
Abstract
The effect of marital discord on the psychological well-being of children has been well documented, and interparental conflict is recognized as a risk factor for many child behavioural and emotional problems [1–6]. Understanding of the impact of the marital relationship on children, however, has been limited by the use of measures of marital functioning that have tended to focus on relationship quality and satisfaction [7].
Results from several studies suggest that children who witness marital conflict have an increased vulnerability in many areas of functioning including self-esteem [8], parent–child relationships [9, 10], social functioning [11], and psychopathology [12, 13]. Davies and Cummings proposed that the nature of the effect of conflict on children, functions through the child's sense of emotional security [14]. Children exposed to marital conflict may be emotionally insecure as a result of feelings of anxiety and fear in relation to their own relationship with the parent, as well as to the stability of the interparental relationship. In addition, the authors suggested that emotional insecurity may also develop because of a reduced capacity to effectively regulate emotions as a result of exposure to conflict.
Parental disagreements about child-rearing
An increasing number of studies have shown that conflict specific to parenting may be more detrimental than other sources of conflict that do not involve the child [15–17]. Grych and Fincham argued that parental conflict that is frequent, poorly resolved, intense and child-related is more damaging to the children who witness these arguments than those conflicts that are resolved amicably and do not involve child-related topics [18]. Jouriles et al. found evidence that parental disagreement over child-rearing was a better predictor of child behaviour problems than global marital adjustment, indicating that marital conflict specific to child-rearing may be more damaging to the development of children and potentially explains more of the variance in childhood problems than general marital conflict or marital dissatisfaction [15].
Many studies have relied on measures of marital quality or marital satisfaction, rather than parental conflict [2, 9, 19]. Global measures of marital satisfaction are simply too broad and do not adequately consider the context or characteristics of the parental relationship or the marital discord that affects children [2, 15, 20]. The nature and context of the marital problems may have differing effects on children and it is important to determine the specific dimensions of the marital relationship that are related to negative child outcomes [21]. For that reason, it would be beneficial to use measures that include child-rearing conflict when assessing the relationship between marital functioning and children's behaviour problems. Assessment of child-rearing conflict may lead to a better understanding of the relationship between marital functioning and child behaviour problems. Additionally, measures of conflict specific to child rearing may be used to highlight areas of difficulty and family functioning issues that can guide the development and implementation of effective interventions.
Parent Problem Checklist: measure of parent conflict
Despite the evidence that conflict specific to parenting is more strongly associated with negative child outcomes, there are few measures that directly assess parenting disagreement, and many studies still rely on measures of relationship conflict and satisfaction. Many of the existing measures of parenting conflict have limitations that threaten their utility in research and clinical practice. For example, the Interparental Conflict Questionnaire (IPQ) is a 20-item scale designed to assess conflict regarding both spouse (finance, sexual relations etc.) and child-related (chores, discipline) issues in terms of frequency, intensity, whether the conflict was witnessed by the child and how often discussion of the topic led to arguments [22]. Forehand and McCombs found that despite the measure having sound face validity, it does not have well-established test–retest reliability, with five out of eight subscales having reliabilities of <0.41 [22]. On the child-related issues subscale, the measure could differentiate between married and divorced parents only with regards to how often issues were discussed, as would be expected after the dissolution of a relationship and subsequently less contact between parents. The IPQ could not differentiate between divorced and married couples on any other factors of the child subscale. The O'Leary–Porter Scale was devised to examine conflict style and disagreement in couples [23]. It is a 20-item scale (containing only nine items that are scored) that assesses how often differing forms of conflict such as sarcasm and verbal aggression are witnessed by children. Neither of these scales contain clinical cut-offs that classify cases as falling within normal or clinical ranges, or measure whether issues are perceived as problematic by the parents.
In contrast, the Parent Problem Checklist (PPC) was devised in an effort to clarify the individual contributions to child adjustment problems made by parenting conflict [1]. Compared to other measures of marital conflict, the PPC assesses parent conflict in terms of parents’ ability to agree and cooperate when performing parenting duties within their families. The PPC has various advantages over other currently available measures of marital conflict. In addition to addressing child-rearing issues, the PPC displays good reliability, the ability to distinguish between clinically distressed and non-distressed couples and, at only 16 items, is shorter in length than most measures. Dadds and Powell found that parent conflict as measured on the PPC was a better predictor of aggression in children than the Dyadic Adjustment Scale (DAS), a widely used and well-established measure of marital conflict [1, 24].
