
Abstract
Attention-deficit–hyperactivity disorder (ADHD) is one of the most common childhood psychiatric disorders and is characterized by the core symptoms of inattention, hyperactivity and impulsivity with an early onset [1, 2]. The estimated prevalence of DSM-IV-defined ADHD is between 5% and 8% and that of ICD-10-defined ADHD is approximately 1.5% worldwide [3], while the corresponding figures among boys in Hong Kong were approximately 8.9% on the basis of DSM-III-R, and approximately 0.78% according to ICD-10 [4].
ADHD is a chronic and debilitating condition that could impact upon many aspects of a subject's life and cause significant academic, social, and emotional problems [5]. Preschool children with ADHD often present with excess motor restlessness, associated difficulties including delayed development, oppositional behaviour, and poor social skills [6, 7]. School-aged children with ADHD more frequently experience academic failure, rejection by peers, and low self-esteem [8]. In adolescence, children may develop further problems, including aggressive and antisocial behaviour, and at-risk behaviours [8]. In the past ADHD was assumed to gradually resolve after puberty [9], but recent longitudinal studies have suggested that ADHD can persist into adulthood [10], and as many as 60% of patients with ADHD symptoms in childhood continue to have problems in adult life, such as interpersonal difficulties with colleagues and employers and dismissal from employment, and they are at higher risk for drug and substance abuse and dependence [8].
In recent years quality of life (QOL) has emerged as an important outcome measure in guiding health care [11]. The World Health Organization (WHO) defined QOL as ‘an individual's perception of his/her position in life, in the context of the culture and value systems in which s/he lives, and in relation to goals, expectations, standards and concerns’ [12]. Preliminary evidence indicated that children and their parents have interrelated social and health needs [13], and the interactions between them are bi-directional [14]. For example, previous studies indicated that quality of the parents’ marital relationship, parenting stress and socioeconomic status were associated with behaviour problems in children 15–19; in contrast, children's mental problems could also lead to increased level of parenting stress, marital problems, role dissatisfaction and more frequent alcohol use for their parents [5], 20–22. Sawyer et al found that not only did children with psychiatric disorders including ADHD have a significantly poorer QOL than the healthy controls, their mental problems also interfered with the daily lives of their parents and families [23]. As a result, children's behaviour problems including ADHD could have a substantially negative influence on their parents’ QOL. To date, however, no study has explored the relationship between children's ADHD and their parents’ QOL.
The aims of the present study were therefore (i) to survey the QOL of parents of children with ADHD in Hong Kong; and (ii) to explore the relationships between sociodemographic and clinical variables and QOL.
Methods
Settings and subjects
The study was conducted between October 2007 and February 2008. A consecutive sample was used and the subjects were selected from a child follow-up psychiatric clinic of a university-affiliated district general hospital. All children participating in the present study were in treatment. The catchment area of the hospital covers a population of approximately 1. million. Parents of children with a diagnosis of ADHD according to DSM-IV were invited to take part in the study. The diagnosis of ADHD and any other comorbid psychiatric disorders were ascertained by scrutinizing medical records and confirming with the responsible psychiatrists. The assessment instruments were not used to assist in making the diagnoses. Exclusion criteria included (i) being non-Chinese; and (ii) having a child who is mentally handicapped. Mental handicap was defined as IQ <70 [24].
Assuming a medium effect size of 0.50 between the QOL of the parents and the general population in Hong Kong, with a power of 0.8 and significance level of 0.05 (one tailed), the sample size in the present study should be at least 64 according to Cohen's sample size tables [25].
Subjects meeting the study criteria were invited by the principal author (YT Xiang) to participate in the study on the day when they attended the clinic for routine follow up. Those who agreed to participate were asked to sign the consent form after they had been given a detailed explanation of the study.
Data collection
Sociodemographic and clinical data of children and their parents were collected from the children's clinic notes by the children's responsible clinician, and during face-to-face interview by the principal author (YT Xiang).
