
Abstract
Post-traumatic stress disorder (PTSD) is a common sequel of combat, with rates among troops returning from current conflicts in the Middle East estimated to be between 6%%and 13% [1]. Unfortunately, particularly in its chronic form, the disorder has proven difficult to treat [2], [3], creating a challenge for the design of psychiatric services targeted at past and present members of the defence force. Nevertheless, progress has been made in the last decade, with more recent outcome data providing grounds for cautious optimism [4]. In many countries, including the USA, Canada, and Australia, government-funded treatment programmes for veterans have generally been programmatic in nature, with cohorts of veterans progressing together through a relatively standard programme of treatment over a pre-defined period of time.
Since 1995 the Australian Department of Veterans’ Affairs (DVA) has funded programmatic PTSD treatment for veterans, predominantly those from the Vietnam conflict. The initial programmes, established in the mid 1990s, were 12 weeks in duration, consisting of a 4 week inpatient phase followed by 1 day per week outpatient treatment for 8 weeks. Data from those initial programmes were encouraging, with moderate to large treatment effects in PTSD symptomatology and small to moderate improvements in symptoms of anxiety and depression [4]. The question then arose as to whether the initial phase of these programmes could be conducted on a day hospital rather than inpatient basis, providing a more normal environment for recovery, easier access, and a potential cost reduction. Despite initial concerns from clinical staff regarding the capacity of non-inpatient programmes to contain and treat veteran populations, early data indicated no differences in symptom profile or outcome between the inpatient and day hospital programmes [5].
During the past 8 years a wider variety of programmes has been introduced. These alternatives, while consistent with each other in terms of content, have differed across parameters of programme structure and clinical setting. In part, these variations were designed to improve accessibility for veterans living in rural areas, often a considerable distance from metropolitan facilities. These new programme types vary in terms of the number of treatment days per week, as well as in location (metropolitan centres or regional outreach). The goal is to provide a range of programme types to meet the needs of a heterogeneous veteran population with chronic combat-related PTSD and to minimize familial, social and vocational disruption associated with programme attendance.
There are now sufficient data to allow an observational research design to examine the relative effectiveness of these different programme types. Specifically, the aim of the present study was to examine whether: (i) there are differences in initial PTSD and comorbidity profiles across programme types; and (ii) there are differential outcomes as a function of programme intensity. The findings may inform planning of psychiatric services for younger veterans returning from recent military operations, for whom flexible, innovative treatment structures and settings are likely to be required.
Method
Participants
Participants consisted of 4339 male veterans with a PTSD diagnosis who were consecutive admissions to accredited PTSD treatment programmes between 1995 and March 2008. PTSD diagnoses were based on structured interview using the Clinician-Administered PTSD Scale (CAPS) [6]. The mean baseline CAPS severity score was 81.65 (SD = 17.97). Comorbidity in the sample (as rated by the assessing clinician using a non-structured psychiatric clinical interview) was common, including substance abuse/dependence (36%), depression (39%), and another anxiety disorder (11%). These rates are consistent with those reported in US samples of treatment-seeking combat veterans with PTSD [7].
Approximately 80% had served in the army, 15% in the navy and the remaining 3% in the air force. Mean age at programme entry was 54.40 (SD = 8.86) years. The majority (74%) were married or in a de facto relationship. Almost all (93%) of the sample was in receipt of a DVA pension. Written informed consent to complete evaluation forms was obtained.
Decisions regarding which programme model each veteran would undertake were based on several factors, including availability and accessibility. Service providers vary in the range of programme types they offer; large facilities run several models while smaller providers often conduct only a single programme type. Options for veterans, therefore, depend on the programme types available in their State. Where more than one programme type was available, the decision was based on a combination of clinician judgment and veteran preference.
Treatment
At the time of the present study five programme types were available with varying levels of intensity (days of treatment per week) and setting.
High-intensity inpatient–outpatient programmes
These programmes were conducted in hospital settings with an intensive inpatient phase of 3–4 weeks followed by an outpatient phase of approximately 8 weeks at 1 day per week (n = 1680).
High-intensity residential programmes
These programmes have the same structure as inpatient programmes, but participants return home each day during the intensive phase; those who live some distance from the hospital were housed in residential accommodation, rather than a hospital ward, for the intensive phase (n = 422).