Although there is some evidence for the utility of the PPC, it has not been widely examined and therefore it has limited evidence of validity, and no descriptions of the scale's factor structure. Although there is considerable evidence of the need for brief measures of parent conflict, more investigation of the properties of the PPC to further establish the validity and reliability of the measure as well as to examine the factor structure would be useful to both research and clinical practice.
Aims of the present study
Given the methodological considerations mentioned here, the aims of the present study were threefold: first, to further validate the psychometric properties and examine the factor structure of the PPC; second, to examine the validity of the measure by comparing it to well-established measures of conflict and relationship quality; and third, to examine the individual contribution of conflict specific to child-rearing issues assessed using the PPC to the prediction of child problems, in order to further assess the validity of the PPC. It was hypothesized that conflict regarding child-rearing issues as assessed by the PPC would be a better predictor of child difficulties than either marital satisfaction or global marital conflict, over and above the effects of demographic factors.
Method
Participants
Participants in the present study were 200 parents with a target child between the ages of 2 and 16 years (mean=8.69 years, SD=3.45). Of these participants, there were 186 mothers (93%), 10 fathers (5%), two stepmothers (1%), one stepfather (0.5%) and one foster mother (0.5%). Parents were recruited through advertisements in school newsletters and all parents participated on a voluntary basis. The children consisted of 112 boys (56%) and 88 girls (44%). In view of the research questions, parents were required to be in a relationship and were sharing the responsibility of parenting with their partner. The sample primarily consisted of Caucasian families (93%), with smaller proportions of other ethnic groups (2.5% Asian, 0.5% Aboriginal or Torres Strait Islander, and 4% no ethnicity given).
The majority of children (83%) lived in their original family, 15% lived in a stepfamily and 2% did not respond. The majority of parents were from intact marriages (81.5%), with a smaller proportion in a de-facto relationship (18.5%). In addition 90.5% of the parents in the sample felt at least moderately capable in their role as parent, 75% felt at least moderately supported in their role as parents and 87.5% felt at least moderately supported by their partner in their parenting role. Parental education was evenly spread, with 41.5% university educated, 23% with college qualifications, 3% trade educated, 13% high school only, and 19.5% not completed high school. In terms of annual income, 2.5% had an annual income of <AUD$25000, 44% had an annual income between AUD$25001 and AUD$75000, 45% had an annual income between AUD$75001 and AUD$150000, and 7.5% had an annual income >AUD$150001.
Measures
General marital satisfaction
The Relationship Quality Index (RQI) consists of six items that measure global relationship satisfaction that can discriminate between clinical and non-clinical couples [25]. In the present sample the scale was found to have a high level of internal consistency (α=0.95). The first five items assess relationship strength, stability and satisfaction on a 7-point scale ranging from 1=very strongly disagree to 7=very strongly agree. The final item assesses overall happiness of the relationship on a 10-point scale ranging from unhappy (1 point) to perfectly happy (10 points). The measure generates a total score from 6 to 45, with a cut-off of ≤29 indicating a clinically elevated level of dissatisfaction in the relationship. The index is correlated with the DAS [24].
General marital conflict
The Spanier Dyadic Adjustment Scale–Consensus Subscale (DAS-CS) assesses disagreement across various areas of the relationship but does not contain any items that assess disagreement over child-rearing [24]. The DAS-CS contains 15 items that assess agreement or disagreement on topics that are common to most relationships including finances, religion, sexual relations, shared goals, career decisions, household chores and leisure time. Each item is rated on a 6-point scale ranging from 5=always agree to 0=always disagree. Items are summed to an overall score of between 0 and 75, which can reliably distinguish between distressed and non-distressed couples [26]. In the present sample the scale displayed high internal consistency (α=0.91).