Assessment instruments
Hong Kong version of World Health Organization Quality of Life Schedule-Brief version
The World Health Organization Quality of Life Schedule–Brief version (WHOQOL-BREF) is a 26-item, self-administered generic questionnaire [26]. Subjects assess their satisfaction on each item during the past 2 weeks on a 5-point scale (from 1 = very dissatisfied to 5 = very satisfied). The 26 items can be divided into four subscales including physical health, psychological health, social relationships and environmental factors domains. The WHOQOL-BREF has well-established psychometric and cross-cultural properties and is sensitive to QOL changes. The scale has been widely used to assess QOL worldwide including Hong Kong [27].
Hong Kong version of the Strength and Difficulties Questionnaire
The Strength and Difficulties Questionnaire (SDQ) is a well-established and widely used screening instrument for psychopathology among children and adolescents. It consists of 25 statements relating to children's strengths and difficulties [28]. Each statement is rated on a 3-point scale (not true, somewhat true, certainly true). The 25 items are divided into five subscales: Conduct Problems, Emotional Problems, Hyperactivity, Peer Problems, and Prosocial Behaviour (each containing five items). Scores on the first four of these subscales are summed to provide a Total Difficulties score. The parent version of the SDQ was used in the present study and it has been validated for use among Chinese children in Hong Kong by two of the present authors (Lai et al.: unpublished data, 2009).
Hong Kong version of Strengths and Weaknesses of ADHD-Symptoms and Normal-Behaviour scale
The Strengths and Weaknesses of ADHD-Symptoms and Normal-Behaviour scale (SWAN) is an informant-rated questionnaire that contains 18 items to measure ADHD symptoms. Informants are asked to rate children's behaviours by comparing these with those of other children of the same age. The scores are rated on a 7-point scale, where negative scores indicate behaviours that are better than average, and positive scores indicate behaviours that are poorer than average (−3 = far above average, −2 = above average, −1 = somewhat above average, 0 = average, 1 = somewhat below average, 2 = below average, 3 = far below average) [29]. An individual's total score on the inattention and hyperactivity–impulsivity dimensions of the SWAN were then averaged to range from −3 to +3, with a negative score indicating a lower level of ADHD symptoms. The SWAN has been validated for use among Chinese children in Hong Kong by two of the current authors (Lai et al.: unpublished data, 2009).
Data analysis
Statistical analyses were performed using SPSS 13.0 (SPSS, Chicago, IL, USA). First, one-sample t-test was carried out to compare QOL rated in the present study with the norm of WHOQOL-BREF in Hong Kong. Second, the relationship between sociodemographic and clinical features and parents’ QOL domains was measured by means of Pearson correlation analysis when the data followed a normal distribution; otherwise Spearman rank correlation was used. Multiple regression using the stepwise method was used to identify factors affecting each of the QOL domains. Categorical variables were included as dummy variables. To avoid multicolinearity, tolerance was used to measure the strength of the linear relationships among the independent variables. In this case, ≥0.4 was regarded as acceptable. Two-tailed tests were used. Furthermore, a re-calculation of power based on the results was made using Cohen's criteria [25].
Ethical considerations
The research proposal was approved by the Joint Chinese University of Hong Kong–New Territories East cluster Clinical Research Ethics Committee in Hong Kong. All subjects involved had given written consent.
