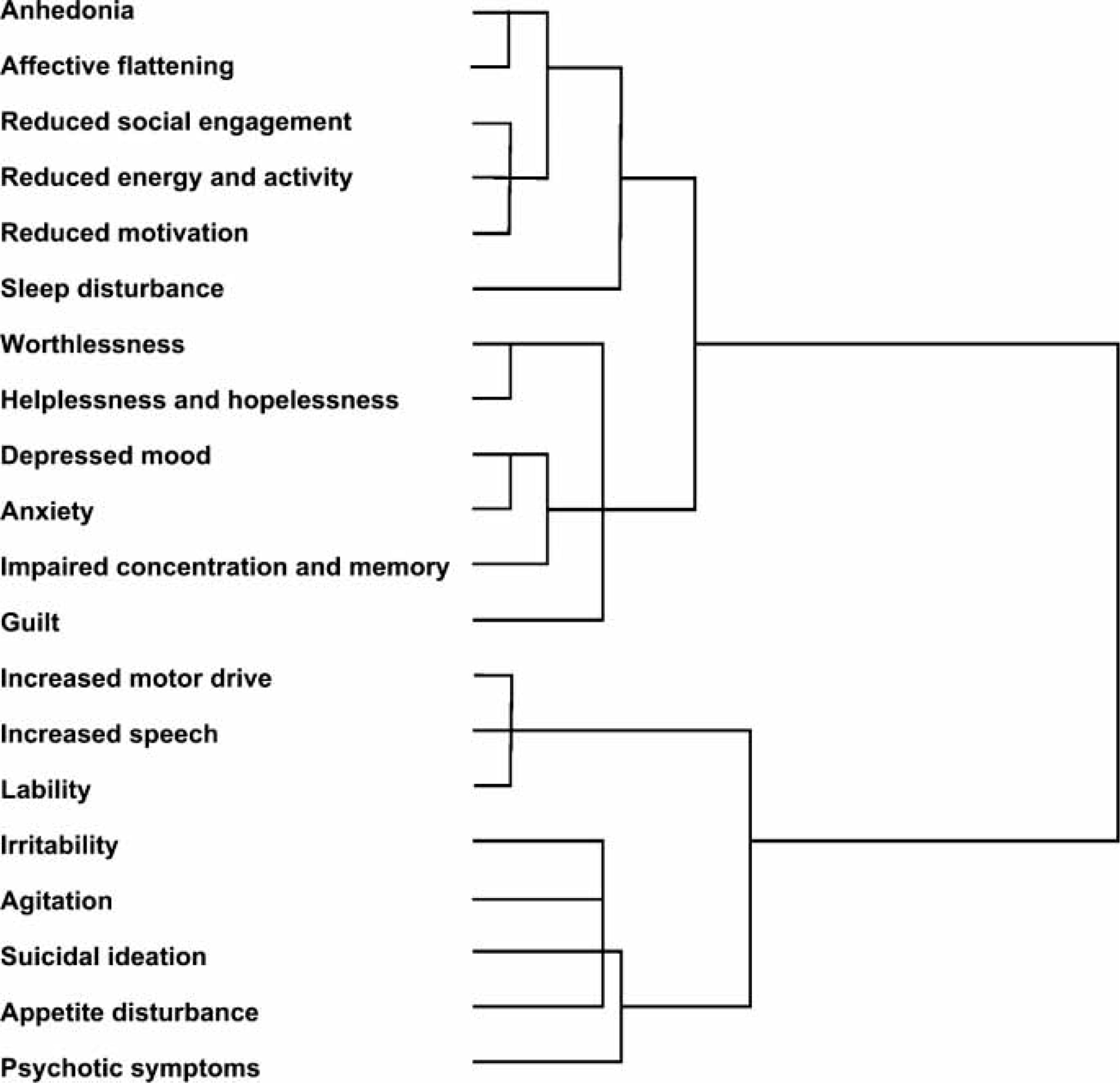
The geometric structure of the BDRS, as determined on MDS mapping, is shown in Figure 2. Model fit statistics (the Stress and RSQ values) supported a 2-D solution. Partitioning the MDS space according to the first dimension (dimension 1) was in accordance with the results of HCA with Ward's method. The second dimension (dimension 2) was not amenable to regional interpretation. In terms of cluster properties, the area of depressive symptom cluster showed a thicker swarm of item points in the MDS space compared to the area of mixed symptom cluster, and thus a higher degree of dispersion of the points from the cluster centre was associated with the area of mixed symptom cluster.