Interparental conflict
The PPC is a 16-item questionnaire measuring conflict between parents specifically relating to child-rearing practices, and their abilities to cooperate as parents, including disagreement over household rules, discipline and inconsistency between parents [1]. For each of the items, parents report whether or not the issue has been a problem over the last 4 weeks by answering either yes or no. This generates a score on the Problem Scale, which indicates the number of areas in which the parents are experiencing conflict. The Problem Scale ranges from 0 to 16, with a clinical cut-off of 5 (based on 1 SD above the non-clinical mean reported by Dadds and Powell). Dadds and Powell reported the Problem Scale to have adequate internal consistency (α=0.70) and high test–retest reliability (r=0.90) [1]. The internal consistency for the current sample was high (α=0.85).
For each issue that parents identify as problematic they are also asked to rate the extent to which each issue has caused difficulty. Extent is measured on a 7-point scale ranging from 1=not at all to 7=very much, with scores on the Extent Scale ranging from 16 to 112. In the present sample the Extent Scale displayed high internal consistency (α=0.94). The PPC also has concurrent validity with the DAS [27].
Child behaviour
Child behaviour was assessed using the Strengths and Difficulties Questionnaire (SDQ), a screening measure that is used to identify children's emotional and behavioural problems over the previous 6 months [28]. The measure consists of 25 items that address five factors: hyperactivity, conduct problems, emotional symptoms, prosocial behaviour, and peer problems, and five items that assess the impact of the problems on various aspects of the child's life. Each of the five subscales is measured by five items, and responses are measured using a 3-point scale. Parents respond according to how correct they feel each statement is for their child and options are 0=not true, 1=somewhat true, and 2=certainly true. The scale includes some reverse-scored items. A total difficulties score is produced by summing all of the deficit scores together excluding prosocial behaviour, giving a total score ranging from 0 to 40. A total impact score is generated by the scores on the five impact questions, all of which are measured on a 4-point scale.
The SDQ has been shown to reliably discriminate between clinical and non-clinical children, and the cut-off for the normal range is 13 out of 40. Scores of 14–16 are borderline and a score of ≥17 indicates clinically elevated difficulty. The SDQ has well-established reliability and validity, and Australian data show moderate to good internal consistency for each subscale (ranging from α=0.67 to α=0.80) and total difficulties scores (α=0.73) [29]. The SDQ has also been found to have good external validity [30]. The scale displayed moderate internal consistency in the present sample (α=0.69).
Procedure
Parents were recruited for the study through advertisements in their children's school newsletters. Australian schools with a publicly available email address were contacted and asked to include a notice of the study in the school newsletter. An email to the school contained a brief outline of the study and a draft notice that could be used in the school newsletter, containing the website address where an online version of the study was available along with contact details if additional information was required.
The website contained information that advised the parents of the study's aim and advised parents of the voluntary and confidential nature of their participation. Following the initial page was an online consent form that parents were asked to complete before being able to proceed to the questionnaires. Parents then completed the questionnaires along with a family background questionnaire that asked demographic questions about age, gender, family structure and status, educational attainment, employment status and income. Once the questionnaires were completed, parents were asked to click the submit icon and the information was then stored.
A small number of participants requested hard copies of the questionnaires. These hard copies contained the same cover letter and consent form found on the website as well as paper-and-pen versions of all the measures and family background questionnaire. Once these were completed, parents posted the questionnaires in the reply-paid envelopes provided. Information from completed surveys was keyed into the website.
Results
Preliminary analyses resulted in the removal of 18 cases from the analyses, giving a final n=200 (in eight cases there was >25% of items missing and 10 subjects had responded that they were either in a single-parent family, were divorced or widowed). A small number of respondents had values missing for some variables, but missing values analysis showed no systematic pattern among responses. Replacement of values with the item means did not change the substantive interpretation of the results. For ease of comparison and interpretation the dataset used in the following analyses contained missing values replaced with the mean scores for each item in the questionnaire. No outliers were detected in the data set. All analyses were conducted using SPSS for Windows Version 14.0 (SPSS, Chicago, IL, USA).
Validity of the Parent Problem Checklist
To inspect the validity of the PPC, correlations of the Problem and Extent scales with other measures were examined, as shown in Table 1. High scores on the PPC were associated with reports of more child problems, higher levels of general conflict, and lower marital satisfaction. In order to check whether these results were consistent across the wide age range of the study, the correlation were examined for children aged ≤9, and ≥10, and overall the same pattern was evident. In subsequent analyses only data for the full range of child ages are reported.