Moderate-intensity day hospital programmes
These programmes were conducted on an outpatient basis at a metropolitan hospital with an intensive phase of at least 2–3 days per week for 4–6 weeks followed by a less intensive phase for the remaining weeks (n = 1697).
Moderate-intensity regional day hospital programmes
These programmes had the same structure as the day hospital programmes, but were conducted solely in a regional centre close to where the participating veterans lived (n = 267). In these programmes the treatment team from the metropolitan facility would travel to the designated regional area and deliver the programme from a local facility.
Low-intensity programmes
This programme type was conducted on a once-weekly basis over approximately 6 months (n = 273).
The treatment programmes were primarily cognitive behavioural in orientation and conducted by mental health professionals with closed cohorts of between six and 10 participants. The treatments were consistent with the specifications outlined in the Australian Centre for Posttraumatic Mental Health (ACPMH) guidelines. Although all programmes were consistent with these guidelines, there was some variation across services in the manner in which the guidelines were applied. Although these manuals remain the property of the individual services, the accreditation guidelines upon which they were based are available from the ACPMH website (www.acpmh.unimelb.edu.au). Key components included psychoeducation, symptom management skills (with a particular focus on arousal and anger), trauma focus work, cognitive restructuring, alcohol management and problem solving. Between eight and 16 sessions of individual therapy were also provided to participants over the course of programmes. More information on treatment programmes is provided elsewhere [4]; importantly, the content was consistent across programme types. All primary facilitators in these programmes were trained health professionals.
Measures
As part of standardized assessment, participants completed self-report questionnaires. These questionnaires included the PTSD Checklist (PCL) [8] as a measure of PTSD. The PCL has demonstrated high levels of diagnostic accuracy when evaluated against gold standard structured interview measures such as the PTSD component of the Structured Clinical Interview for DSM-IV [9] and the CAPS, both at a single time point and over the course of treatment and follow up [10]. A score of 50 on the PCL is considered an appropriate cut-off at which to make the diagnosis of PTSD in treatment-seeking veteran samples [10]. The measure has demonstrated strong test–retest reliability (0.96) and high levels of internal consistency (0.97). The Hospital Anxiety and Depression Scale (HADS) [11] was used as a measure of anxiety and depression. The HADS is a 14-item scale, with seven items relating to anxiety and seven items relating to depression. It has strong psychometric properties, with high internal consistency (α = 0.90 for depression and 0.93 for anxiety) and a robust two-factor structure. The Alcohol Use Disorders Identification Test (AUDIT) [12] was used as a measure of alcohol use. Scores of ≥8 are considered positive for alcohol problems and the scale has demonstrated strong internal reliability (0.86). All questionnaires were completed on three occasions: at admission, as well as at 6 and 12 months after intake.
Data analyses
Analyses of the data included preliminary descriptive statistics examining major outcome measures across each of three time points: baseline, 3 months after discharge and 9 months after discharge for each location×intensity programme combination. Analysis of variance (ANOVA) was used to test for statistical differences.
Analyses combined the two high-intensity metropolitan programmes of inpatient and residential because the structures of these programmes were highly similar. Repeated measures analysis of variance (RMANOVA) were then used to compare improvements achieved in each of the three categories of programme conducted in metropolitan and regional locations. Results are also presented as effect sizes. These analyses, including presentation as effect sizes, were then replicated with participants tertiled by CAPS severity score at intake. Finally, outcome measures were compared using RMANOVA for attendees of moderate-intensity courses conducted in metropolitan and regional locations to assess whether location of course contributed to improvement in outcomes. Data analyses were conducted using SPSS 15 (SPSS, Chicago, IL, USA).
Results
Table 1 provides means and standard errors of the four outcome measures (PCL, HADS depression and anxiety scores, and total AUDIT score) for those assessed at baseline, 3 months and 9 months after discharge from the programme. These measures are given for participants in the three types of metropolitan courses, those undertaking the moderate intensity course in regional locations and all participants combined. Effect sizes of these interventions have also been calculated. As can be seen from Table 1, mean intake scores for PCL and anxiety differed significantly for those participating in programmes of different intensities. Such differences, however, were not evident in depression or in substance use at the 12 month time point.
