
Abstract
Surveys of prescribing patterns in the use of neuroleptics are generally critical of the excessive dosages prescribed and of the practice of polypharmacy [1]. Polypharmacy, defined as the simultaneous use of two or more neuroleptics, seems to be even more common among Asian psychiatric patients [2–4].
Research data suggest that Asian patients may require lower doses of neuroleptic medications [5,6] and are probably more vulnerable to developing extrapyramidal side-effects (EPSE) [5,7,8,].
Considering the above, the expectation is that in a Chinese psychiatric population, the usual practice would be one of using small doses of a large number of neuroleptic drugs.
To examine this, we surveyed the prescribing pattern in Chinese patients with chronic schizophrenia in a state mental hospital in Singapore and compared our findings with surveys of Chinese patients in other countries.
Method
Singapore is an island state in South-East Asia with a population of about 3 million, with the Chinese being the majority ethnic group. Wood-bridge Hospital is the only state mental hospital in Singapore. The majority of patients with schizophrenia are highly likely to have received their entire treatment at this hospital which also maintains records from first contact. It is therefore possible to obtain a comprehensive lifetime history of patients' drug treatments.
This survey was conducted in the long-stay wards of Woodbridge Hospital over a 3-month period from January to March 1999. All patients currently resident in the hospital and meeting DSM-IV criteria for schizophrenia based on chart review by a psychiatrist (SAC) were included. Two hundred and three patients were not interviewed as their diagnoses based on their medical records were inconclusive. Consent from the patients was obtained before assessment and 97 were excluded because of lack of consent. We converted dosages of neuroleptics to mg chlorpromazine equivalents (mg CPZ-eq) using standard guidelines [9,10]. Ethics approval for this study was given by the Institute of Mental Health, and Woodbridge Hospital, Singapore.
Extrapyramidal side-effects (EPSE) were assessed by the Simpson-Angus Rating Scale [11], and undertaken by three psychiatrists who were blind to the clinical and medical histories of the patients. The raters had jointly assessed a number of patients over three sessions before the start of the study and an interrater reliability (intraclass correlation) coefficient of 0.82 was obtained for the total scores.
Differences between groups were tested by t-test and Mann–Whitney U-test for normal and non-normal continuous variables respectively, and the χ2-test for categorical variables.
Results
Of the 534 patients, there were 404 males and 130 females. The mean (SD) age of the patients was 53.2 (11.4) years. The median duration of illness was 30.0 years (range = 3.0–58.0 years) and the mean (SD) was 29.3 (10.1) years. Only 18 patients were not prescribed any psychotropic drugs, and the remaining 516 patients received a median daily dose of 400.0 mg CPZ-eq (range 50.0–2875.0 mg), with the mean (SD) dose being 600.0 (593.8) mg CPZ-eq. Ninety (17%) patients were receiving more than 1000 mg CPZ-eq of neuroleptic medications daily. There were no differences in gender distribution between those prescribed multiple neuroleptics and those with none or one neuroleptic (χ2 = 0.12, df = 1, p = 0.73) although those receiving multiple neuroleptics were younger with a mean (SD) age of 49.1 (10.1) years versus 59.6 (11.2) years (t = 11.33, df = 534, p < 0.001). Patients who were prescribed one neuroleptic received a daily mean (SD) dose of 168.8 (147.5) mg CPZ-eq with a median of 125.0 mg CPZ-eq compared with a mean of 823.8 (622.7) mg CPZ-eq and a median of 625.0 mg CPZ-eq for those receiving two or more neuroleptics (Mann–Whitney U-test: z = −16.2, p < 0.005).
