
Abstract
In childhood, mental health problems primarily consist of behaviour and emotional problems. These affect one in every seven children (i.e. 200 000 in Australia). Left untreated, up to 50% of preschool problems continue through the childhood years. Because of their high prevalence, population-based approaches will be needed to reduce their associated burden. The aim of the present study was therefore to identify evidence-based preventive interventions for behavioural and emotional problems of children aged 0–8 years. Randomized controlled trials of preventive interventions for behavioural and emotional problems were located by searching standard clinical databases and systematic reviews. The authors determined which programmes were effective and ineffective, dividing the effective programmes into those with high or low risk of trial bias. Among effective programmes, the most promising for delivery in Australian contexts were identified, selected for their strength of evidence, sample comparability to Australia's population, and programme compatibility with Australia's service system. Around 50 preventive interventions have been evaluated in randomized controlled trials. Most targeted children's behavioural problems, and a few targeted emotional problems. Three US programmes have the best balance of evidence: in infancy, the individual Nurse Home Visitation Programme; at preschool age, the individual Family Check Up; at school age, the Good Behaviour Game class programme. Three parenting programmes in England and Australia are also worthy of highlight: the Incredible Years group format, Triple P individual format, and Parent Education Programme group format. Effective preventive interventions exist primarily for behaviour and, to a lesser extent, emotional problems, and could be disseminated from research to mainstream in Australia, ensuring fidelity to original programmes. Future research should develop programmes targeting emotional problems, and replicate effective programmes for behaviour problems in quality population translation trials. Randomized trial methods in staged roll-outs can determine population cost–benefits for children's mental health without delaying dissemination.
In childhood, mental health problems primarily consist of behaviour and emotional problems. Australia's national youth mental health survey reported that behaviour and emotional problems affect one in every seven children aged 4–17 years (around 200 000 in Australia) [1]. Behaviour problems typically include oppositional defiance, hyperactivity and aggression. They are also known as ‘externalizing’ problems, because children show outward manifestations of the problem. Emotional problems typically include anxiety, withdrawal and depression. They are also known as ‘internalizing’ problems, because children experience inner emotional distress that may not be overt or obvious to others. Although children's mental health problems cluster in children from low socioeconomic families, the bulk arises in children from middle class families, simply because these families make up numerically more of Australia's population. For around 25% of children with problems, behaviour and emotional problems co-occur [1].
Many serious problems we see in adulthood (depression, substance abuse, family violence, criminality) have their origins in pathways that begin much earlier in life, often with childhood behaviour and emotional problems [2, 3]. Early childhood problems can establish developmental trajectories that become progressively more difficult to modify as children get older [4],[5]. Left untreated, around 50% of preschool children grow out of behaviour problems [6]. For the 50% who do not, long-term sequelae can include school drop out, family breakdown, and later adolescent and adult depression, drugs and alcohol abuse, and employment difficulty [7]. These sequelae have social and financial costs, such as clinical treatment services and suboptimal workforce participation, imposing a considerable cumulative drain on society and undermining Australia's productivity [8].
Cost–benefit studies show that intervening earlier in the life course is cheaper and more effective than later treatment [9]. It is biologically and economically more efficient to get it right the first time, than to attempt to fix things later on when problems are entrenched. But what is the best way to intervene early in children's behavioural and emotional trajectories? The aim of the present review was to provide evidence for this question.
Children's behaviour and emotional problems are in part inherited and in part due to the environment [10, 11]. Preventive intervention focuses primarily on optimizing the environment, with a view to managing or preventing the child's problem. Parenting style has been shown to be the single most important environmental factor to influence a young child's behaviour [10]. Harsh and abusive parenting contributes to child behavioural problems, while over-involved and protective parenting contributes to child emotional problems [10, 12]. Therefore, most preventive programmes try to optimize parenting styles [13]. The main goal of parenting programmes is to develop parents’ skills to identify, define, observe, and respond to child behaviours in new ways. Parents are helped to identify problem behaviours. They are taught to use positive reinforcement to encourage desirable behaviour, and non-punitive discipline techniques (such as ignoring and time-out) to discourage undesirable behaviour. Interventions also focus on positive parent–child relationship strategies. These include active listening, helping parents understand the ways in which children think and the motives for their behaviour, and warm sensitive responding to child distress and requests for interaction. During parenting programmes parents are encouraged to keep a record of their child's behaviour changes and undertake homework to practise new skills.
Some preventive programmes focus on different aspects of the child's environment, other than parenting. These include relationship with peers, teacher responses to child behaviour, and anger or anxiety management for the child. Multi-systemic models incorporate a package of different intervention programmes delivered across more than one service sector. This could include a child-directed programme in the school classroom accompanied by an outreach parenting programme in the home.
In 1994 Mrazek and Haggerty developed a theoretical model for mental health promotion conceptualizing eight possible gradients of intervention, from prevention through treatment and continuing care [14]. Preventive interventions are further divided into ‘universal’ (offered to the general public or a whole population group that has not been identified on the basis of individual risk); ‘targeted-selective’ (to individuals or a subgroup of the population whose risk of developing mental disorders is significantly higher than average); or ‘targeted-indicated’ (to high-risk individuals who are identified as having minimal but detectable signs and symptoms foreshadowing mental disorder, but who do not meet DSM-IV diagnostic levels at the current time). In reality these boundaries can overlap.