Correlation between key outcome variables
DAS-CS, Dyadic Adjustment Scale–Consensus subscale; PPC, Parent Problem Checklist; RQI, Relationship Quality Index; SDQ, Strengths and Difficulties Questionnaire.∗p<0.05, ∗∗p<0.01.
A χ2 test was performed to examine the association between levels of parent conflict and levels of marital dissatisfaction. Scores on the PPC Problem Scale and the RQI were categorized as clinical or non-clinical based on published cut-offs (≥5 and ≤29, respectively). As seen in Table 2, for parents within the clinical range on the Problem Scale the majority also scored in the clinical range for the RQI (χ2(176)=17.71, p<0.001). For parents in the non-clinical range on the Problem Scale, however, there were similar numbers of parents reporting in the non-clinical and clinical ranges for the RQI. Additionally, only a small proportion of parents reported in the non-clinical range for the Problem Scale but in the clinical range for the RQI. These frequencies were significantly different from those expected if the two constructs were unrelated, but does highlight that there is not a perfect association between marital satisfaction and parenting conflict.
Relationship between RQI and the PPC Problem Scales
PPC Problem, Parenting Problem Checklist–Problem subscale; RQI, Relationship Quality Index.
Clinical cut-offs for the PPC Problem Scale
Findings from previous studies suggest a score of 5 as the clinical cut-off on the Problem Scale [1, 31]. The average number of areas that parents reported as problematic was 5.66 for the current sample. This suggests that the average number of problem areas for the sample is in the clinical range. One-way analysis of variance (ANOVA) showed that parents who reported in the clinical range for the Problem Scale also reported higher levels of child difficulty, SDQ total (mean=19.48, SD=5.49), than parents in the non-clinical range (mean=16.78, SD=5.32; F(1,186)=11.77, p<.001). Similarly, parents who scored in the clinical range for the Problem Scale also reported significantly more problems in emotional sensitivity, conduct problems, and hyperactivity, and prosocial behaviour, but not peer problems, as shown in Table 3. These results indicate that the PPC Problem Scale can discriminate between clinical and non-clinical child problems using the SDQ.
Scores on the SDQ vs clinical and non-clinical parents on the PPC Problem Scale
PPC Problem, Parenting Problem Checklist–Problem subscale; SDQ, Strengths and Difficulties Questionnaire.
Clinical cut-offs for the PPC Extent Scale
A one-way ANOVA was conducted to determine if there were differences in the intensity of problems as measured on the Extent Scale between parents who reported in the clinical range for the Problem Scale compared to parents in the normal range. There was a significant difference between the two groups (F(1,46)=40.06, p<0.001), with parents in the non-clinical range for the Problem Scale (mean=22.53, SD=5.31) indicating lower intensity of conflict than parents in the clinical range (mean=56.10, SD=22.64). Stallman et al. have suggested that a score ≥2 SD above the non-clinical group mean on the Extent Scale may be a useful clinical cut-off (≥30) [31]. The present results indicate that a score of ≥30 would be effective at differentiating between clinically elevated scores and those in the normal range.
Factor structure of the PPC
Principal factor extraction was performed on the 16 items of the PPC Problem Scale using the complete dataset. It was not possible to perform factor analysis on the Extent Score due to the large amount of missing data for this scale. Principal components extraction was used to estimate number of factors, presence of outliers, absence of multicollinearity and factorability of the correlation matrices. Inspection of the correlation matrix indicated that there were many coefficients of ≥0.3. The Kaiser–Meyer–Olkin value was 0.87, exceeding the recommended value of 0.6, and the Barlett's test of specificity reached statistical significance, supporting the factorability of the correlation matrix.
Examination of the scree plot and eigenvalues suggested evidence to retain three factors. Communality values were strong, with 14 of the 16 items exceeding 0.4. When items loaded onto two factors, the largest factor loading was used to determine placement. The three factors extracted accounted for 47.2% of the variance. Seven of the 16 variables loaded on the first factor, which accounted for 31.26% of the variance, and a further four variables loaded on the second factor, which accounted for 9.01% of the variance; the third factor accounted for 6.95% of the variance. The pattern matrix and communalities are shown in Table 4. For ease of interpretation the variables are ordered and grouped in size of loading on factors. It appears that the first factor is related to disagreements over discipline (mean=3.08, SD=2.15), while the second factor is related to disagreements over child care (mean=0.82, SD=1.17). The third factor appears to describe broader family processes, such as more general family conflict and disagreement (mean=1.82, SD=1.54). Correlations between the three factors, as well as between SDQ and the three factors, are reported in Table 5.
