
Abstract
Keywords
For several decades there has been an increasing interest in the linkage between homocysteine metabolism and neuropsychiatric disease. Recent studies of schizophrenia patients have found higher levels of homocysteine 1–3. A recent meta-analysis showed that a 5 µmol L−1 increase in plasma homocysteine level was associated with a 70% higher risk of schizophrenia [4]. Homocysteine-reducing strategies, such as oral folic acid, vitamin B12 and pyridoxine, improved the positive, negative and psychopathology subscale of the Positive and Negative Syndrome Scale (PANSS) in schizophrenia patients with hyperhomocysteinaemia [5]. Homocysteine level tended to be higher in patients with a family history of mental illness [6] and correlated with the severity of extrapyramidal symptoms [7]. It was therefore postulated that an elevated homocysteine level was associated with the clinical phenotypes of schizophrenia. There have been other studies, however, yielding inconsistent results [8, 9], indicating that the role of homocysteine in schizophrenia is controversial.
The current study is the largest study, to the authors’ knowledge, to be carried out on homocysteine levels in schizophrenia patients, with consideration of confounding factors, such as drugs, medical and psychiatric illnesses, lifestyle and physiological determinants. It is also the first study in a Chinese (Han) population. The aims were to compare the serum homocysteine levels between schizophrenia patients and healthy controls and to ascertain whether the level was associated with duration of illness, clinical symptoms of schizophrenia, age at onset and family history of mental illness.
Method
Inclusion and exclusion criteria
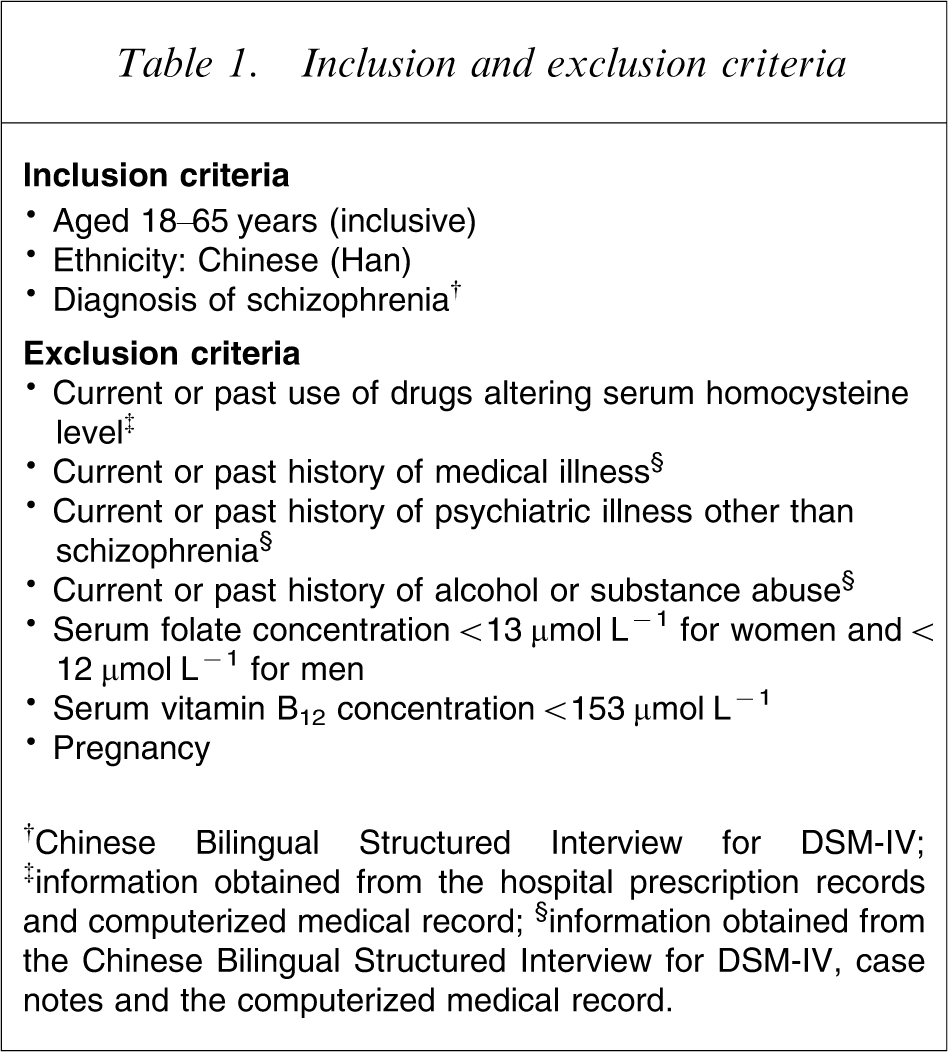
†Chinese Bilingual Structured Interview for DSM-IV; ‡information obtained from the hospital prescription records and computerized medical record; §information obtained from the Chinese Bilingual Structured Interview for DSM-IV, case notes and the computerized medical record.