Programme outcome measures vs programme intensity and location
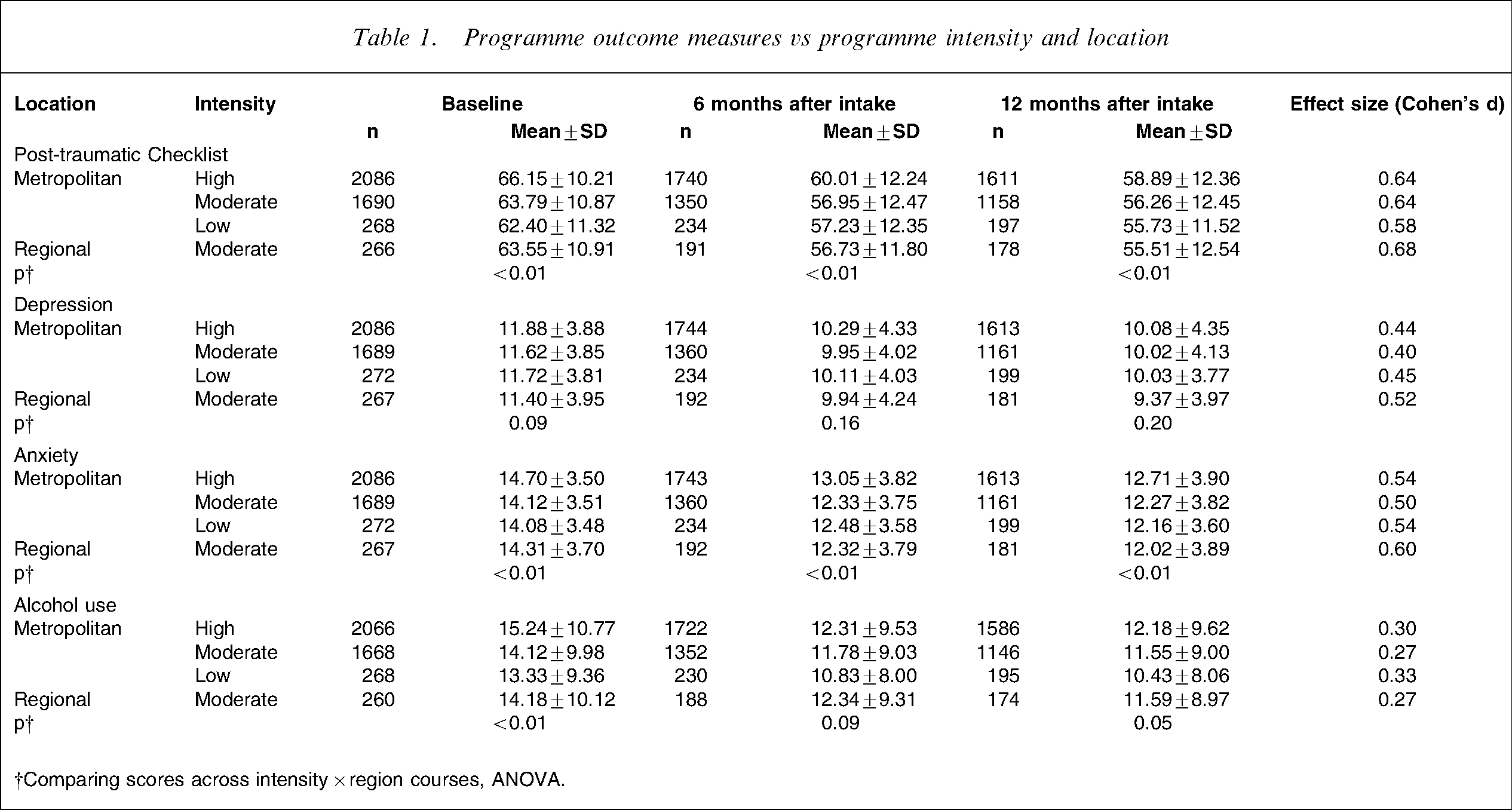
†Comparing scores across intensity×region courses, ANOVA.
Direct comparison between programme types, using the Tukey–Kramer multiple comparisons test showed that the statistically significant finding at baseline, 6 months and 12 months for PTSD was due to those participating in the high-intensity programmes. There were no statistically significant differences between any of the other programmes.