The aim of this systematic review was to identify evidence-based preventive interventions for behavioural and emotional problems of children aged 0–8 years, to inform policy planning for early childhood services. As aforementioned, behavioural and emotional problems are the primary mental health problems of childhood, affecting one in seven Australian children (similar rates reported internationally), with cumulative personal, societal and economic ramifications. It is therefore essential to consider effective early prevention for children at the population level. The review findings have implications for developing effective public health systems for youth mental health in Australia and New Zealand. In line with the Mrazek and Haggerty theoretical framework [14], for this review we defined prevention strategies as either universal programmes (offered to a whole population group that has not been identified on the basis of individual risk) or targeted programmes (offered only to at-risk samples of children, either selective or indicated risks). Treatment trials for diagnosed child mental health disorders or children receiving clinical mental health services were not defined as early prevention.
Method
Identification of trials
We identified randomized controlled trials (RCTs) as the gold standard methodology to assess a programme's effectiveness. RCTs were identified from a variety of sources including standard clinical databases, published systematic reviews, and hand searching of key articles. The following studies were included in the review: RCTs; sample with child mean age < 9 years; and outcomes of behaviour or emotional problems assessed on standard measures. The following studies were excluded as ineligible in the review: narrow behavioural or emotional outcomes (e.g. fire setting, specific fear of snakes); post-intervention follow up length <6 months; sample primarily consisting of children with a clinical diagnosis of a mental health problem, and/or trial taking place in tertiary/clinical setting.
Eligible RCTs were identified using the following search strategy (Appendix I). We searched published abstracts in the databases of Medline, PsychInfo and Cinahl from 1995 to 2007 via MESH search terms (defining populations, outcomes, interventions). This identified 3827 abstracts. We next hand-searched the abstracts to exclude non-RCTs (key words randomi/ze or controlled), drug trials, samples of children primarily >8 years, clinical treatment of diagnosed disorders, and short post-intervention follow up (<6 months). We further hand-searched 18 recent relevant reviews, published between 1996 and 2007 and incorporating trials from the 1960s onwards, for any RCTs meeting our review criteria [13], 15–30.
Quality ratings
Although RCTs are considered the gold standard assessment of a programme's effectiveness, they can still have problems in design or analysis that weakens their findings. We therefore ranked the quality of each RCT using the Australian National Medical Health and Research Council (NHMRC) recommendations from their 2000 report [31] and guidelines of the 2006 Cochrane handbook of systematic reviews[32].
We assessed quality in four areas: method of treatment assignment; control of selection bias after treatment assignment; blinding of outcome assessment; and quality of outcome assessment. Bias can occur in any of these areas and can affect the interpretation of the study's results. Random allocation of families to the intervention or control arm of a trial is essential, because parents of children with more problems may seek out the intervention if given a choice. Similarly, losing >15% of the study sample after treatment assignment, or failing to report the effectiveness of the intervention according to how the intervention was received, can artificially inflate an intervention's effectiveness. If families of children with more behaviour problems tend to drop out of the intervention arm of a study, this will disproportionately leave families of children with relatively positive behaviour. The intervention can then appear more effective than it really is. An intention-to-treat analysis means that the outcomes are analysed according to the way children were initially randomized (i.e. the way they were intended to be treated). Serious trial bias can occur if this does not happen. If some children from the intervention group do not receive the intervention (as often occurs in real life) but the trial reports only on those who did receive the intervention, then effectiveness can again be artificially inflated.
Unlike drug trials, outcome assessments for child behaviour intervention studies almost inevitably are not completely blinded. This is because most key outcomes are reported by parents. Parent report is the most appropriate, the most feasible, and the most common outcome source in preventive intervention trials for child behaviour and emotional problems. But parents are not blinded because they are usually aware whether or not they or their child have received an intervention. We therefore decided not to include this assessment criterion in our overall quality rating of each trial because it would not be discriminatory. Nevertheless we recorded whether trials had partial blinding (at least one outcome assessor was blind to the child's group allocation, e.g. teacher or independent observer) or no blinding (no outcome assessors were blind to the child's group allocation). Likewise because all studies included a standardized assessment of the child, we decided not to include this assessment criterion in our overall quality rating of each trial.
Our final quality rating for each RCT was therefore based on the first two criteria scores (method of treatment assignment, control of selection bias after treatment assignment). A trial was designated as having low risk of bias if these first two criteria were fully met; moderate risk of bias if the first two criteria were partly met; and high risk of bias if the first and/or second criteria were not met [32].
We next selected specific effective programmes that we considered to have the most potential for application in Australia's population context. Here we considered the Biglan et al. guidelines on evidence to support programme uptake [33]. Biglan et al. recommended promoting adoption of programmes that show effectiveness in two or more RCTs ideally conducted by independent research teams. Because very few programmes meet these criteria, we rated each preventive intervention programme as effective if there was one or more RCT showing effectiveness on child behavioural or emotional outcomes, or ineffective if the programme's sole RCT showed it was ineffective on child behavioural or emotional outcomes. We selected effective programmes as applicable for the Australian context, by taking into account the number of trials demonstrating effectiveness, comparability of trial samples to Australia's population, trial quality, length of follow up, and intervention duration/intensity as a broad indicator of cost and potential fit into Australia's service system. Formal economic evaluations have rarely been conducted to provide extensive costings, and the few conducted are difficult to directly compare due to different metrics used.