Results
Subject characteristics
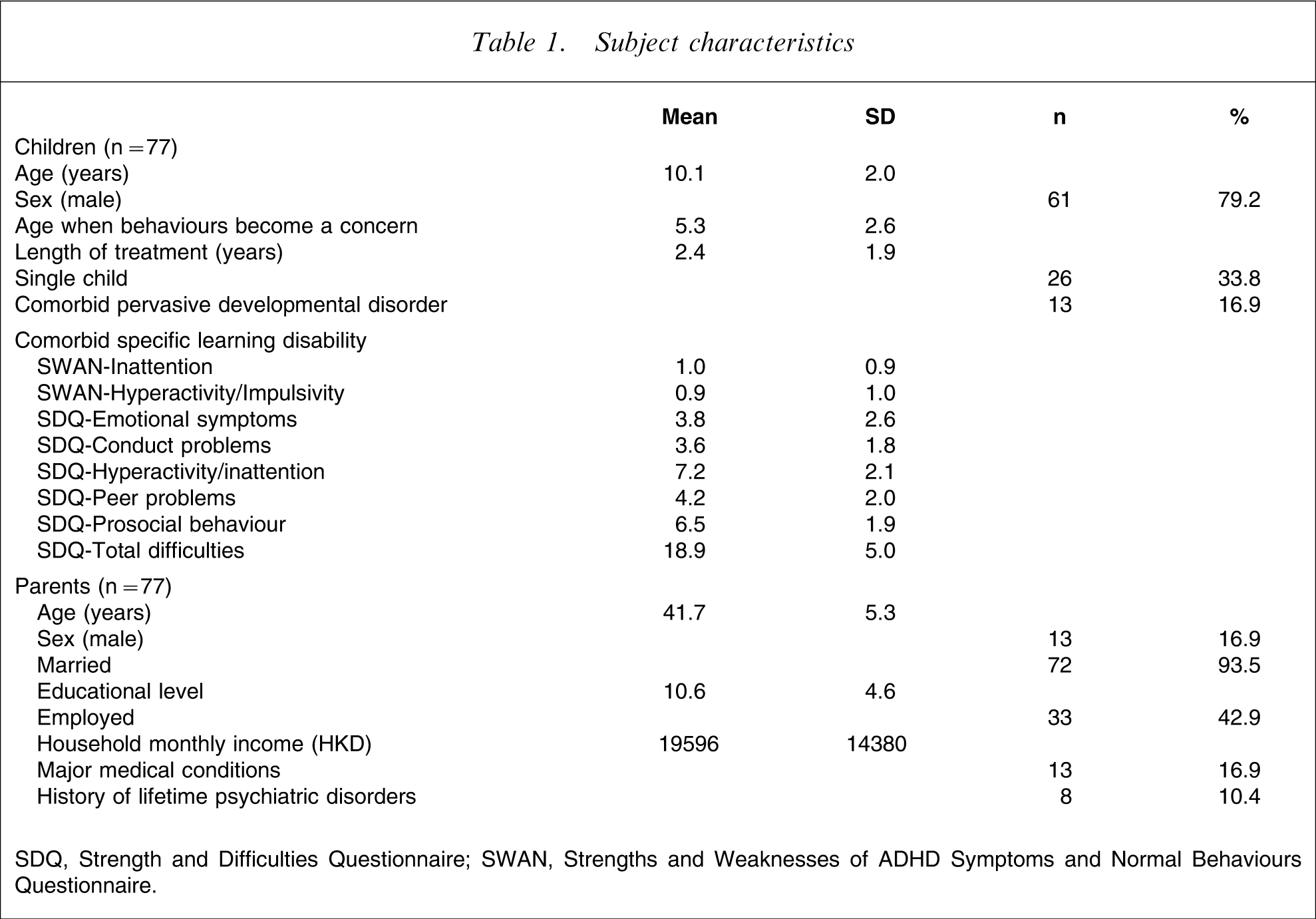
SDQ, Strength and Difficulties Questionnaire; SWAN, Strengths and Weaknesses of ADHD Symptoms and Normal Behaviours Questionnaire.