Two-dimensional representation of the relationship between 20 items of the Bipolar Depression Rating Scale from the sample of 60 patients with bipolar disorders. (•), depressive cluster; (○), mixed cluster. RSQ, R-squared index.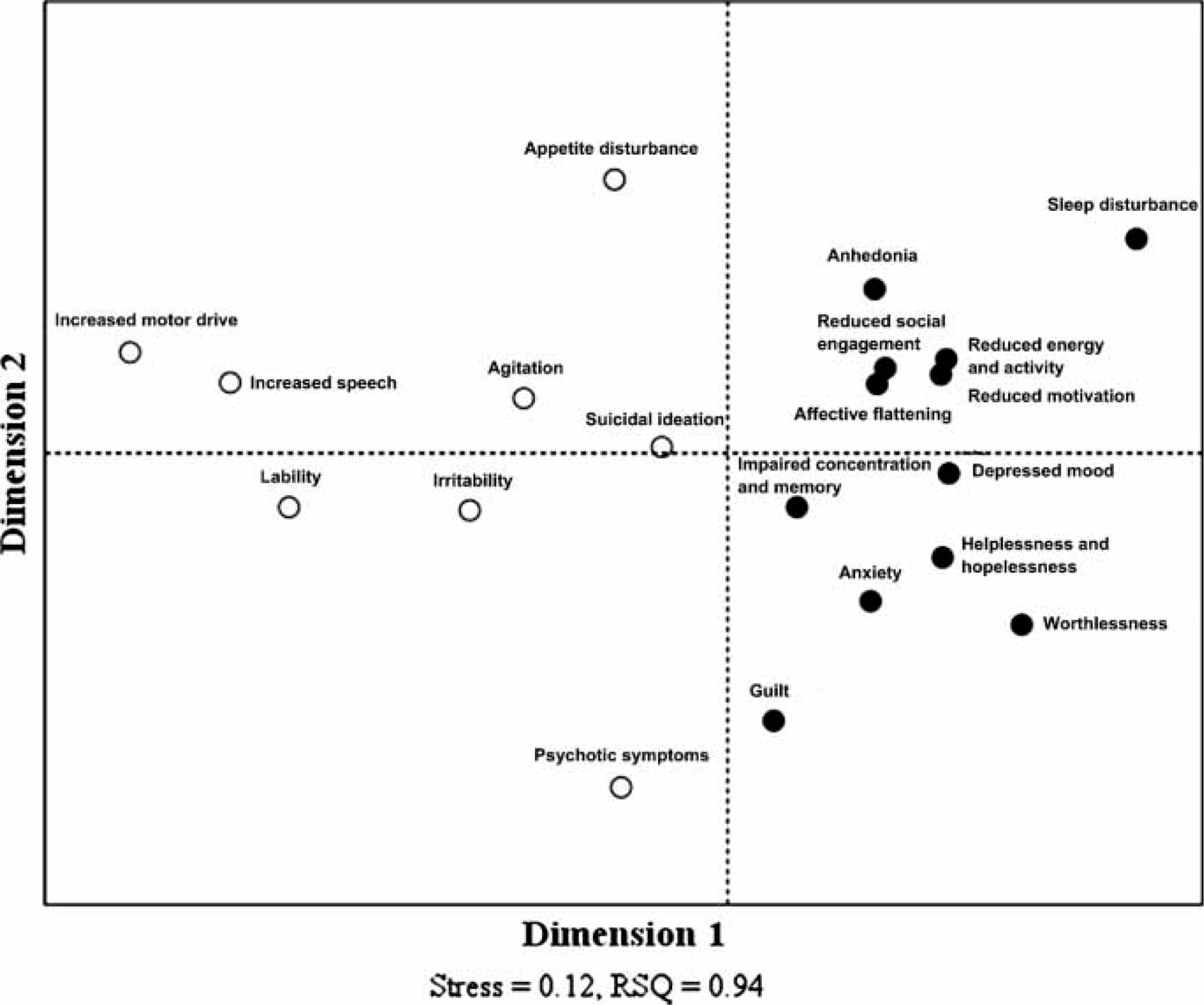
Relationships between the BDRS and other measures of mood symptoms
Partial correlations between scales after controlling for the effects of EPS on mood symptoms (n = 60)
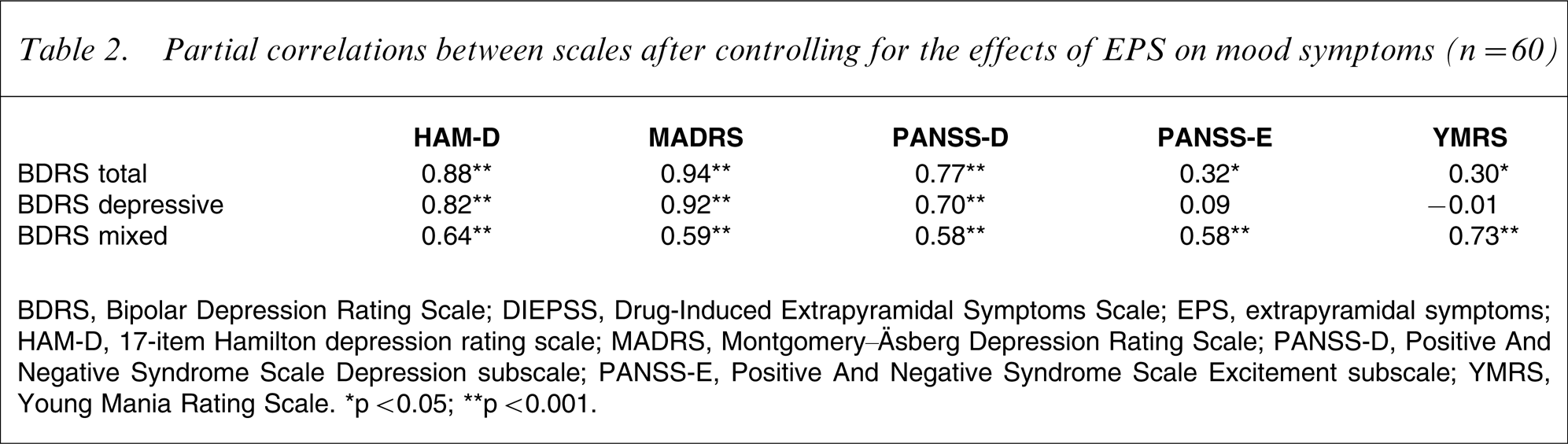
BDRS, Bipolar Depression Rating Scale; DIEPSS, Drug-Induced Extrapyramidal Symptoms Scale; EPS, extrapyramidal symptoms; HAM-D, 17-item Hamilton depression rating scale; MADRS, Montgomery–Äsberg Depression Rating Scale; PANSS-D, Positive And Negative Syndrome Scale Depression subscale; PANSS-E, Positive And Negative Syndrome Scale Excitement subscale; YMRS, Young Mania Rating Scale. ∗p < 0.05; ∗∗p < 0.001.
The geometric relationships between the rating instruments is shown in Figure 3. A 2-D solution was acceptable in terms of the Stress and RSQ. On the first dimension (dimension 1), the standardized scores of rating instruments for mood symptoms were clearly separated from the standardized score of DIEPSS for treatment-emergent EPS. In addition, according to the second dimension (dimension 2), the MDS space was partitioned into separate depression and mania subregions. The standardized z-scores were used for comparisons between the scores of the different rating scales.