The control group consisted of healthy individuals recruited from the donors at the Red Cross Blood Donation Centre (Mong Kok) in Hong Kong, with written informed consent. There was no advertisement for recruitment of the control subjects and the same inclusion and exclusion criteria were applied, the only difference being the diagnosis of schizophrenia. Each of the control subjects were screened by the same clinician using the same structured diagnostic interview (CB-SCID-I/P) to exclude any psychiatric diagnosis. A computer-generated table of random numbers was used to determine which donors should be included. Each selected donor underwent blood analysis for biochemical markers, including serum homocysteine level, and assessment of demographics. They were also evaluated for their smoking habit, BMI and family history of mental illness as for the case subjects. Of the 257 donors who fulfilled the criteria and consented to be included, 250 were randomly selected. There were no significant differences between the demographic data and characteristics of the participants and non-participants.
Confounding factors (i.e. drugs affecting serum homocysteine level, medical and psychiatric illnesses other than schizophrenia, alcohol and substance abuse, folate and vitamin B12 deficiency, and pregnancy) were eliminated using the exclusion criteria (Table 1). All clinical subjects had been put on a balanced diet designed by the hospital dieticians for at least 1 month before the study, there being no alcohol or coffee on the dietary menu. Smoking status, age and gender were recorded for both patients and controls: these factors would be controlled by statistical methodology in the analysis of the results.
A 4 mL venous blood sample collected from either patient or control was immediately transferred to an ice-cooled plain bottle and transported to the chemical pathology laboratory of Queen Elizabeth Hospital within 1 h. Upon arrival the blood samples were immediately centrifuged and a 1 mL aliquot of the serum transferred to a separate bottle for storage at −70°C. Tests were performed in a batch after collection was completed, and serum homocysteine level was assayed using the Axsym homocysteine assay (Abbott Laboratories, Abbott Park, IL, USA), with the technicians being blind to participant status.
Statistical analysis was undertaken to examine any significant difference between the clinical and control groups on the demographic data, including age, gender, smoking habit and BMI. Independent t-tests were then carried out to ascertain any significant difference in the homocysteine level between the two groups. Following this, analysis of covariance (ANCOVA) was used to determine the differential effects of gender and diagnosis.