QOL in parents vs Hong Kong general population
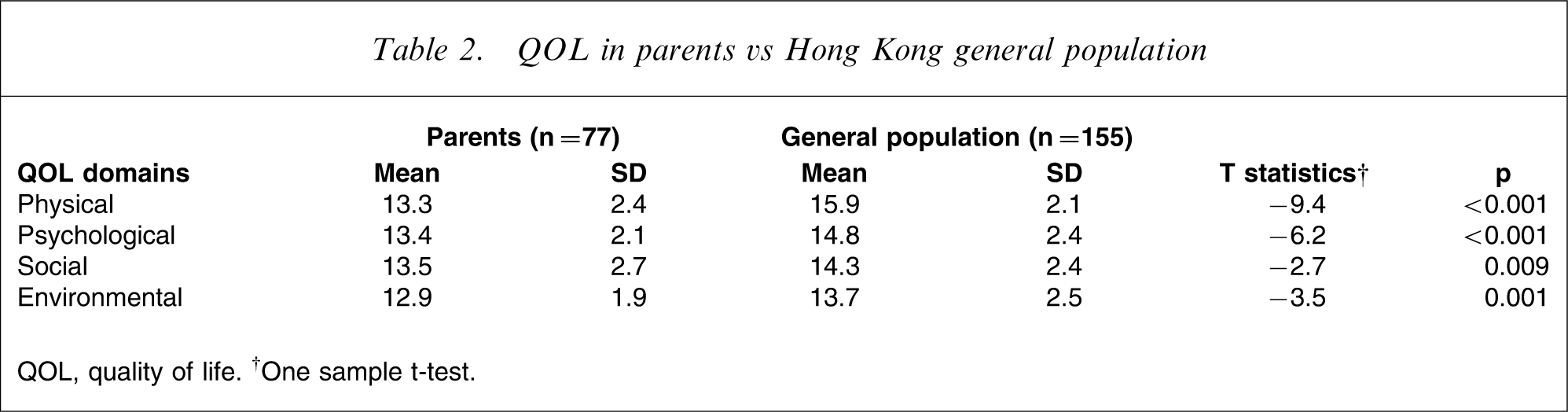
QOL, quality of life. †One sample t-test.
Correlation of sociodemographic and clinical factors vs QOL domains
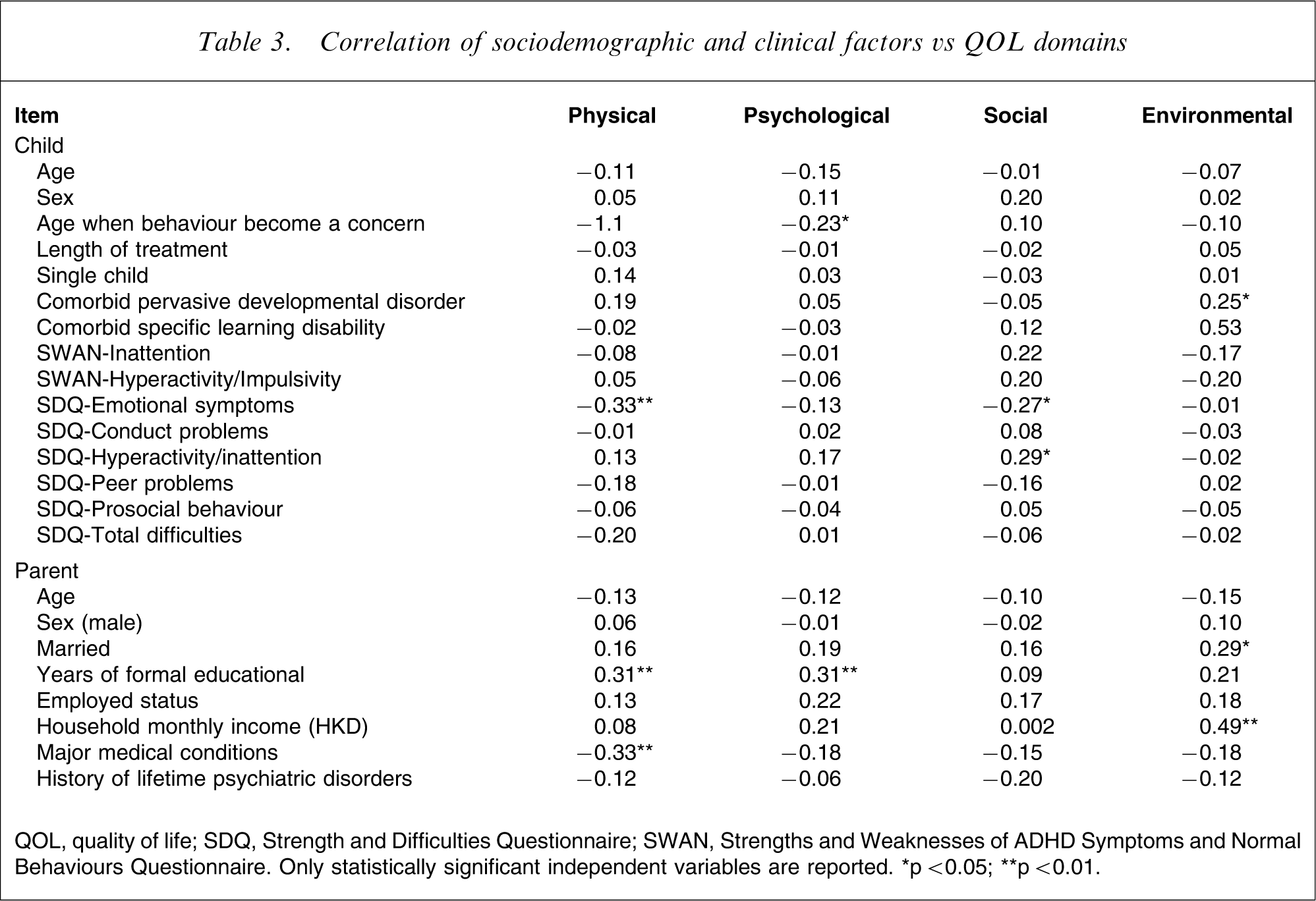
QOL, quality of life; SDQ, Strength and Difficulties Questionnaire; SWAN, Strengths and Weaknesses of ADHD Symptoms and Normal Behaviours Questionnaire. Only statistically significant independent variables are reported. ∗p < 0.05; ∗∗p < 0.01.
Stepwise multiple regression for QOL and demographic and clinical variables in Hong Kong†
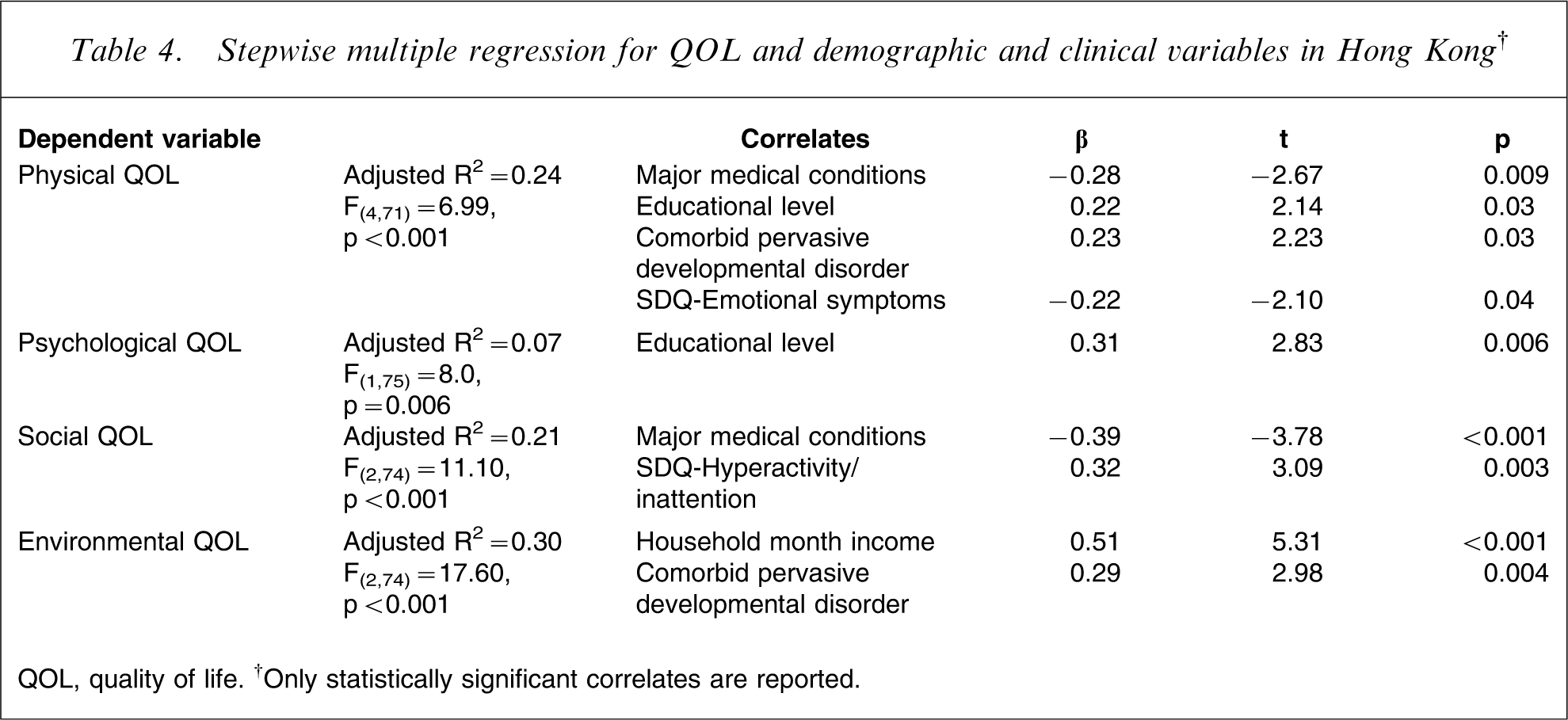
QOL, quality of life. †Only statistically significant correlates are reported.
Based on the differences between the participants and the general population in Hong Kong in the four QOL domains, using Cohen's method [25], the average power achieved in the present study was 0.82 (one-tailed).
Discussion
To the best of our knowledge, this is the first study exploring QOL and its sociodemographic correlates in parents of children with ADHD.