Factor loadings (pattern matrix) and communalities (h2) for the three-factor solution with oblimin rotation for PPC Problem variables
PPC Problem, Parenting Problem Checklist–Problem subscale.
Correlation between the three factors and child behaviour
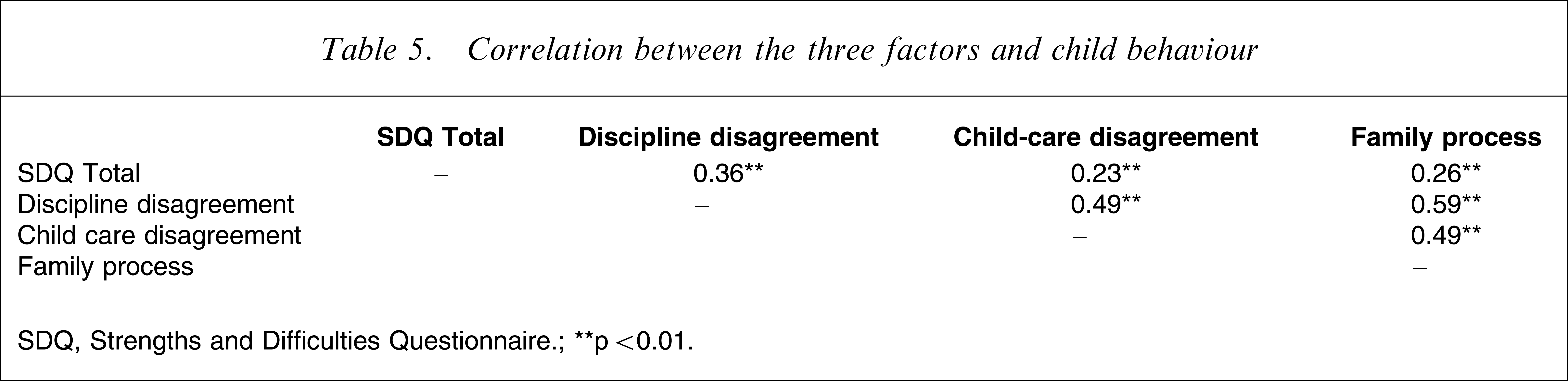
SDQ, Strengths and Difficulties Questionnaire.
∗∗p<0.01.
Prediction of child difficulty
Scores on the PPC Extent and Problem Scales showed evidence of multicollinearity (r=0.93). The PPC Extent Scale was used in the following regression analysis due to its higher correlation with child behaviour (Table 1). A hierarchical multiple regression was performed to test the hypothesis that scores on the PPC would be better predictors of child difficulty than either the RQI or the DAS-CS over and above the effects of the child's age, the child's gender, educational attainment of the respondent, family structure and family income. No multivariate outliers were found. Child age, child gender, family structure, family income and respondents’ education level were entered at the first step and the relationship scales were entered at the second step.
At step 1 there was no significant association between child age, child gender, education, family structure or family income and scores on the SDQ, with the predictors accounting for 12% of the variance in child behaviour (R=0.34, R2=0.12, F(5,47)=1.10, p=0.37). At step 2 the three relationship scales added significantly to the explained variance (R=0.70, R2 change=0.39, F(8,39)=4.71, p<0.001). Together the variables accounted for 49% of the variability in SDQ scores. Examination of the coefficients table showed that only two variables made a significant contribution to the prediction of SDQ scores. As shown in Table 6, the PPC Extent Scale was the most important variable, accounting for 35% of the variance in SDQ scores, with the DAS-CS accounting for a further 7.7% of the variance in SDQ scores. These results suggest that parent conflict assessed via the PPC is the most predictive of the measured marital factors in predicting child difficulty.