Results
Subject characteristics (n = 500)
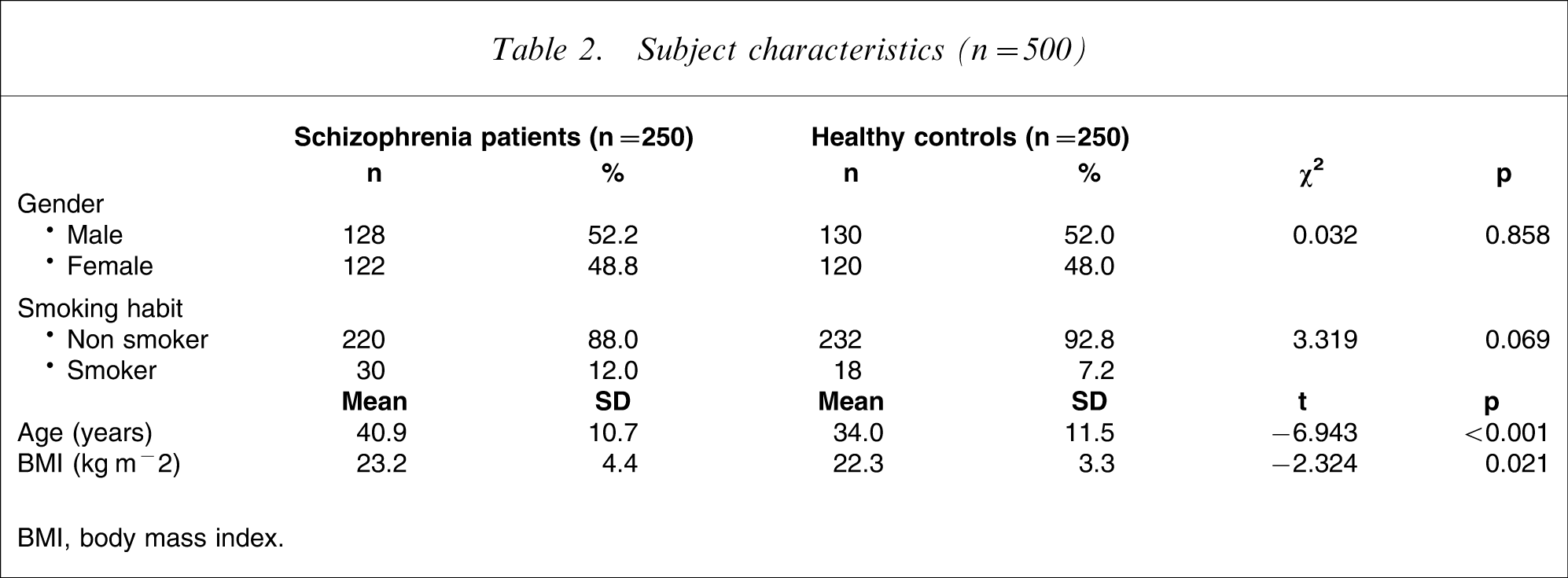
BMI, body mass index.
Serum homocysteine levels (µmol L−1)
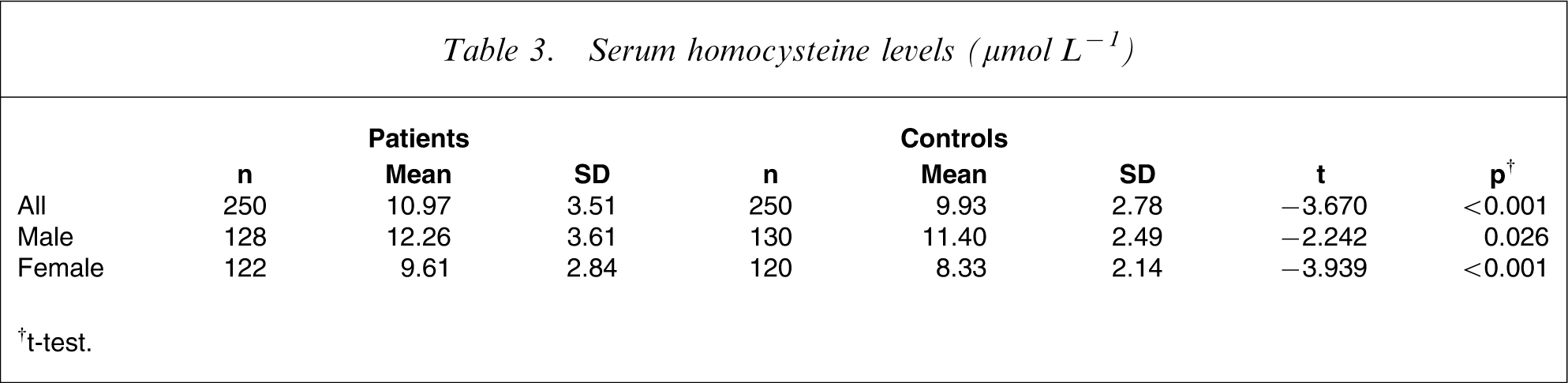
†t-test.