Review results
Overview of effectiveness for all programmes in review and child outcome, vs child age
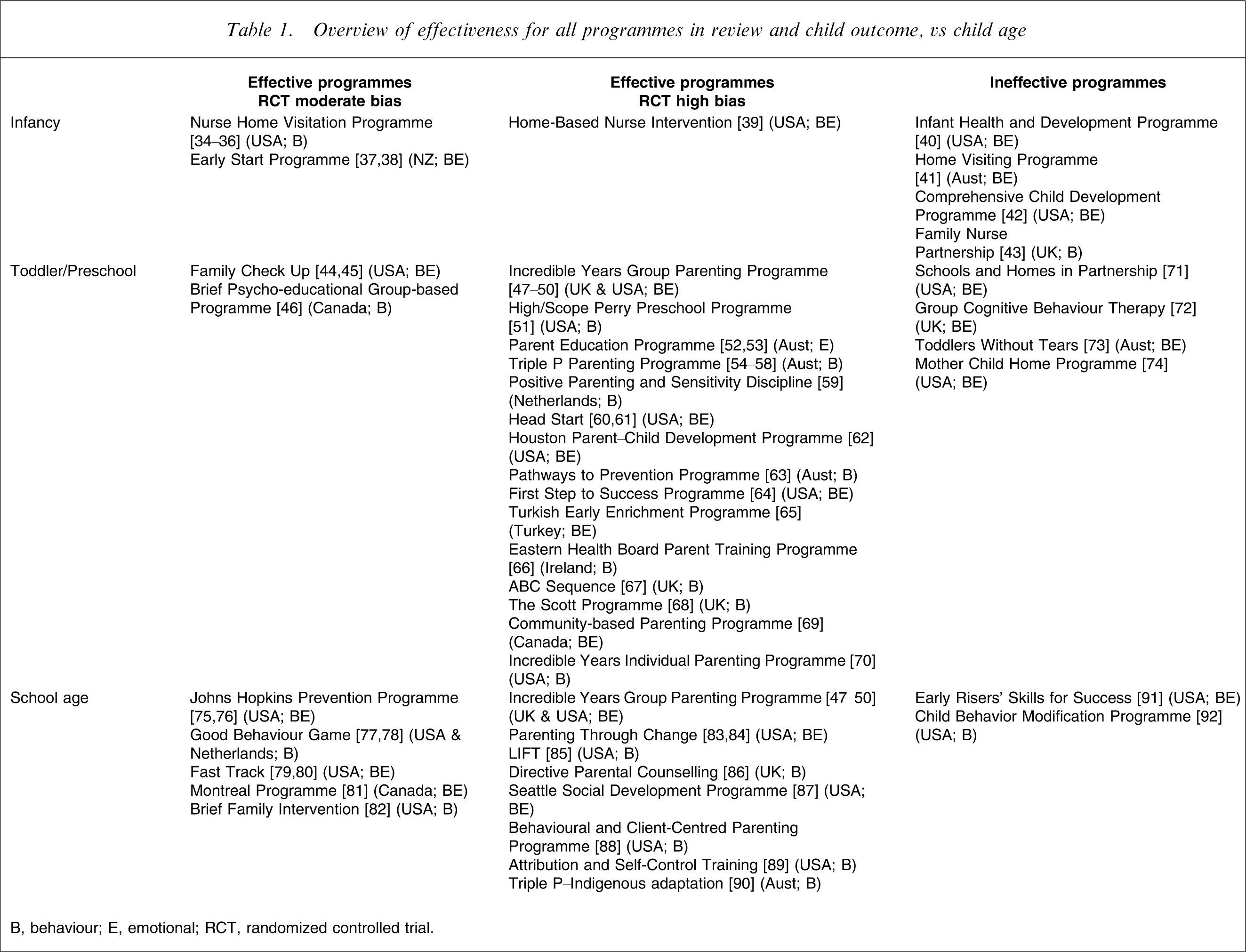
B, behaviour; E, emotional; RCT, randomized controlled trial.