RMANOVA was then used to compare the outcome measures across the three time points (baseline, 3 months and 9 months) for the four categories of programme: high-, moderate- and low-intensity courses conducted in metropolitan areas, and moderate-intensity courses conducted in regional locations. The test of time×programme effects indicated significant improvements in all programme types over the 12 month time period with no significant differences in levels of improvement by programme type (Table 2).
RMANOVA of change in programme outcome measures
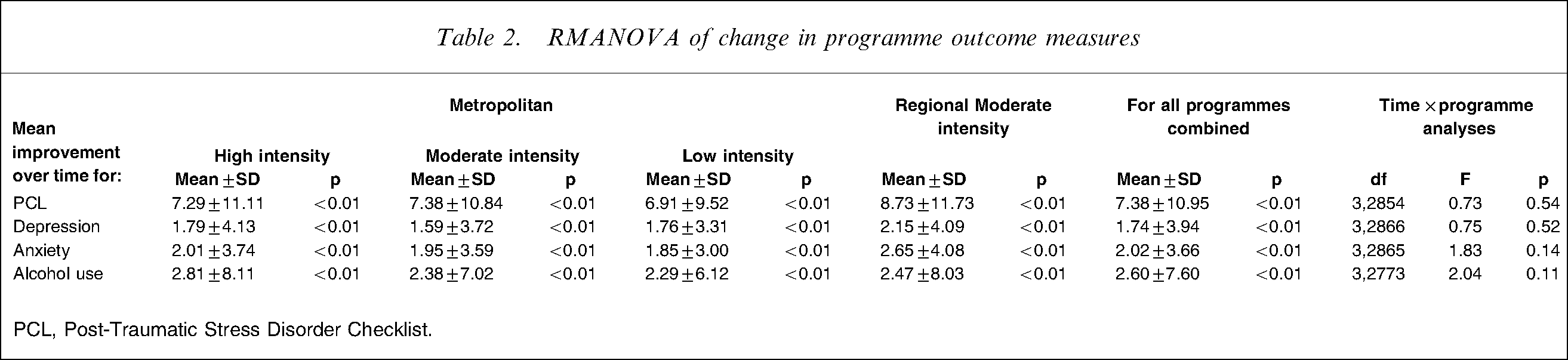
PCL, Post-Traumatic Stress Disorder Checklist.
The respondents were then tertiled into three subcategories based on the severity of their PTSD symptoms at intake. As can be seen from the results of the RMANOVA in Table 3 and effect size analyses of PCL outcomes in Table 4, veterans in the highest tertile of PTSD symptom severity reported significantly smaller improvements in depression, anxiety and alcohol use if they undertook a PTSD programme of low intensity compared to veterans in this high-severity group who undertook moderate- or high-intensity programmes. Consistent with this, veterans in this high-severity tertile group attending high- or moderate-intensity programmes reported large effect reductions in PTSD (effect size of 0.80), while veterans in this tertile who participated in low-intensity programmes reported only moderate improvements in PTSD (effect size of 0.52). Interestingly, there was also a trend for those with lowest severity PTSD at intake to improve less in high-intensity programmes compared with others with the same severity of symptoms who undertook low-intensity programmes. For those reporting the lowest tertile of PTSD symptoms, the effect size of undertaking the high-intensity intervention was 0.52 (moderate effect size), whereas for those with this level of PTSD severity who completed the low-intensity programme, the intervention achieved a large effect size (0.75).