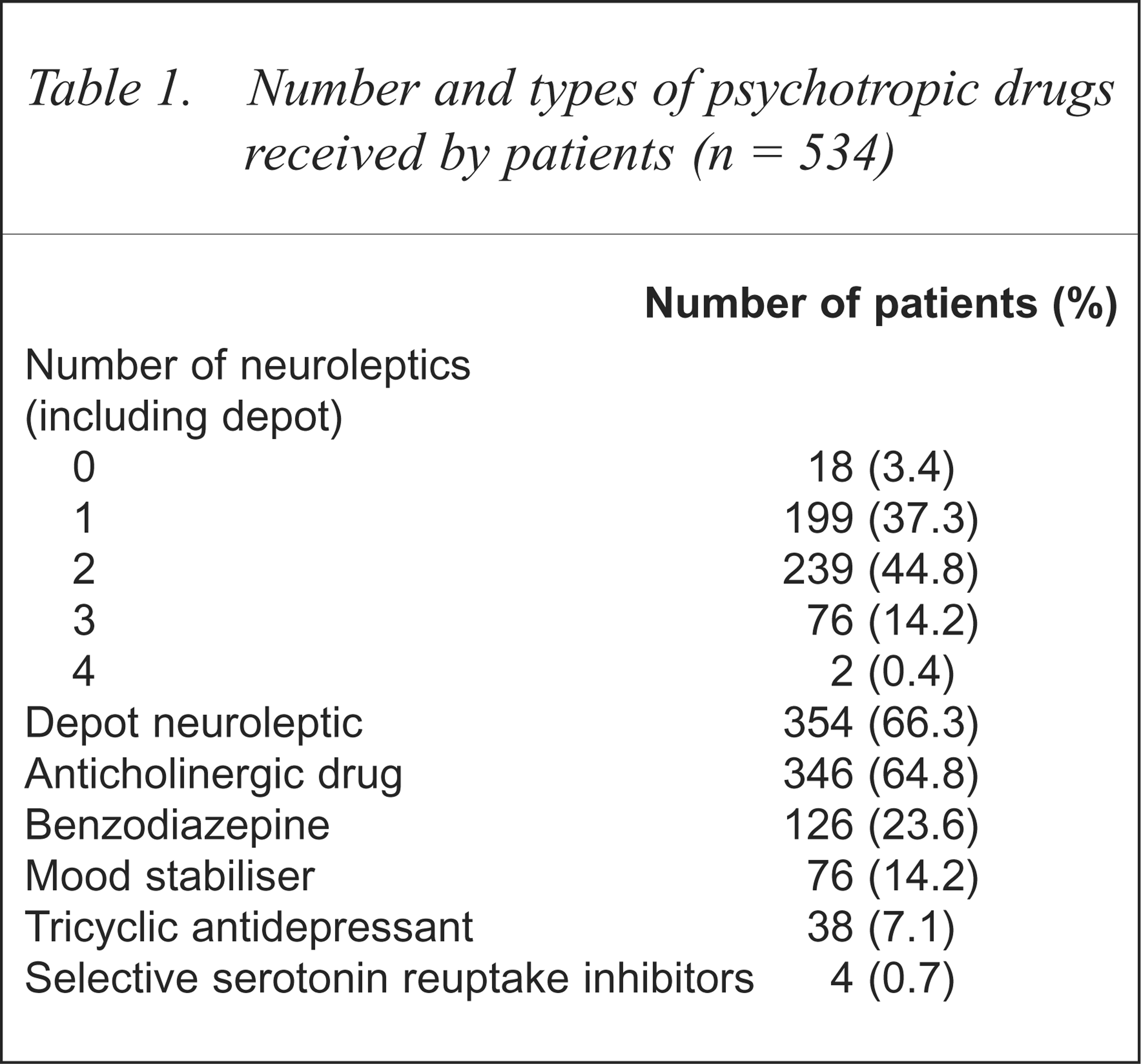
Table 1 shows the various psychotropic medications prescribed for these patients. There were only six (1.1%) patients who were prescribed atypical neuroleptics (three receiving clozapine and the other three risperidone).
Number and types of psychotropic drugs received by patients (n = 534)
Patients on depot neuroleptics received significantly higher CPZ-eq daily dose than those on oral neuroleptics. The respective medians were 525.0 mg CPZ-eq/day (range 31.3–2875.0 mg) and 125.0 mg CPZ-eq/day (range 10.0–1900.0 mg) (Mann–Whitney U-test: z = −12.0, p < 0.001).
Sixty-five per cent of patients were prescribed an anticholinergic agent (trihexyphenidyl being the only agent used). Table 2 shows the characteristics of patients receiving and not receiving trihexyphenidyl. Those receiving trihexyphenidyl were younger, in receipt of higher CPZ-eq doses and had lower Simpson-Angus scores (see Table 2). The mean (SD) cumulative neuroleptic exposure for our patients was 19.1 (11.1) years while the mean (SD) cumulative trihexyphenidyl treatment was 7.5 (7.5) years.