Hierarchical regression of demographic, marital and child variables on child difficulty scores
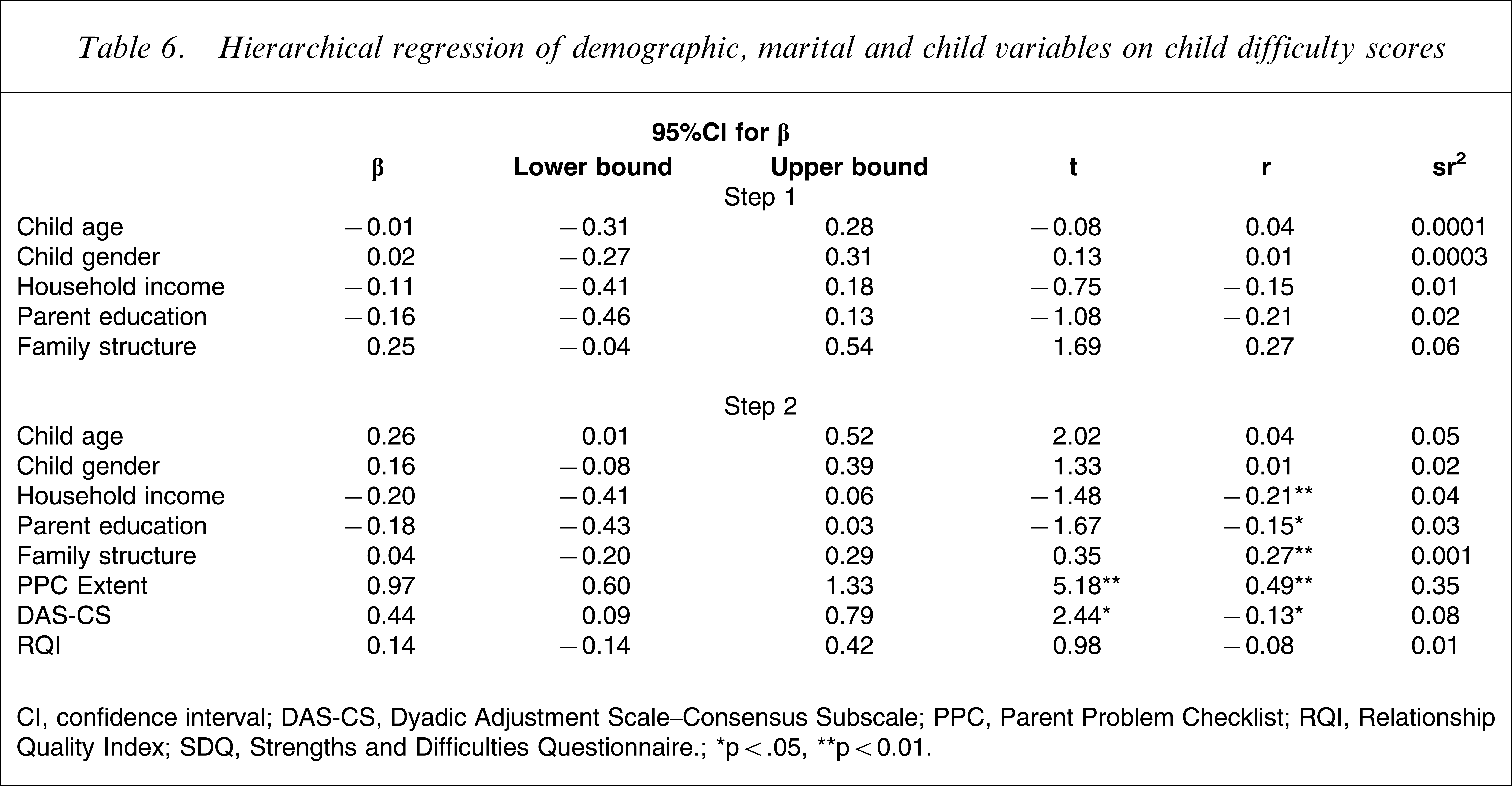
CI, confidence interval; DAS-CS, Dyadic Adjustment Scale–Consensus Subscale; PPC, Parent Problem Checklist; RQI, Relationship Quality Index; SDQ, Strengths and Difficulties Questionnaire.
∗p<.05, ∗∗p<0.01.