RMANOVA of change in outcome measures vs CAPS severity score at intake
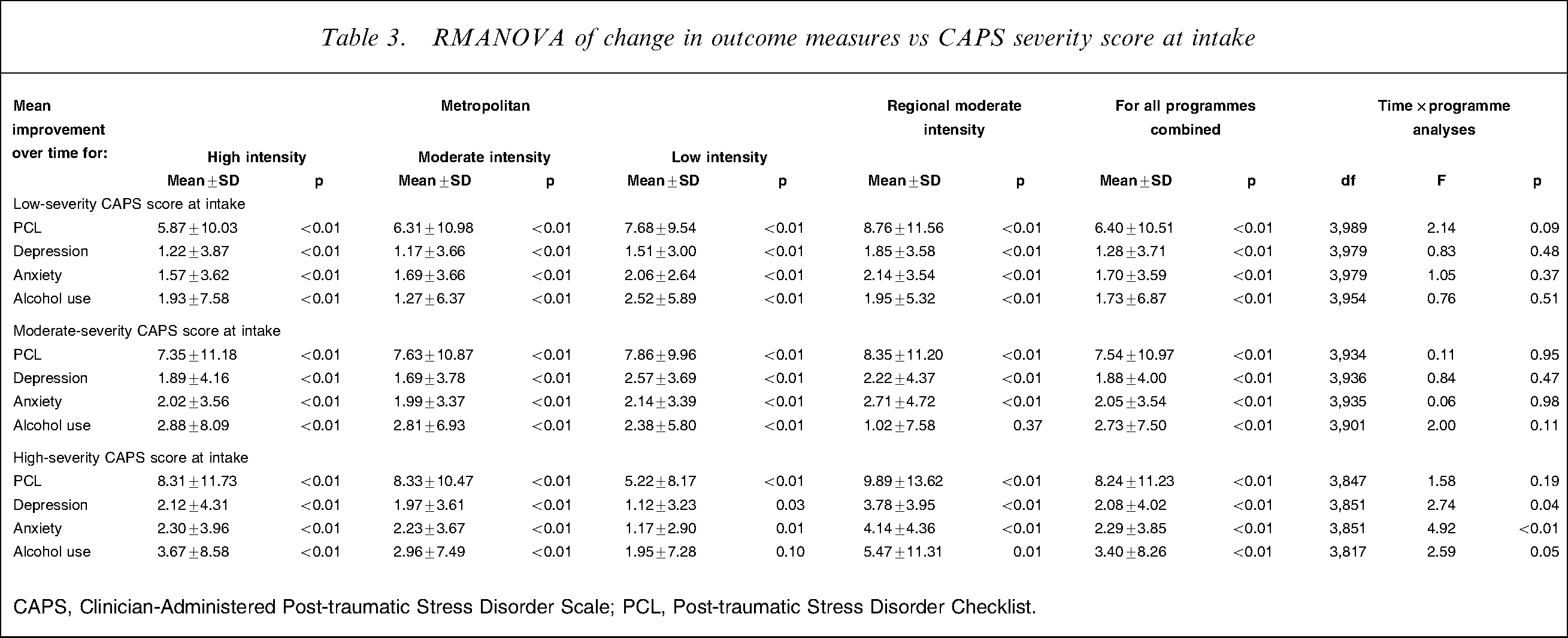
CAPS, Clinician-Administered Post-traumatic Stress Disorder Scale; PCL, Post-traumatic Stress Disorder Checklist.
Effect size analyses of PCL outcomes
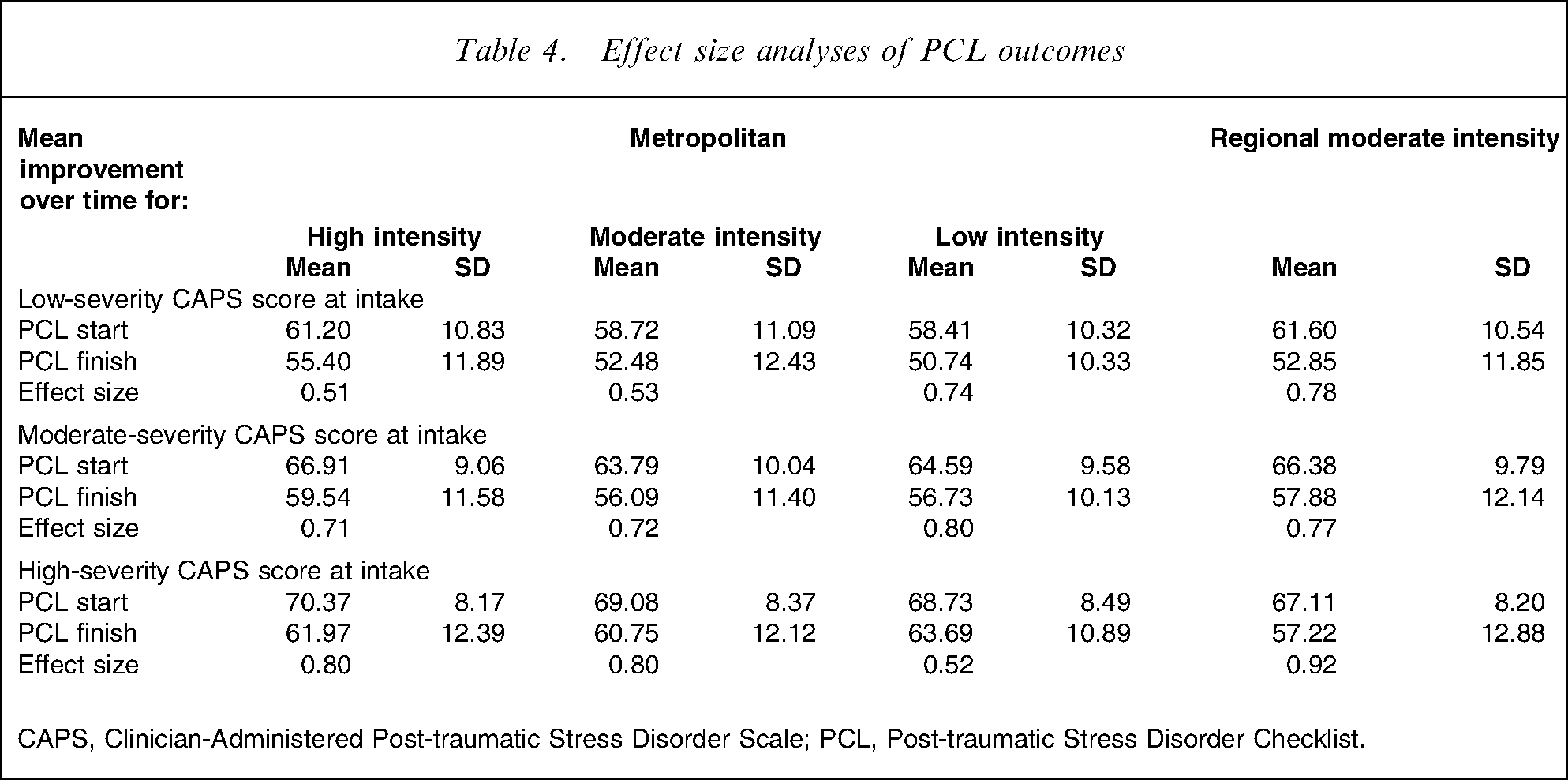
CAPS, Clinician-Administered Post-traumatic Stress Disorder Scale; PCL, Post-traumatic Stress Disorder Checklist.
Our final analysis (Table 5) compared the outcomes of the two moderate-intensity programmes conducted in metropolitan and regional locations. There were no statistically significant differences by PCL scores. Participants with high-severity PTSD reported significantly better outcomes in depression and anxiety symptoms and alcohol use if they had undertaken their moderate-intensity programme in a regional location. The finding concerning alcohol use, however, was reversed for those with moderate-severity PTSD; those in metropolitan programmes reported better outcomes in this measure.