2-D representation of the relationship between seven different scales from the sample of 60 patients with bipolar disorders. BDRS, Bipolar Depression Rating Scale; DIEPSS, Drug-Induced Extrapyramidal Symptoms Scale; HAM-D, 17-item Hamilton Depression Rating Scale; MADRS, Montgomery–Äsberg Depression Rating Scale; PANSS-D, Positive And Negative Syndrome Scale Depression subscale; PANSS-E, Positive And Negative Syndrome Scale Excitement subscale; YMRS, Young Mania Rating Scale.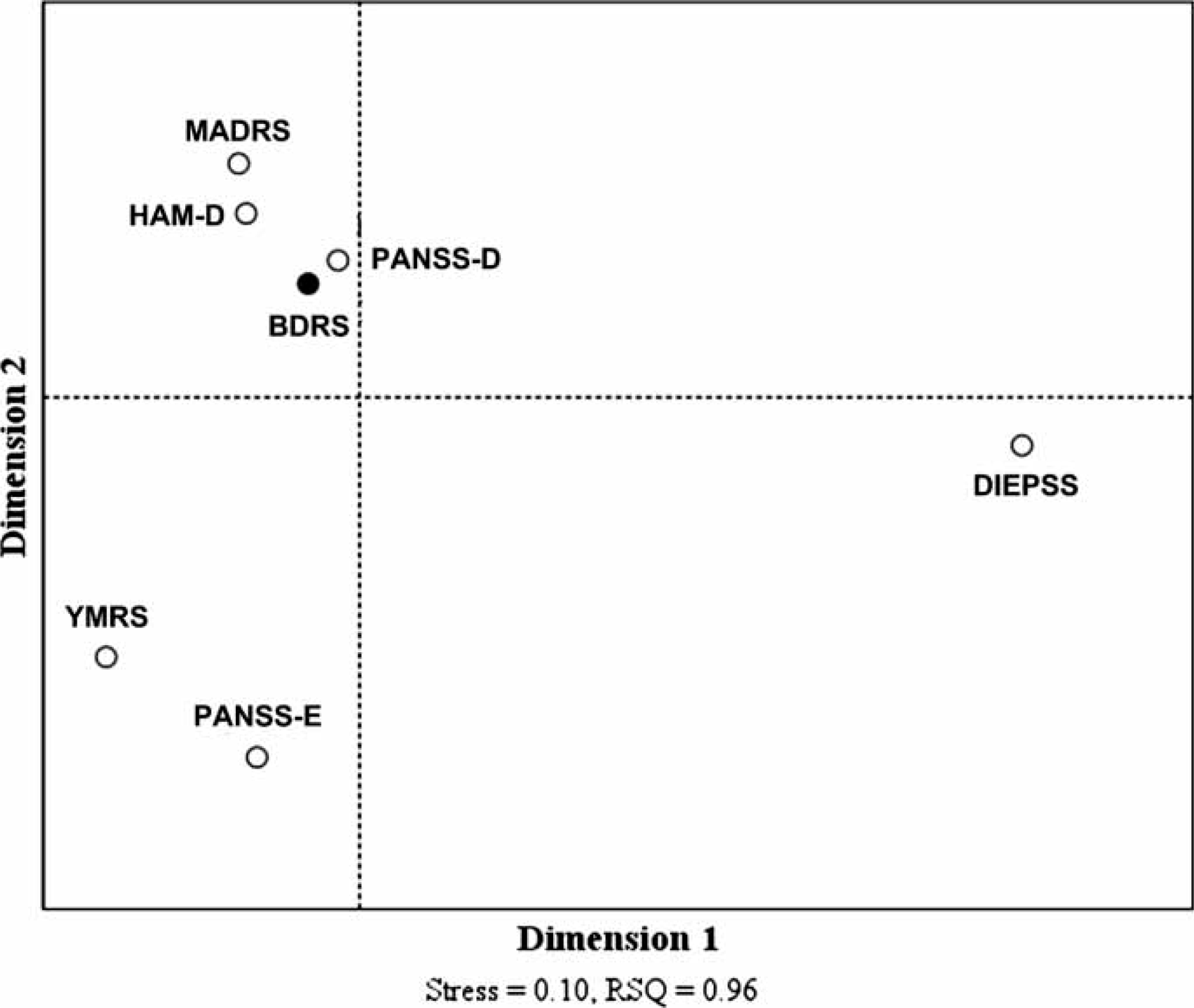
Discussion
The current study presents the cluster structure of 20 items on the BDRS in a sample of patients with bipolar depression. Two non-overlapping clusters of depressive and mixed symptoms were identified through HCA and MDS. High correspondence was observed between neighbourhoods in MDS configuration and clusters determined by HCA. Geometric properties of the cluster structure indicated the inherent heterogeneity of mixed symptoms compared to depressive symptoms, thereby explaining the contribution of mixed symptoms in formulating the characteristic features of bipolar depression. The cluster structure of the BDRS in patients with bipolar depression may underpin the need for more comprehensive methods in assessing clinically depressed patients with bipolar disorder instead of currently available depression rating instruments.
The underlying depressive–mixed dimension was in accordance with the previous results of factor analysis [5], but the subdivision of depressive factor (psychological–somatic) was not observed in this sample population. Because space-dilating methods including Ward's method and complete linkage tend to create non-overlapping clusters of hyperspherical form, highly correlated depression factors may form a single cluster instead of two clusters without a clear boundary. In any case, the BDRS was shown to cover the mixed symptoms of bipolar depression, maintaining its ability to assess conventional depressive symptoms. Therefore, the results of multivariate analysis suggest that the internal structure of the BDRS reflects the purpose of rating scale development.