Discussion
The aims of the present study were to investigate the psychometric properties of the PPC [1] including validity, and to examine the factor structure of the measure. The present results indicate that parenting conflict as assessed using the PPC was related to observations of child difficulty in the sample, and explained more of the explained variance in child difficulty scores than either marital conflict or marital satisfaction. Furthermore, the results suggest that the PPC displays excellent levels of reliability and validity and can distinguish between clinically elevated levels of problems relating to parenting. The results of this study provide tentative support for three underlying factors for the measure of parenting conflict: discipline disagreement, child-care disagreement and family processes.
Validity of the Parent Problem Checklist
Given the well-established reliability and validity of the RQI and DAS-CS, the high correlations between the PPC Problem and Extent Scales and both the aforementioned measures are evidence for the concurrent validity of the PPC. Additionally, predictive validity is evidenced by the ability of the scores on the PPC to vary between clinical and non-clinical scores on the RQI and the SDQ. Both scales of the PPC also displayed excellent reliability in the present study.
Parenting conflict and relationship dissatisfaction were also found to be related. For the present sample, parents were unlikely to experience clinically elevated levels of parenting conflict without experiencing clinical levels of relationship dissatisfaction. Parents in the normal range on the PPC, however, reported no differences in the numbers of clinical compared to non-clinical levels of marital satisfaction. One-third of parents were classified in the clinical range for only one measure, indicating that these two factors of marital functioning are not perfectly associated. This suggests that although parenting conflict increases the likelihood of also experiencing marital dissatisfaction, it is not a necessary component. Not all discontented relationships are characterized by parenting conflict, hence there is a need to assess the more specific factor of parenting conflict over and above relationship satisfaction as it relates to children.
Previous research has suggested that child difficulty is more strongly associated with specific measures of child-rearing problems than measures of marital conflict or satisfaction, thus it was predicted that parenting conflict as assessed using the PPC would be a better predictor of child difficulty than either marital satisfaction or marital conflict [1, 15]. In accordance with previous research, the present results indicate that parenting conflict was more strongly correlated with child difficulty than either general marital conflict or marital satisfaction.
It is noteworthy that no significant relationship was found between parents’ reports of child difficulty and scores of marital satisfaction, and there was only a weak correlation found between general marital conflict and child difficulty. These results are in line with previous research that suggests that these global measures of marital functioning are lacking in specificity, and cannot adequately capture the relationship between the specific components of marital functioning that affect children [7, 9, 15]. It was predicted that all the relationship measures would correlate with reported child difficulty but that conflict over child-rearing would account for more of the variance in child difficulty scores than either marital satisfaction or conflict. This hypothesis was supported because parenting conflict was the most significant correlate of child difficulty scores and was the best predictor of child emotional and behavioural problems in the present sample. Furthermore, it was found that as specificity of the measures increased so did the observed relationship: parent conflict was more significantly associated with child problems than either of the other measures, followed by marital conflict, which was weakly associated. and finally relationship satisfaction, which did not significantly correlate with child difficulty. Family demographic variables did not contribute to the prediction of child problems. Overall, these results suggest that parent conflict is the best predictor of the measured factors in predicting child difficulty for the current sample.
Parents who reported clinically elevated levels of parenting conflict also reported that their child displayed significantly more problem behaviours in the areas of emotional sensitivity, conduct problems and hyperactivity, and overall child difficulty. They also reported that their children displayed significantly less prosocial behaviours than parents who reported in the normal range on the PPC Problem Scale. There was no difference between the two groups for peer problems, possibly as a result of the low reports of peer difficulties in this sample. In sum, these findings provide further evidence of the association between parenting conflict and child behaviour difficulties, and highlight the usefulness of the PPC to measure interparental conflict as it relates to child behavioural outcomes.
Overall, the PPC appears to be a valid and reliable measure for assessing interparental conflict and thus would be a useful tool in clinical practice. The PPC could be used by clinicians to inform them about aspects of family functioning and guide the development and tailoring of effective interventions aimed at assisting parents in their roles and enabling them to effectively address the problems that their children are displaying.