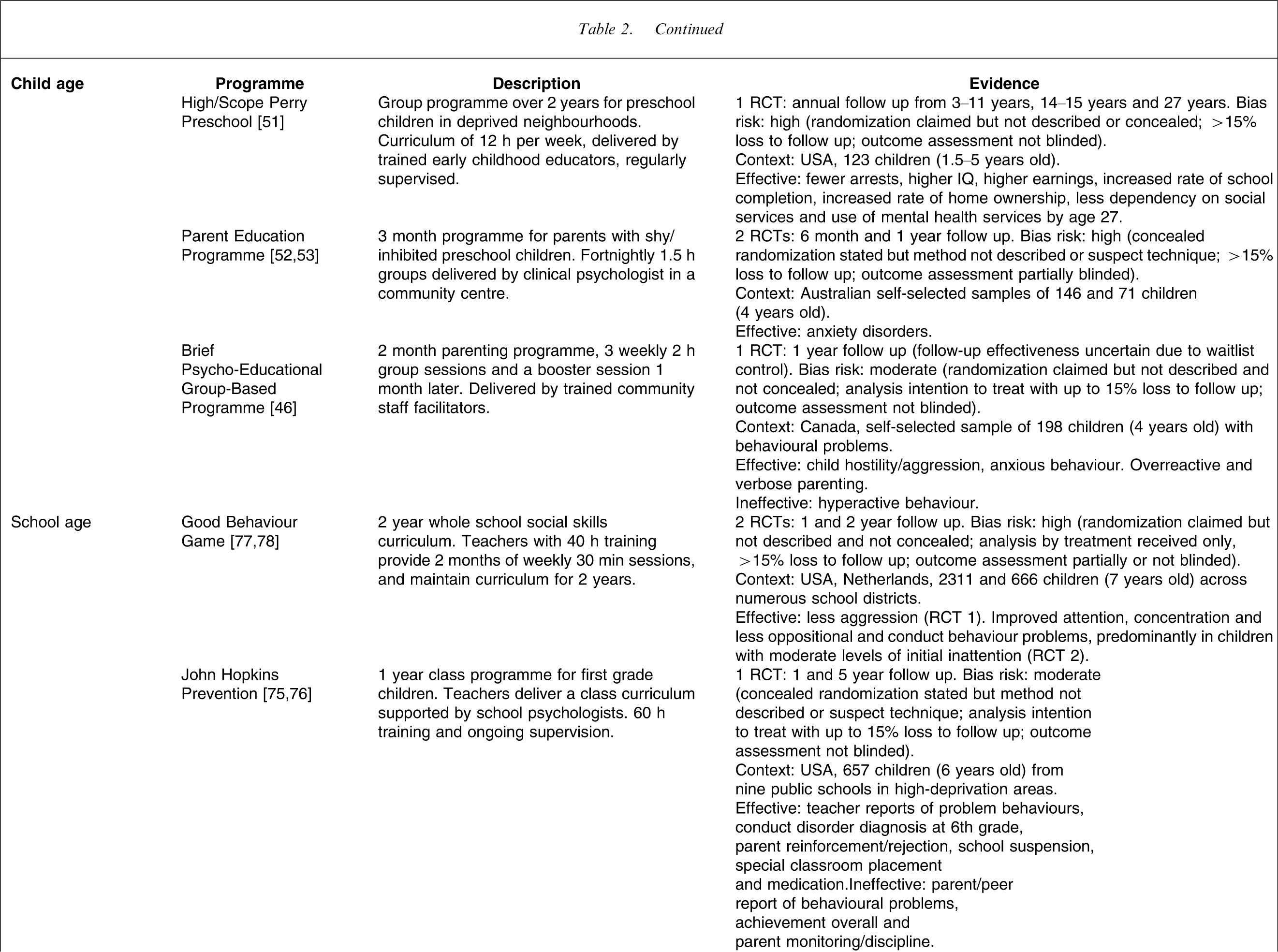
Effective preventive interventions for child behaviour and emotional problems, considered applicable for Australia
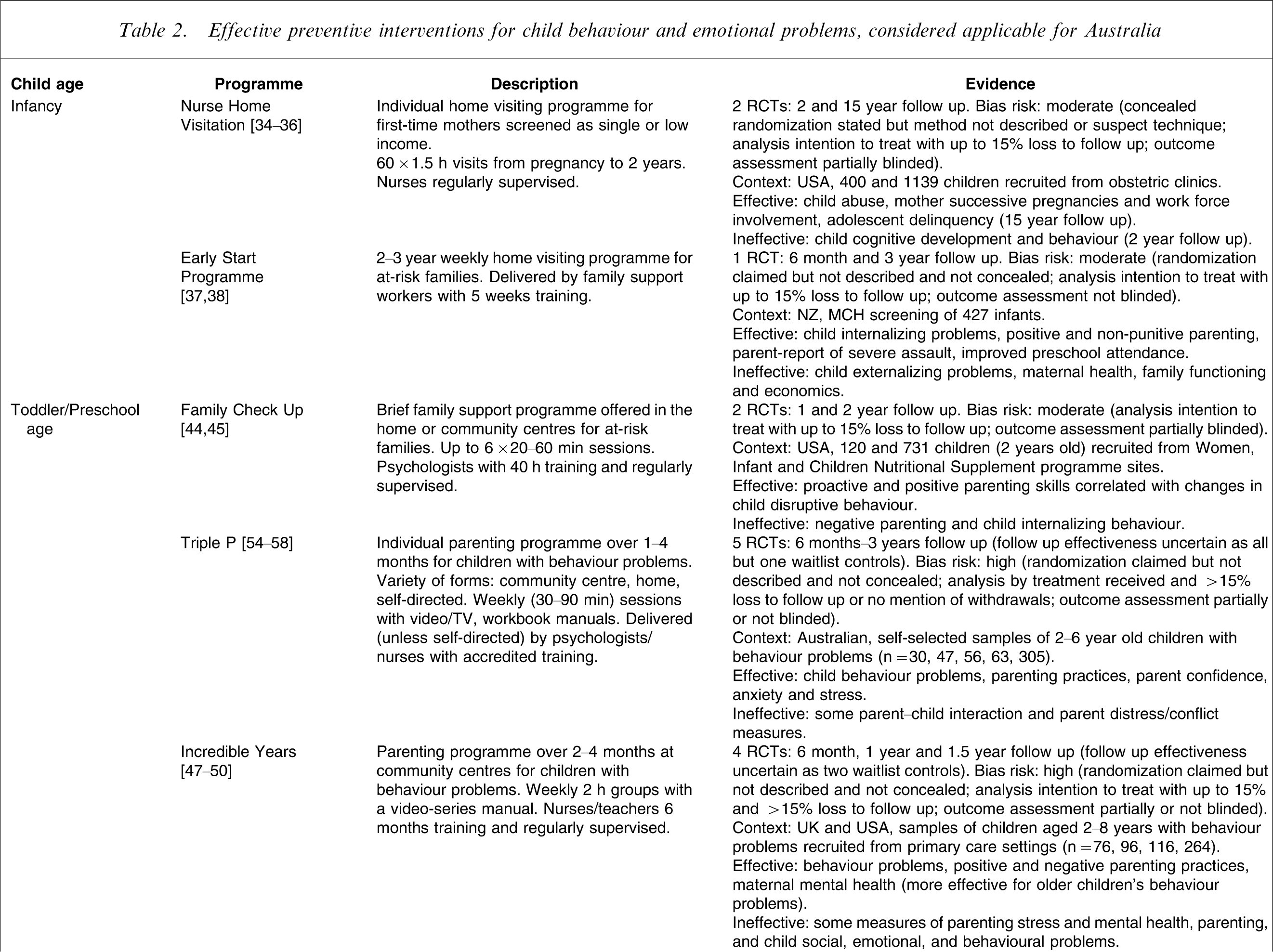
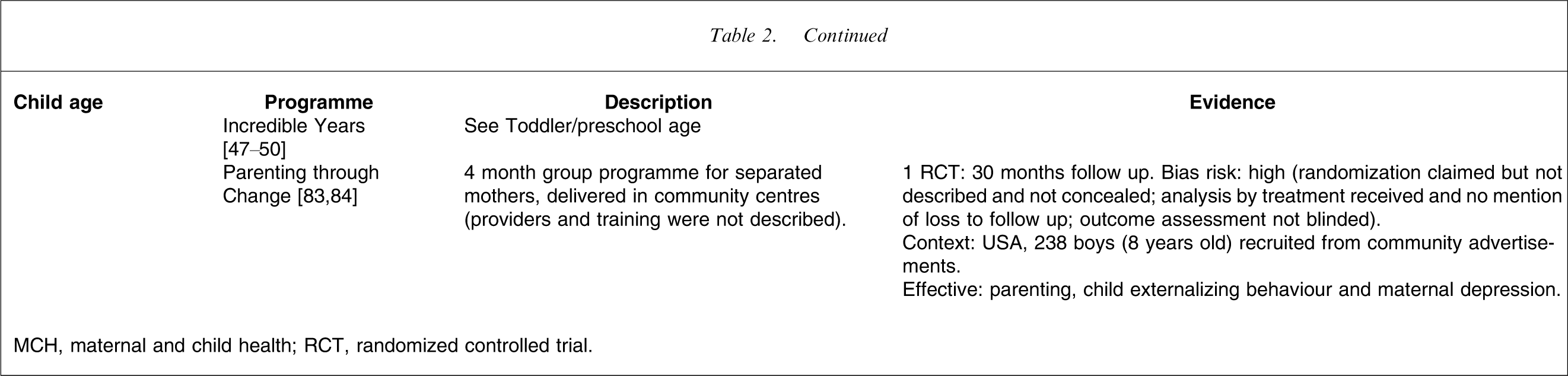
MCH, maternal and child health; RCT, randomized controlled trial.
Best preventive interventions for Australia's context to reduce child behaviour problems
Infancy
The US-based Nurse Home Visitation Programme has the best balance of long-term evidence for reducing child behaviour problems 34–36. This is a targeted individual home visiting programme delivered over 2 years to low-income, unmarried, first-time mothers. Two high-quality RCT evaluations were conducted in the USA, with large sample sizes and an extended follow up to 15 years. This programme was effective for reducing adolescent behaviour problems as well as parenting abuse. Service requirements for delivery are screening for risk in obstetric clinics, followed by up to 60 90 min home visits from pregnancy to age 2 years, by nurses receiving regular supervision. Cost-effectiveness was demonstrated at $US 1582 per family. We considered this programme to be feasible for dissemination in the Australian context. We caution, however, that individual home visiting is likely to be more costly to implement than other effective programmes we recommend that are delivered in groups. In addition, we caution that this home visiting programme's outcomes may be less effective in Australia than in the USA, given higher US deprivation levels compared to Australian families, along with better existing universal services and resource infrastructure in Australia.
We did not recommend another US targeted-selective Home-Based Nurse Intervention delivered over 1.5 years that was effective for child behaviour [39], because that trial had high risk of bias. We also point out that several other targeted-selective individual infancy home visiting programmes delivered in Australia [41], New Zealand [37, 38], the UK [43], and the USA [40, 42] were found to be ineffective for child behaviour. These home visiting studies included a measure of child behaviour problems and found that intervention was ineffective on that outcome.
Preschool
Commencing at preschool age, we recommend three targeted preventive interventions with the best balance of evidence for reducing child behaviour problems as most potentially applicable in the Australian context. First, the US Family Check Up is a brief (approx. three sessions) targeted (selective/indicated) family support programme offered individually at home or community centres to mothers with toddlers [44, 45]. Two high-quality RCT evaluations were conducted in the USA with high-deprivation families (urban, suburban and rural communities). This programme was effective in preventing preschool behaviour problems via improving parenting. Service requirements include screening for family risk when children are between 2 and 3 years of age. Those at risk are then followed by up to six contacts (20–60 min face to face or telephone) according to family need and desire (mean of three contacts), by psychologists with training and supervision. This programme appears to be feasible for the Australian context, but requires 40 h of training and ongoing supervision, and it has not yet been trialled in Australia.