There was a significant positive association of homocysteine level with age (Pearson correlation coefficient = 0.115, p = 0.01, n = 500) but no significant correlation with BMI (Pearson correlation coefficient = 0.075, p = 0.092, n = 500). The homocysteine level was significantly higher in men (p < 0.001) and smokers (p = 0.004) in both patients and control subjects. Because there was no significant difference in the number of smokers between the patient group and control group, smoking habit did not contribute to the difference of homocysteine levels between the two groups.
Analysis of covariance (ANCOVA) with serum homocysteine level as the dependent variable, and diagnosis of schizophrenia and gender as independent variables, adjusting for age, indicated significant main effects of diagnosis (df = 1, F = 12.79, p < 0.001) and gender (df = 1, F = 126.9, p < 0.001) on homocysteine levels, but there was no interaction effect between gender and diagnosis.
Serum homocysteine level vs clinical parameters (Pearson correlation)
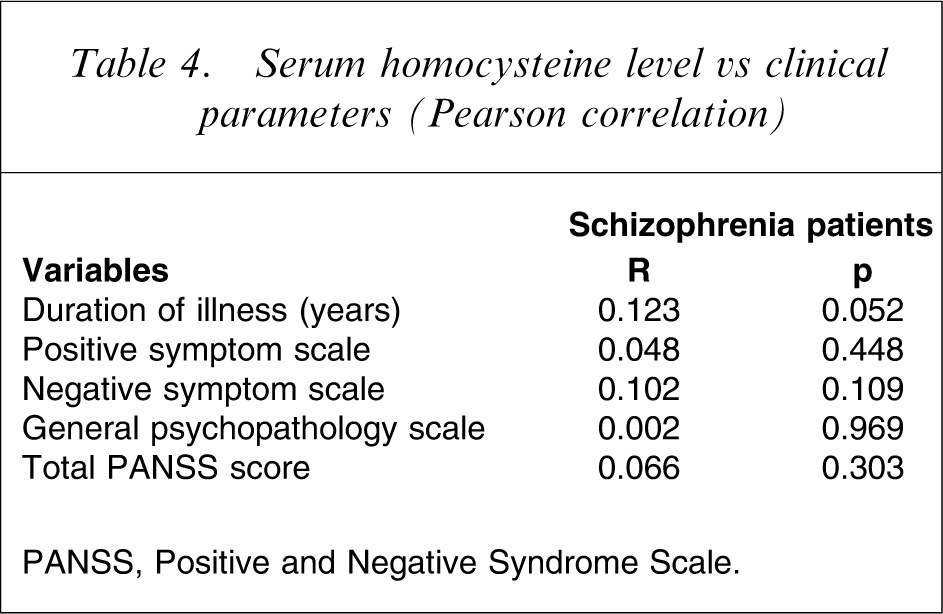
PANSS, Positive and Negative Syndrome Scale.
Because there is no established reference range for the Chinese population, hyperhomocysteinaemia was defined as concentration exceeding the 90th percentile of the control group. This definition was adopted in previous studies on homocysteine [11]. A total of 27 male (21.1%) and 28 female (23%) schizophrenia patients had homocysteine concentrations above the corresponding cut-off points (male patients, 14.27 µmol L−1; female patients, 10.86 µmol L−1). Logistic regression was used to investigate the relationship between different levels of homocysteine and the prevalence of schizophrenia. For serum homocysteine levels in the fourth quartile (men, >13.02 µmol L−1; women, >9.97 µmol L−1) the odds ratio was 2.2 (95% confidence interval = 1.3–3.8; p = 0.004) compared with the lowest quartile. These results persisted even after considering the effects of gender and age.