Comparison of the two moderate-intensity programmes
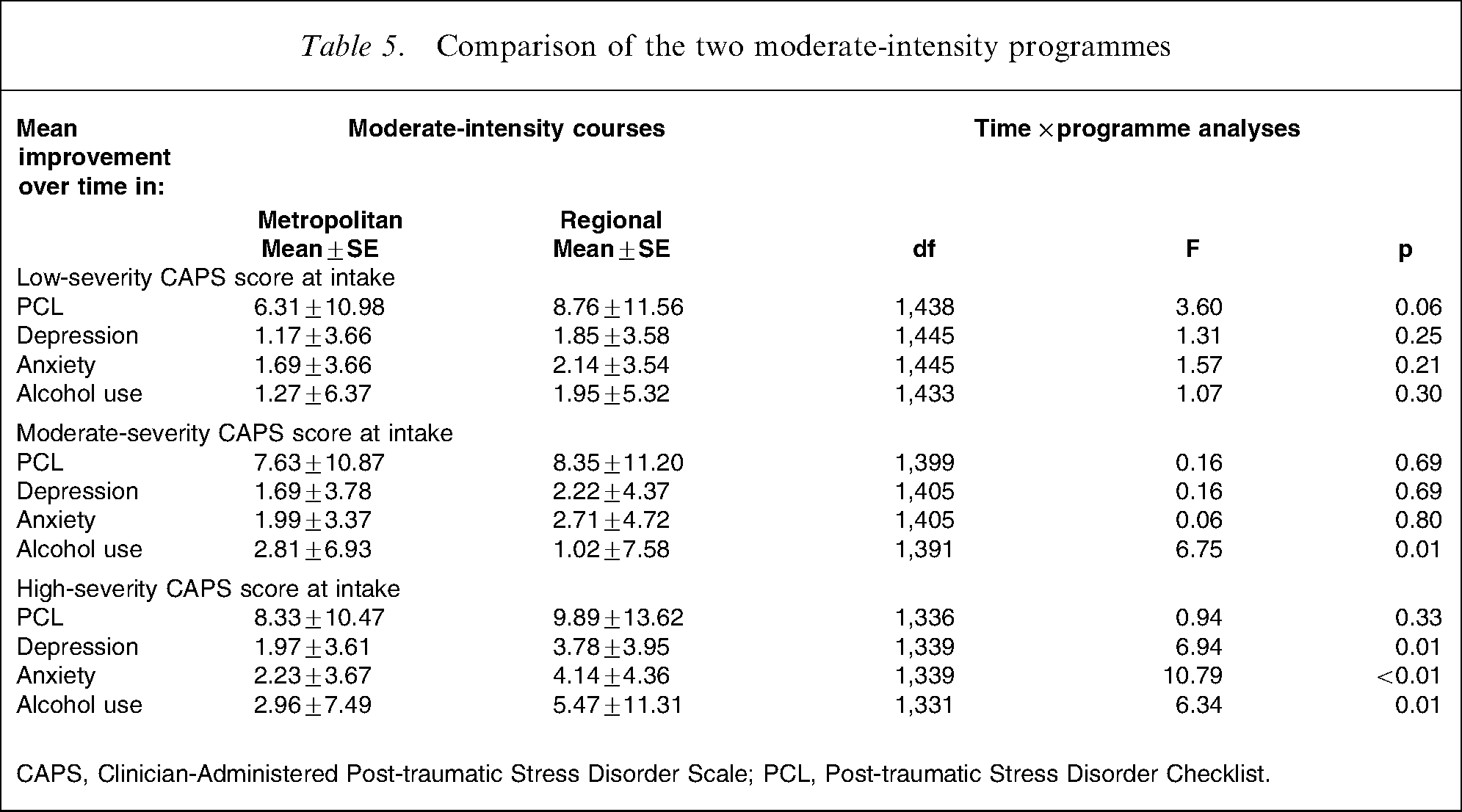
CAPS, Clinician-Administered Post-traumatic Stress Disorder Scale; PCL, Post-traumatic Stress Disorder Checklist.
Discussion
The study findings show that high-intensity programmes recorded consistently higher intake scores on PTSD, anxiety and alcohol at intake than moderate- and low-intensity programmes. Importantly, however, although these differences are consistent and statistically significant, they are unlikely to reflect differences of clinical significance. For PTSD, for example, they reflect differences of <4 points on a 75 point scale from highest to lowest intensity programme, with even smaller differences for anxiety and alcohol. Analyses failed to identify any overall differences in treatment outcome between the different intensities of programme type for PTSD or its comorbidities. Interestingly, however, when the severity of PTSD was considered, a number of trends became evident. First, the data supported by effect size analyses suggested that participants with low-severity or mild PTSD did poorer in the high-intensity programmes than veterans with mild PTSD who participated in low-intensity programmes. A similar finding of poorer outcomes in the context of a mismatch of PTSD severity and programme intensity type was also evident for veterans with more severe PTSD. In this case results suggested that veterans with more severe PTSD benefited most from the high- and moderate-intensity programmes rather than the low-intensity programme.
Overall, both of these findings suggest that attempts to place veterans in the programme intensity types consistent with their PTSD and comorbidity severity can maximize outcomes. This appears to be particularly the case when the low- and high-intensity programmes are considered. In terms of the moderate-intensity programmes, these programmes appeared largely beneficial across the severity range.