Second, Triple P is a targeted (indicated/selective) parenting programme delivered over 1–4 months individually to parents of children with behaviour problems via a variety of formats (community centre, home, self-directed) 54–58. Five RCT evaluations have been conducted in Australia, although all had high risk of bias (Table 2). In addition, four trials used waitlist controls who were then offered the programme within a few weeks, so that long-term efficacy beyond this time is difficult to determine. Nevertheless, this programme appears to be effective for behaviour, parenting and stress outcomes. Service requirements are 8–10 weekly (30–90 min) sessions with video/TV and workbook manuals, delivered (if not self-directed) by psychologists or nurses with extensive accredited training. This programme is directly applicable to Australian contexts in that it was developed and evaluated in Australia. Limitations of the Triple P trials, however, are their self-selected samples (meaning that parents volunteer interest, rather than being systematically recruited to ensure population representation), and waitlist control design that provides no comparison control data beyond a few weeks on programme effectiveness.
Third, the Incredible Years Group Parenting Programme is delivered over 2–4 months at community centres targeted (indicated) to parents of children with behaviour problems 47–50. Two RCT evaluations at preschool age with high risk of bias (Table 2) and follow up to 1.5 years were conducted in the UK and USA. In early childhood this programme was effective for some child behaviour, parenting and parent mental health outcomes. Service requirements are 10–16 weekly 2 h parenting groups, delivered with a video-series manual, by nurses and teachers trained for 6 months and supervised by a psychologist. Cost to implement was £571 per child. Incredible Years is likely to be suitable for the Australian context because it has been shown to be effective in two similar modern Western countries (UK, USA) and the available cost data indicate that wider implementation is likely to be feasible.
Triple P and Incredible Years are the most widely known and respected preventive interventions for child behaviour problems in the field. We recommend both of these programmes as applicable for the Australian context for the following reasons. Triple P's strengths are as an Australian developed and researched programme that has been evaluated in five randomized trials. Triple P's limitations regarding large-scale dissemination are that these trials had significant quality concerns, they lack strong long-term outcomes, and the parenting programme was delivered individually using a different format in each trial. Incredible Years’ strengths are that it is a parenting programme delivered in groups, designed for well-child service systems, evaluated in four randomized trials, in two Western countries similar to Australia (UK and USA). Incredible Years, however, was more effective for school-age than younger children, and the trials also had quality concerns.
Two additional preschool age programmes had promising effectiveness but we would not recommend them strongly for the Australian context. The High/Scope Perry Preschool Programme was a targeted-selective educational group programme (child-initiated learning) delivered over 2 years in deprived US neighbourhoods [51]. One RCT evaluation with high risk of bias but extended follow up to 27 years found that this programme was effective in the long term for behaviour (arrests), increased life standards and reduced dependency on welfare services. Service requirements for fidelity of delivery are a preschool curriculum of 12 h per week, delivered by trained early childhood educators with ongoing supervision. Cost-effectiveness has been demonstrated (and quoted very widely), with $US 7 lifetime return for every dollar invested, but the programme was carried out in North America in the 1960s and findings may not hold for Australia in the 2010s.
Positive Parenting and Sensitivity Discipline’ is a targeted-indicated brief (3 month) individual programme showing effectiveness for behaviour [59]. We do not recommend this programme strongly for the Australian context because the trial had high risk of bias, required extensive training (170 h), and had fewer effective outcomes.
School age
Four early intervention programmes had the best balance of evidence for reducing school-age children's behaviour problems. We considered the first two as most applicable for the Australian context. The first, Good Behavior Game, is a universal 2 year, whole of school, social skills curriculum [77, 78]. Two RCT evaluations with large sample sizes have been conducted in different countries (USA, Netherlands; one high quality, one with risk of bias). This programme effectively reduced aggression and oppositional/conduct problems. In recommending application in the Australian context, teachers would need to establish this programme in their class via 2 months of weekly 30 min sessions, and then maintain this curriculum for 2 years. Teachers require 12–40 h training before commencement.
The second, the Incredible Years Group Parenting Programme (as reported in the previous section) is a brief (3.5 month) programme targeted at children already showing behaviour problems 47–50. Two RCT evaluations were conducted with school-age children from low socioeconomic status families, both with high risk of bias and use of waitlist controls, so effectiveness beyond a few weeks is uncertain. Nevertheless, this programme appears effective for school-age behaviour and parenting outcomes.
The Johns Hopkins Prevention Programme was a targeted-selective 1 year class programme for first grade school children, delivered to all classes within participating schools in high-deprivation areas [75, 76]. One high-quality RCT evaluation was conducted in the USA. This programme reduced 6th grade conduct disorder, as well as teacher reports of behaviour problems, school outcomes (special education, suspensions) and improved some aspects of parenting. Although this intervention was effective, it has only shown effectiveness in US high-deprivation areas, and considering the Australian context it would place high demands on teachers. Service requirements are that teachers deliver a 1 year class curriculum supported by school psychologists, including undergoing 60 h training and ongoing supervision.
Parenting Through Change is a brief (4 month) programme targeted (selective) to separated mothers with boys [83, 84]. One RCT evaluation with 2.5 year follow up (but high risk of bias) found that this programme was effective for behaviour, parenting and maternal depression outcomes. The intervention was delivered in community centres, but providers and training were not described. We would not prioritize dissemination of this programme in Australia's context because separated mothers with boys is a very narrow risk group and therefore this programme would miss many other children in need in the community.