Serum homocysteine level vs clinical phenotype in schizophrenia patients
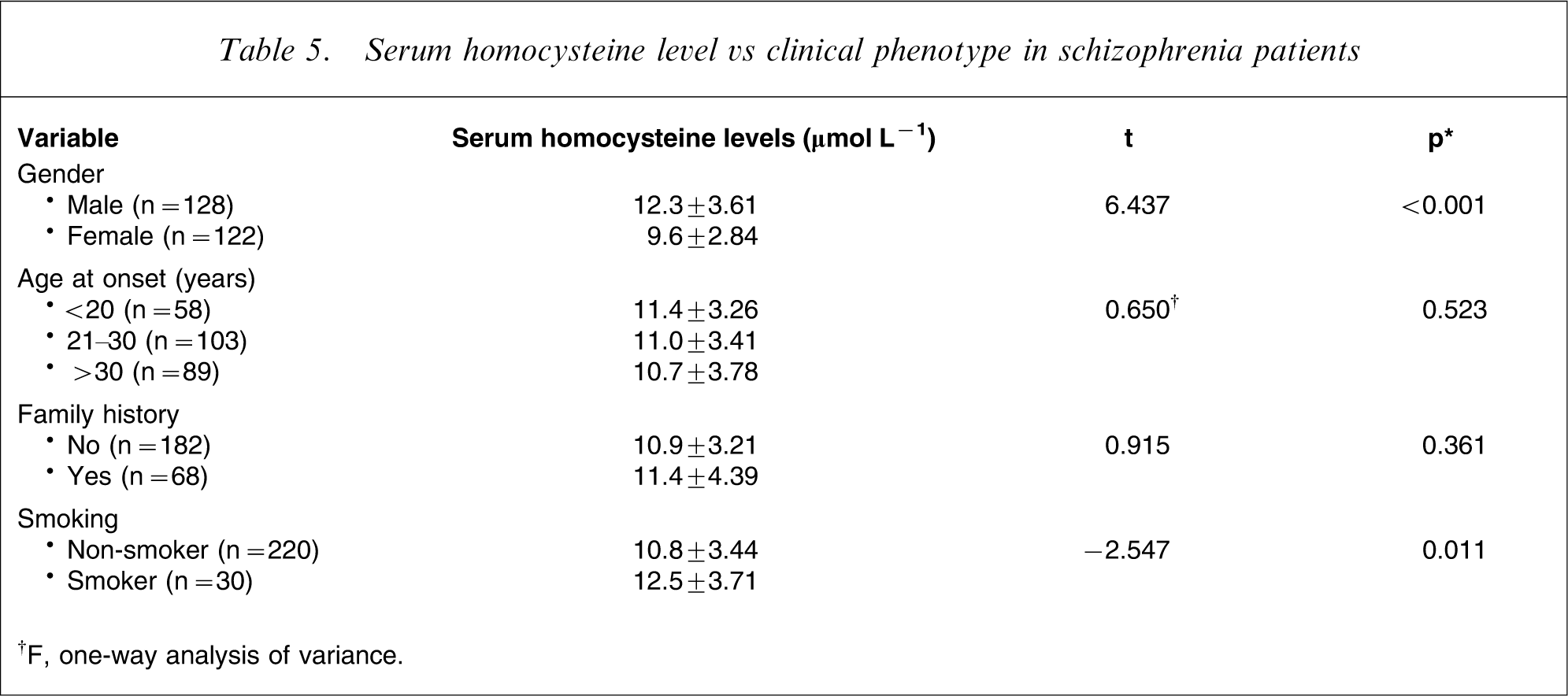
†F, one-way analysis of variance.
Discussion
This study confirmed the hypothesis that serum homocysteine levels were elevated among schizophrenia patients. This result is in agreement with studies in Caucasian subjects [13, 14], the Southern Israel population [1], the Arabian Gulf population [15] and the Korean population [16].
Negative findings were, however, reported in other studies 17–19. Some were of a smaller sample size. Inadequate power may have resulted in false acceptance of the null hypothesis. Also, some studies involved a heterogeneous sample of other diagnoses such as schizoaffective disorder or bipolar disorders. In the current study such patients were excluded by the strict adherence to the DSM-IV criteria and the use of a structured diagnostic interview.