A further comparison of interest was the difference in outcome between the two moderate-intensity programmes, delivered in either a metropolitan or regional outreach setting. For veterans with more severe PTSD, the data suggest that outcomes for comorbidity are improved when veterans from regional areas complete the moderate-intensity programme locally. Similarly, for veterans with mild PTSD, locally delivered regional programmes appear to demonstrate a trend toward greater improvement in PTSD symptoms than those delivered in metropolitan facilities, although no differences in comorbidity outcomes were evident.
Interestingly for veterans with moderate-severity PTSD, metropolitan programmes demonstrated stronger outcomes in alcohol misuse specifically than the regionally delivered programme. It is important to note that because veterans participating in metropolitan-based moderate-intensity programmes may be either local to the metropolitan areas or commuting from regional areas, it is difficult to make more confident assertions about the respective benefits of these programmes. The data do suggest, however, that delivering a moderate-intensity programme on an outreach basis to veterans in regional areas does not appear to detract from potential outcomes, and may in some ways enhance these outcomes. Such an approach also has good clinical validity, allowing regionally residing programme participants to practise skills in their normal environment, minimizing disruption to existing functional routines and optimizing opportunities for maintenance of naturally occurring support networks during treatment.
The difficulty, of course, is often one of providing an appropriate treatment team in a rural location, particularly when the distances involved may be very large. For the programmes described in this paper, clinicians travel from the metropolitan facility to the rural location, often for several days at a time. Such a model places considerable demands on clinicians. Regionally based outreach programmes, however, also aim to engage local clinicians in the treatment programme. Where this occurs, it potentially offers a service development opportunity to up-skill local clinical services and facilitate engagement of the veteran with local providers for post-programme support.
The present study has implications for the planning and implementation of service models for veterans with combat-related PTSD. To maximize outcomes it is suggested that a range of programme intensity models be offered with attempts to, as best as possible, place veterans in programmes that match the programme intensity with PTSD severity. Where the development or purchasing of such a range of models is not feasible, the moderate-intensity programmes appear to offer comparable benefit to veterans of varying PTSD severities and may offer the most parsimonious model. Importantly, solid gains are evident from the moderate-intensity programmes when delivered either in metropolitan facilities or on a regional outreach basis. Indeed, the advantage of regionally delivered programmes for regional veterans may be enhancing access and minimizing disruption to routine functioning and local and natural support networks.
Interpretation of the current findings should be tempered with caution. First, stabilization of key comorbid conditions such as alcohol misuse and depression were required criteria for admission to the programmes. Facilities often provided extensive clinical care to the veteran prior to the PTSD programme. Therefore, absence of difference in clinical presentation at programme commencement across moderate- and high-intensity programmes may be a function of adequate stabilization by the high-intensity programmes prior to PTSD programme commencement.
Second, the veterans included in the present study suffered PTSD of, in many cases, 25 years chronicity. Outcomes of the programme types may differ in the case of more acute presentations. Third, there were smaller numbers of veterans in some of the programme types, which may affect the significance of possible differences. Finally, in view of the naturalistic design of the present study, the findings require confirmation using a randomized controlled design and methodology.
Conclusion
This study indicates that comparable outcomes were evident across variations in PTSD programme intensity type. There was some suggestion that outcomes may be maximized when veterans are placed in programme intensity types that match their level of PTSD and comorbidity severity. When such matching is not feasible, moderate-intensity programmes appear to offer the most consistent outcomes. The data also suggest that, for regionally based veterans, delivering treatment in their local environment does not detract from, and may even enhance, outcomes. These findings, although requiring replication, have substantial implications for the planning and purchasing of mental health services for sufferers of PTSD, particularly for veterans of more recent combat or peacekeeping deployments.
Footnotes
Acknowledgements
The authors would like to thank veterans and staff from PTSD programmes across Australia for their participation in programme evaluations, without which this study would not have been possible. The authors would also like to thank Dirk Biddle and Dr Peter Elliott for their contributions to earlier versions of this paper. Ethics approval for the collection of evaluation data from programme participants was provided by the Department of Veterans’ Affairs Human Research and Ethics Committee.