The following additional programmes at school age also showed effectiveness but were not recommended for the Australian context. Although the US targeted-selective Fast Track programme had a high-quality trial showing effectiveness for some behaviour, social–emotional, and parenting outcomes, it is an intensive 5 year intervention evaluated only in high-deprivation areas of one country [79, 80]. Similarly, Linking the Interests of Family and Teachers appears to be a relatively brief (2.5 month) teacher-delivered group programme at targeted schools, showing effective behaviour and social outcomes [85]. We steered away from recommending this programme in Australia because the trial with deprived US families had high risk of bias, and intensive participation from families is required (20 child and six parenting sessions).
Best preventive interventions for Australia's context to reduce child emotional problems
In this review relatively few preventive interventions specifically attended to emotional problems. The first three were considered most applicable for the Australian context.
Infancy
Early Start, a 2–3 year targeted-selective individual home visiting programme in New Zealand for at-risk and stressed mothers, had the best balance of evidence for reducing emotional problems from infancy [37, 38]. One high-quality RCT evaluation with 3 year follow up was conducted, effectively improving child internalizing problems, parenting (including abuse) and preschool attendance. Services in primary care screened all families for risk, and then coordinated weekly home visits by family support workers given 5 weeks training. This individual home visiting programme is more costly than group programmes, but could be directly applied to Australian and New Zealand contexts (more so than the aforementioned US Nurse Home Visitation Programme34–36), given comparable maternal and child health systems and deprivation levels.
Preschool
Two targeted-indicated programmes had the best balance of evidence for reducing emotional problems. The Parent Education Programme is a 3 month group programme for parents with shy/inhibited preschool children [52, 53]. Two RCT evaluations with 6 month and 1 year follow up (but high risk of bias) were conducted in Australia, and effectively prevented child anxiety disorders. This programme requires screening in community preschool settings for shy/inhibited children, followed by fortnightly 1.5 h parenting groups, delivered by a clinical psychologist at a community centre.
The Brief Psycho-educational Group-Based Programme is a 2 month group programme for parents of children with behaviour problems [46]. One high-quality RCT evaluation was conducted in Canada with a self-selected sample. Although targeting behaviour problems, this programme also reduced child anxiety and improved parenting. The waitlist control design, however, means that effectiveness beyond a few weeks is uncertain. Service provision consists of three 2 h sessions delivered weekly with a booster 1 month later, delivered by trained community staff facilitators. Although this community programme could be feasible in Australian contexts, longer term effectiveness needs to be established.
School age
Fast Track was a US programme evaluated in a high-quality trial that showed some impact on children's social–emotional skills [79, 80], but this was an intensive 5 year targeted-selective intervention delivered in high-deprivation US areas. Further, the improved social–emotional skills documented may not actually translate into less child internalizing problems. For these reasons we would not recommend this programme for child emotional outcomes in the Australian context.
Conclusions
Effective preventive interventions exist for young children's behaviour and emotional problems. Around 50 programmes have been evaluated in RCTs. Most programmes were targeted to at-risk children, with selective environmental and/or indicated behavioural risks. Most programmes focused on children's behavioural problems, and only a few attended to emotional problems. Three US programmes have the best balance of evidence as well as potential applicability for the Australian context: in infancy, the targeted (selective) individual Nurse Home Visitation Programme 34–36; at preschool age, the targeted (selective/indicated) individual Family Check Up [44, 45]; and at school age, the universal Good Behaviour Game class programme [77, 78]. Three targeted (indicated) parenting programmes in England and Australia are also worthy of highlight as applicable in Australia: The Incredible Years group format 47–50; Triple P individual format 54–58; and the Parent Education Programme group format [52, 53].
The results of this review could inform a whole-of-early-childhood framework for effective early intervention that assists policy development. Via universal screening, families under significant stress could be identified at birth and offered a home-based support programme to supplement existing universal primary care services through infancy and toddlerhood. At age 2–3, further universal screening/surveillance could identify families who could benefit from a targeted programme of individualized family support or a group parenting programme. At age 5–7, children could receive a classroom child-directed programme, with links to parenting groups in the local community for families identified as in need.
Cost and implementation
Few studies have reported economic evaluations for early intervention programmes. The few that have do not use comparable assessment metrics. This makes it difficult to directly compare the cost of one programme with another. Typically evaluations focused on implementation service costs, such as training, programme materials and salaries for programme providers. Costs to families (e.g. time off work, transport costs) are often not included. A minority of projects have calculated the health and welfare service costs saved from implementing a targeted intervention (e.g. Perry Preschool Programme [51], Nurse Home Visitation 34–36) while others have reported on the costs of implementing the programme only (e.g. Incredible Years 47–50). Overall considering the available cost data, for high-risk families, there seems to be a good return on investment [9], 34–36, 47–51. Cost and implementation are likely to be similar in Australia and New Zealand, given comparable maternal and child health systems and deprivation levels. In this systematic review, noting cost data that has been reported to date in studies offers policy makers some information. In addition, emphasizing in this review the limited amount and comparability of cost data across studies highlights the need for all future trials of preventive programmes to build in formal economic evaluation procedures from the outset.