As expected, the children in the present study had more severe ADHD symptoms (SWAN scores) and general psychopathology (SDQ scores) in comparison with the community norms, and their parents had significantly poorer scores in physical, psychological, social and environmental QOL domains compared with the general population in Hong Kong.
Johnston and Mash reported that the presence of ADHD could lead to increased likelihood of disturbances to family and marital functioning, reduced parenting efficacy, disrupted parent–child relationships, and increased levels of parent stress [5]. Pelham and Lang found that ADHD was associated with increased parental alcohol use [20]. Befera and Barkley demonstrated that mothers of hyperactive children reported more depressive symptoms and marital discord compared to those of healthy children [31]. Given the aforementioned potential influences of ADHD, the present finding could be partly explained by the distress/protection QOL model, which suggests that QOL is the outcome of an interaction between various protective factors and a number of distressing factors [32]. QOL decreases if distressing factors (such as disturbances to family and marital functioning, disrupted parent–child relationships, increased parental alcohol use and depressive symptoms) predominate over protective factors (such as social support from family and friends, self-efficacy, task and avoidance). Although the poorer QOL experienced by this group of parents is expected, it is interesting that it is not so much the ADHD symptoms, but the presence of emotional and hyperactivity/inattention symptoms in the children that is significantly correlated with the parents’ QOL. In addition, it should be noted that 10.4% of the parents in the present study had a history of lifetime psychiatric disorders, which might contribute to their lower QOL, although on multiple analyses the history of lifetime psychiatric disorders was not independently associated with any QOL domain.