A large body of evidence supports a qualitative difference in the phenomenology between unipolar and bipolar depression [42]. Some features such as leaden paralysis, psychomotor retardation, and lability of mood may suggest hidden bipolarity [2]. In addition, bipolar depression is inherently affected by subsyndromal manic or hypomanic symptoms [2]. Heterogeneous states of bipolar depression may require the understanding of intradepressive manic or hypomanic symptoms in assessing clinical changes in depressive patients receiving pharmacotherapy.
Correlation pattern between the BDRS and other rating instruments for mood symptoms is in line with previous results [5]. The relationships between the rating instruments were not significantly affected by the severity of treatment-emergent EPS, and thus the BDRS may not be more sensitive to clinical features of EPS compared with other depression rating instruments. Intriguingly, the subscales of the PANSS did not differ in assessing mood symptoms compared to other rating instruments. Therefore, in order to measure the multidimensional nature of bipolar depression, it may be plausible for clinicians to use a five-factor structure of the PANSS with other rating scales in patients with bipolar depression. The BDRS can thus effectively measure both depressive and mixed symptoms in patients with bipolar depression receiving pharmacotherapy, and it would be worthwhile to test whether the five-factor structure of the PANSS is useful in clinical research in bipolar depression.
Among various techniques of multivariate analysis, both HCA and MDS are effective methods for identifying a latent structure of complex data, which is not discernible through other multivariate techniques [33, 36]. Due to their less conservative nature, HCA and MDS have advantage over factor analysis in handling small-size data [37]. The essential properties of clusters can be easily explored using the MDS map, and thus these two techniques are often complementary.
There have been numerous studies reporting the differential characteristics of bipolar depression with regard to illness course and comorbidity: subsyndromal depressive symptoms [43], acute onset and abrupt cessation of depressive episodes [3], high rates of substance misuse [44], and so forth. These features are helpful in long-term recognition and management of bipolar disorder, but not associated with short-term evaluation of clinical changes in bipolar depression. Evaluating bipolar depression based on phenomenological characteristics of bipolar depression may provide clinicians with practical guidance in judging clinical response to therapeutic trials. Nonetheless, detailed description of mood symptoms is often difficult in a clinical setting. Even in research protocols, the syndromal differences between unipolar and bipolar depression are infrequently examined [45]. It is therefore necessary that more systematized means of assessing bipolar depression be developed and tested. The BDRS or other rating instruments designed for bipolar depression seem to be potential candidates [46].
There are certain limitations that need to be considered. First, all of the participants were Korean, which compromises the generalizability of the present study. No significant deviations were detected, however, in the basic properties of the BDRS between Korean and Australian samples regardless of ethnicity and language differences. Second, although the present sample size may not pose substantial problems in the statistical analyses, it is small for validation study. Third, because the multivariate statistics used here are characterized as descriptive, atheoretical, and non-inferential [36], the interpretation of data remains exploratory and heuristic. Nonetheless, the versatility of these techniques has made a substantial contribution to psychiatric research [35]. Finally, although mixed symptoms are often indicative of the syndromal differences between unipolar and bipolar depression, a subgroup of patients with unipolar depression may have prominent symptoms of ‘activation’, which are similar to hypomanic or mixed symptoms [47]. In addition, mixed depression is occasionally regarded as evidence of the continuity of mood disorders [48]. Therefore, using the BDRS in a broad range of mood disorders may provide additive information about the utility of the BDRS and the nature of bipolar depression.
In conclusion, the internal structure of the BDRS appears to be sensitive to mixed symptoms of bipolar depression. Regardless of the effects of treatment-emergent EPS, strong correlations with other depression rating scales suggested preserved ability of the BDRS in measuring the severity of depressive symptoms. Hence, the BDRS may enable the assessment of clinically significant changes in patients with bipolar depression within the therapeutic process.
Footnotes
Acknowledgements
This study was supported partly by grant number 03-PJ10-PG13-GD01-0002 from the Korea Health 21 R&D Project funded by the Ministry of Health, Welfare and Family Affairs, and partly by an unrestricted research grant number 06-2005-163-0 from Astra Zeneca Korea to Dr Kim. We would like to thank Dr Berk, who kindly supplied the BDRS and gave us comments on this study.