Preventive interventions in this review took place in a variety of settings (family homes, community health centres, child care centres, schools) and were delivered by a range of providers (community health workers, nurses, psychologists, psychiatrists, teachers). Multi-systemic approaches with a package of different interventions delivered by more than one service sector are likely to be most costly to implement (e.g. teachers delivering social skills training to children at school, plus psychologists delivering parenting education at home). Individual approaches delivered one on one by a professional to each family (e.g. nurse home visiting) are likely to be moderately costly to implement, given that families are seen separately and sometimes over substantial time periods. Group approaches (delivered to parents or children) are likely to be the least costly (estimates indicate eightfold less) [13, 69]. The reach, however, of group programmes might be lower, because it is unlikely that all parents in the population are willing to attend groups. In a recent trial of a prevention programme offered to all families attending their maternal and child health nurse in nine socioeconomically diverse areas of Melbourne [73], 69% of parents consented to take part in group parenting programmes.
To widely disseminate effective preventive interventions, Giesen et al. note the following important principles [93]. Programmes should have staff who are properly trained and who adhere to the programme content. Intervention dosage (such as attendance at sessions) should be maximized by providing out-of-hours sessions for working parents and on-site childcare where possible. Programme delivery should be sensitive to different cultures and at-risk populations. Programmes are more likely to be accepted by service providers and taken up in the real world when they have proven effective or cost-effective outcome data; synchronize with the adopter's values, past experience and perceived needs; are simple to understand; are easy to adapt into the organization; have transferable knowledge to other contexts; and supply training and a help desk. When prevention programmes are adapted into new settings, it is essential that a professional consultant who is experienced with the programme works closely with the new providers, to ensure that components essential for effectiveness are maintained while minimal aspects of the programme are being tailored to local needs.
This systematic review has the following strengths. The review process was a detailed, systematic search of key databases for preventive programmes, throughout early childhood (birth to 8 years), across broad behaviour and emotional outcomes, directly relevant to childhood mental health. Only evaluation trials with a rigorous prevention evaluation (RCTs with at least 6 month follow up) were included. Service delivery aspects of evidence-based programmes were highlighted in the review for policy makers in Australia and countries with similar primary care systems. The review also had the following limitations. It was not a meta-analysis, which calculates comparative effect size statistics for each trial to make direct outcome measure comparisons. The review did not follow a formal (i.e. Cochrane) procedure, in which two reviewers cross-evaluate a pre-set proportion of articles and unpublished research reports may also be sought.
Further research
Over 30 years a large evidence base has been accumulated for at-risk targeted intervention/prevention for children's behavioural problems. Since the 1990s, recognition has grown that childhood emotional problems exist and can be very debilitating, and a small evidence base has been developed in response. We believe that further research is urgently needed on early prevention for emotional problems, because there is a paucity of effective programmes. As a priority we suggest a population-level RCT for the Australian Parent Education Programme [52, 53]. This programme has advantages of being brief (3 months), and being the first programme to target shy/inhibited preschool children in the community and prevent later anxiety disorders. For behaviour problems, we recommend pairing an independent replication trial in Australia or New Zealand with population dissemination of programmes having the best balance of evidence and potential applicability in these countries’ existing service systems. We suggest prioritizing dissemination trials of the following briefer programmes with promising effectiveness: Family Check Up [44, 45]; Triple P 54–58; Incredible Years 47–50; and Parenting Through Change [83, 84]. Briefer programmes are less demanding on families to facilitate uptake, as well as more cost-efficient to deliver.
Dissemination trials in Australia and New Zealand should be careful to recruit at-risk groups as part of their population samples when taking a universal primary care approach to children's mental health (i.e. parents with mental health and substance use problems, indigenous families, housing vulnerable families). Long-term effectiveness data need to be collected for all the brief targeted programmes recommended and this requires sufficient research funding (≥5 years). Although waitlist control designs may be palatable to families, they hamper building of the knowledge capacity of unbiased long-term data. Wide-scale and necessarily costly implementation of new programmes will be more sustainable over time when backed by data on long-term outcomes comparing intervention with control groups. In dissemination RCTs families remain free to access existing services in their community. In dissemination research new preventive programmes should demonstrate effectiveness over and above existing services to justify their wide translation. To assist policy makers with resource management and decision making it is critical that future dissemination research builds in economic evaluation to accompany measured mental health outcomes for children and their families.
Footnotes
Appendix I. MESH search terms (Medline)†
‘(humans and english language and (‘newborn infant (birth to 1 month)’
[Or ‘infant (1–23 months)’, ‘preschool child (2–5 years)’, ‘child (6–12 years)’]
neurotic disorders
aggression
anxiety
separation
Child Behavior Disorders
Mood Disorders
Social Behavior Disorders
Antisocial Personality Disorder
‘Attention Deficit and Disruptive Behavior Disorders’
primary prevention
intervention studies
‘Early Intervention (Education)’
preventive health services
treatment outcome
parents or parenting
health education/or family therapy
parent–child relations
child rearing
Parents with mental illness or drug/alcohol problems
child of impaired parents/
Homeless/housing vulnerable/poverty
homeless persons
poverty
Chronic illness
chronic disease
Culturally and linguistically diverse (including refugees)
culturally and linguistically diverse
refugees
culture
ethnic groups
minority groups
language
Aboriginal or Torres Straight Islander
aborigines or ‘torres strait islander’
oceanic ancestry group
australia
Rural
rural population
rural health
rural health services
Language/learning difficulties
language disorders
learning disorders
developmental disabilities
Autism and spectrum disorders
asperger syndrome/or autistic disorder