Factor structure of the Parent Problem Checklist
Results from the present study support a preliminary three-factor solution for the PPC Problem Scale. Dadds and Powell suggested that the measure may have three factors, but they reported that their factor analyses indicated a unidimensional structure [1]. The authors did not report on any aspect of their factor analysis, making it difficult to interpret the nature of their finding. From the current study it appears that the PPC consists of three factors assessing separate aspects of parenting conflict. The Child-Care Disagreement factor reflects conflict corresponding to how child-care responsibilities should be shared between parents, and the Discipline Disagreement factor reflects conflict according to how parents manage discipline such as disagreement over which behaviours are problematic and how their children should be reprimanded for misbehaviour. Finally, the Family Process factor appears to capture broader aspects of the conflict such as fighting in front of children, and parents undermining each other. The inconsistency between the present study and the Dadds and Powell study may reflect the dichotomous nature of measurement of the PPC Problem scale. Analysis of dichotomous (cf. continuous) scales has several limitations, including loss of information about individual differences, and loss of effect size and power, as well as the potential for spurious factors during factor analysis of binary items [32]. Future research examining the PPC should attempt to confirm these factors, and to conduct factor analyses on the Extent scale. Factoring of the Extent scale was not possible in the present study due to the low response rates for this scale, as discussed in the following section.
Limitations and future recommendations
The present study had a number of limitations that need to be considered when interpreting the results. First, the study used a small sample and there was an unequal representation of mothers compared to fathers. Jenkins and Smith found that fathers reported fewer marital problems and fewer child difficulties than mothers in their sample, suggesting that fathers’ perceptions may differ significantly from those of mothers [9]. Therefore, it would be important for future research to assess fathers’ perceptions of parenting and marital problems and directly compare their responses to those of mothers, because it could not be determined from the present study if fathers considered the same parenting or marital issues as problematic or as intense as mothers did.
The parents in the present sample, on average, reported in the clinical range for parenting conflict, marital dissatisfaction and child problems. This suggests that there may be something about the type of families who responded to the present study that may not be reflective of the general population and therefore limits the generalizability of the findings. It is possible that these families were already experiencing marital and child difficulties, which is why the present study drew their attention and influenced them to participate.
Furthermore, there seemed to be confusion in the sample as to how to respond to the PPC Extent Scale. Participants were asked to answer yes or no to indicate whether each issue was a problem for them, and if they answered yes to indicate the intensity of the problem by a score on the Extent Scale. Despite these instructions, numerous parents stated that the issue was not a problem but still reported an extent score, which suggested that the issue was somewhat of a problem. Therefore, it is recommended that parents be instructed to respond to both scales in the measure for each item. The PPC Extent Scale is currently measured on a scale of ‘not at all’ to ‘very much’. This range allows room for parents who do not perceive the issue as a problem to indicate as such. A complete set of responses on this scale will also enable factor analyses to be conducted.
A limitation common to most research on the relationship between marital conflict and adjustment problems in children, is the use of correlational methodology, which prevents any conclusion of causality. It is likely that the relationship between parent functioning and child outcomes is bi-directional, in that parent conflict influences child difficulty but that difficult child behaviour places stress on the interparent relationship and impacts on marital functioning. Future research would benefit from conducting longitudinal studies that can assess the impact of parent conflict in the long term, using multi-observer assessments.
The current study, as well as the original report of the PPC [1], have used samples that predominantly identified with the white ethnic group, so it is not known if these findings are generalizable to other ethnic groups or cultures. Future research should aim to assess the efficacy of the PPC in a more diverse sample of parents to be able to determine if the effects of parent conflict or even the perceptions of what is problematic are cross-cultural. Moreover, it may prove useful for future research to compare which of the factors of the PPC correlate with different types of behaviour problems within clinical samples. It may be beneficial to determine if either the Child-Care Disagreement or Discipline Disagreement factors are more significantly associated with different behaviour problems. Additionally, this knowledge may serve to highlight areas that are likely to be problematic for presenting families, given their responses to the PPC, and could guide clinicians in their assessments and development of interventions.
Conclusions
The present research highlights the relationship between parenting conflict and negative child outcomes, and demonstrates the usefulness to clinical practice of the PPC. The PPC was found to provide a valid and reliable measure of parent conflict specific to child rearing issues and was a better predictor of child difficulty than either measures of marital satisfaction or general marital conflict. The present findings should not be used to suggest that marital conflict and marital satisfaction are inconsequential to the development of child adjustment problems; rather that parent conflict may have a more proximal influence on problem child behaviour. The present study has highlighted the clinical utility in measuring parenting conflict using the PPC as a tool to identify areas that may be problematic for families, and can thus guide the development of interventions that can be of benefit to the whole family.