As well as factors relating to the children's ADHD symptoms, parents’ own characteristics expectedly also contribute to their QOL. Similar to previous findings [33, 34], parents with major medical conditions reported lower physical and social QOL domains. We found that higher educational level had a favourable effect on physical and psychological QOL domains in parents of children with ADHD, which was consistent with earlier findings in both the general population [35] and in subjects with chronic physical illnesses such as asthma and diabetes [36, 37]. The possible reasons might be that well-educated subjects can find appropriate employment and their living conditions could more likely satisfy their needs and expectations accordingly, and subjects with higher education have more access to information on ADHD or the illnesses they suffer, and are more aware of treatment strategies, so are less stressed. Therefore, in light of the Satisfaction QOL Model [38], they would have a higher QOL compared to subjects with lower levels of education.
Higher household monthly income was associated with better environmental QOL domain in this sample. Fitzgerald et al. suggested that subjects’ QOL was independent of their living standard as long as it reached a certain minimum level [12]. We suggest that the average living standard in the present sample did not reach the ‘certain minimum level’ although the household monthly income was comparable with the local average level (approximately HKD16 700) during the same period. In addition to monthly income, living standard was determined by many other factors such as housing conditions, price level etc., which were not measured in the present study. More variables relevant to living standard should be included in future studies.
We found that severity of emotional symptoms was associated with lower physical QOL domain. Contrary to our expectations, however, presence of comorbid pervasive developmental disorder was associated with higher physical and environmental QOL domains, and severity of hyperactivity/inattention symptoms of the children with ADHD was associated with higher social QOL level of the parents. We could offer no explanation for this striking finding. To date we are not aware of any data or evidence suggesting a positive association between any pervasive developmental disorder or hyperactivity/inattention symptoms in children and the QOL of their parents. Longitudinal studies may shed light on this unexpected and inexplicable connection. In the present study the SWAN hyperactivity/impulsivity score had also a mild positive relationship with social QOL, but did not reach a significant level (r = 0.20).
The present results should be interpreted with caution due to certain methodological limitations. First, the sample size was relatively small. Second, the study was cross-sectional, therefore the causality of the relationship between QOL and sociodemographic and clinical variables could not be explored. In order to clarify the causal relationship between QOL and other relevant factors, longitudinal studies involving more variables (such as parental functioning, parenting stress, marital quality etc.) and a larger sample are needed in the future. Third, without a control group, comparisons could be made only with the Hong Kong norms found using the WHOQOL-Bref [30]. A matched control group would have been more appropriate. Fourth, the majority of the parents involved were mothers (83.1%). Given the previous findings that there could be differences in maternal and paternal parenting practice [19], both fathers and mothers of children with ADHD should be interviewed in future studies. Finally, the present results indicated that of the six correlates of QOL, three are ADHD related (severity of emotional and hyperactivity/inattention symptoms and presence of comorbid pervasive developmental disorder) and three are parent related (presence of major medical conditions, educational level and household monthly income). Therefore we cannot exclude the possibility that the parents who had a lower QOL previously were likely to have it lowered further by parenting a child with ADHD. As a result, the potential interaction between ADHD- and parent-related factors should be clarified in future longitudinal studies with a large sample size.
In conclusion, parents of children with ADHD had a lower QOL in all the domains when compared with the norm of the general population in Hong Kong. Whether these results underline the deleterious effect of ADHD suffered by children on the QOL of the parents needs to be further investigated. Because of their significant correlations with different domains of QOL, more attention should be paid to children with co-occurring emotional symptoms. Attention should also be given to parents with major medical conditions, lower educational level and lower household monthly income. In order to improve QOL of parents having a child with ADHD, mental health professionals could adopt more specific measures based on the findings of the current study, such as reducing co-occurring emotional symptoms by optimizing treatment of ADHD.
Footnotes
Acknowledgements
The authors would like to sincerely thank Professor G. S. Ungvari in the Department of Psychiatry at the Chinese University of Hong Kong for his valuable comments in the preparation of this manuscript. We are also grateful to Dr Arthur Mak and other staff in the children's psychiatric clinic of Alice Ho Miu Ling Nethersole Hospital for their assistance in the project.