In the present study the prevalence of schizophrenia was increased more than twofold in the fourth quartile of homocysteine concentrations compared with the lowest quartile. This finding persisted after considering the effects of gender and age and was consistent with previous findings [13].
Compared with previous studies that reported markedly elevated homocysteine levels (i.e. a difference of 5.7–10 µmol L−1 in young male schizophrenia patients [1, 2]), the present observed elevation in the schizophrenia versus the control group was moderate. This difference could be accounted for by the method of measurement and the different dietary habits of the ethnic groups studied. Variations of homocysteine results between methods and laboratories are considerable [20] and international standard reference materials have been available only recently [21]. The present study used a fluorescence polarization immunoassay, which has the advantage of lower analytical imprecision (4.5% [22]) than high-performance liquid chromatography (6.7% [23]) used in other studies.
The Western diet is higher in total fat (saturated fat and trans-fatty acids) but contains fewer vegetables and fruits compared with the Chinese diet [24]. Moreover, coffee is much more widely consumed [25]. Modification of dietary pattern with increased consumption of fruit and vegetables and reduced consumption of saturated and total fat has been shown to lower plasma homocysteine level [26] and this may explain the general lower homocysteine values in the present study compared with those in other ethnicities.
The present study found no significant correlation between serum homocysteine levels and duration of illness, age at onset or clinical symptoms measured on PANSS. These findings were in agreement with recent evidence for the lack of an association between homocysteine level and clinical phenotypes of schizophrenia [15, 27].
Confounding factors affecting homocysteine level were strictly controlled in the present study. Elevated homocysteine levels in the present study were unlikely to be due to the use of antipsychotics or other drugs, because subjects on drugs known to affect homocysteine levels 28–31 were excluded from the study. It is now well-documented that antipsychotics do not influence homocysteine level [14, 26, 32]. The result was also unlikely to be due to the presence of other medical or psychiatric illnesses because they had been excluded from the study.
Lifestyle determinants such as diet, alcohol and coffee were controlled in all the patients, none had a BMI suggesting malnutrition, and anyone with folate or vitamin B12 deficiency was excluded. The smoking habit of each subject was recorded, there being no significant difference between the patient and control groups.
Physiological determinants predicting homocysteine levels in schizophrenia patients, such as gender, plasma folate and vitamin B12 levels, mean red blood cell corpuscular volume and diastolic blood pressure were considered by Stahl et al. [33]. Only 24% of the variance in male patients was explained by these variables, the main reason for elevated plasma homocysteine level in schizophrenia patients remained unclear. Therefore, the observed association in the present study of elevation of homocysteine with schizophrenia was unlikely to be explained by these confounding factors.
Certain limitations should be acknowledged when interpreting these results. The clinical subjects were recruited from an inpatient setting and might be somewhat different to the overall population of schizophrenia patients. Also, the age of the blood donors was younger than the patients; statistical methods were used in an effort to adjust for this. Moreover, the study was cross-sectional in design, which limited the extent to which a causal relationship between serum homocysteine levels and schizophrenia could be established. Furthermore, the relationship of homocysteine to the methylenetetrahydrofolate reductase genotype was not explored.
More research is warranted to determine the cause(s) of elevated homocysteine levels in schizophrenia, the association with genetics and whether there is elevation at disease onset, thereby providing the potential for early instigation of treatment. Prospective studies are also warranted on the use of homocysteine-reducing agents in the treatment of schizophrenia.
Conclusion
Serum homocysteine level was found to be elevated in Chinese schizophrenia patients. The levels were increased in both male and female patients. Other clinical parameters such as duration of illness, clinical symptoms, age at onset of disease and family history of mental illness did not appear to be related to serum homocysteine levels.
Footnotes
Acknowledgements
The study of homocysteine levels in Chinese schizophrenia patients was funded by a grant from the Queen Elizabeth Hospital Research Fund. This study is part of the dissertation for the Hong Kong College of Psychiatrists Part III Fellowship Examination in 2008. Great appreciation is extended to the Red Cross Blood Donation Centre and the Department of Pathology at Queen Elizabeth Hospital for their support. The authors would also like to thank the individuals who took part in the study.