Characteristics of patients with and without anticholinergic drug
Discussion
In surveys of Chinese patients, the daily neuroleptic dose has varied widely in different countries and in different settings within the same country, making for difficult interpretation. Thus, the mean daily neuroleptic dose of 600.0 (SD = 593.8) mg CPZ-eq for our patients was lower than the mean daily dose of 1049.0 (SD = 899.0) mg CPZ-eq/day received by Chinese patients with chronic schizophrenia in a report from Hong Kong [12]. Another survey of schizophrenic patients in a psychiatric unit of a general teaching hospital in Hong Kong reported a mean daily dose of 568.5 mg CPZ-eq/day [13]. Indicative reports from China suggest somewhat lower mean doses among schizophrenic patients: 430.0–465.0 mg CPZ-eq/day in a report from Hubei Province [4] and 311 mg CPZ-eq/day in a report from Shanghai [14].
Fifty-nine per cent of our patients were receiving two or more neuroleptics, which is close to the 54% rate for patients in Hong Kong [15] and 53% rate for patients in report from China [4]. These rates are higher than reported by Baldessarini et al. [16] in the USA (46% in 1989 and 24% in 1993), while Reardon et al. [17] reported that in the decade between 1973 and 1982, the practice of using concurrent neuroleptics ‘had all but disappeared’ in three settings in New York.
It has been suggested that depot antipsychotics have been underutilised in some countries, especially in the USA where only an estimated 10% to 20% of patients receive them [18]. In European countries, estimated rates vary from 20% to 60%, with an average of 20% taking some oral medications as well [19,20]. While 66% of our patients were receiving depot neuroleptics, 56% of them were also receiving one or more neuroleptics.
The reasons for using multiple neuroleptics are possibly varied and invite speculation. Some of the reasons suggested include the ‘unproven’ belief of the physicians that a combination of drugs is more effective [4] and the beliefs among patients that the more drugs prescribed, the better the effect [2]. It has further been suggested that polypharmacy in Asia is related to the principles of Oriental traditional medicine in which the best prescriptions include a mixture of various ingredients [3]. Unfortunately, this survey did not permit us to address this issue.
The majority (64%) of our patients were prescribed an anticholinergic agent. Prophylactic trihexyphenidyl is routinely prescribed by most of the psychiatrists in Woodbridge Hospital, and all patients not receiving trihexyphenidyl currently had done so sometime in the past. Patients not in receipt of this anticholinergic agent were older and also showed a greater severity of EPSE despite a significantly lower mean neuroleptic dose. There are two possibilities for these findings. The first is that anticholinergic treatment was stopped without subsequent monitoring of the patients who then developed EPSE. The second possibility is that EPSE may have re-emerged at a later stage as the patients aged. The risk factor most frequently associated with drug-related parkinsonism is increasing age [21].
Although we have compared patients of the same ethnicity and diagnosis, interpreting findings from different countries is limited by the differences in methodologies, subjects' demographics and differences in prescribing practices of physicians and the availability of drugs. As with all cross-sectional surveys, this study has the inherent limitations of any parochial study. Prien et al. [1] criticised this ‘scatter gun’ approach of collecting short-term prescription data with its preoccupation with what treatment is prescribed, and not why the treatment is being prescribed and under what circumstances. As such, we are unable to make any definitive judgement about the appropriateness of the prescribing patterns in this hospital. Nonetheless, some of the findings (e.g. the use of multiple typical neuroleptics, and marked under-utilisation of atypical neuroleptics) are of importance.
Our survey indicates that there is a need to have regular reviews of prescription practices in order to reveal discrepancies between standard recommendations and clinical practice. Efforts can then be made to educate clinicians and guide their practices according to evidence-based standards. There is also a need to examine policy issues that may impose constraints on clinical practice.
Acknowlegements
This study is partly supported by grants from the National Medical Research Council, Singapore (NMRC/0316/1998). We thank Professor Gordon Parker for his comments.