
Abstract
Delusion is one of the defining symptoms of psychotic disorders. In a World Health Organization prospective study of individuals with signs of schizophrenia in 10 countries, delusions of reference and persecutory delusions were the two most common symptoms [1]. In the last 10 years cognitive psychological models have been introduced to try to explain the formation and maintenance of delusions [2–6]. These models highlight both reasoning biases and emotional processes.
Reasoning: Jumping to conclusions
Garety et al. and Huq et al. originally demonstrated that, on a typical probabilistic reasoning task (the beads task), people with delusions have been shown to jump to conclusions, requesting less information to reach a decision than controls [7], [8]. In one (easy) version of the beads task, participants are presented with two jars that each contains 100 beads [7]. There are 85 beads of one colour (e.g. black) and 15 beads of another (e.g. orange) in one jar, and, in the other jar, 15 black and 85 orange beads. After the jars have been removed from view, beads are drawn, upon request from the participant, from just one of the jars in a predetermined order. Participants are asked to decide from which jar the beads are drawn. Using this task, previous studies have found that delusional and delusion-prone participants request fewer draws of beads before reaching a decision about the source of the beads [9].
Freeman recently reviewed 10 studies comparing individuals with delusions and non-clinical controls [10]. In all these studies data gathering was hastier in the delusional group, and the majority of the delusional individuals showed the jumping to conclusions (JTC) cognitive bias (which has been defined by participants reaching a decision after two or fewer beads [11]). These studies have all been conducted in Europe (mostly the UK) and North America; there have as yet been no studies of this phenomenon in other cultures. The data gathering bias is hypothesized to result in the hasty acceptance of beliefs that are supported by inadequate evidence. Garety et al. found that JTC is specifically related to levels of delusional conviction [11].
Emotional states: anxiety
Catastrophic worry and anxiety disorders are common in patients with persecutory delusions [12], [13]. It has been suggested that a cognitive component characteristic in anxiety, ‘anticipation of danger’, is reflected in the content of persecutory beliefs [14]. According to the Freeman et al. threat anticipation model of persecutory delusions [15], anxiety provides the threat theme integral to a persecutory delusion and maintains the delusion through processes such as worry and safety behaviours [16]. This idea is supported by cross-sectional studies measuring the links between affect and delusion [3], [13], [17].
JTC and anxiety have therefore been separately linked with delusions. It is plausible that the two delusion factors may interact, that is, high-anxiety states may make data-gathering even more hasty. In an earlier study Garety et al. found that patients with anxiety performed between deluded and non-clinical controls on the beads task, hence hypothesized that anxiety might increase JTC [7]. More recently, Garety et al. found that anxiety and reasoning biases (including JTC) contribute to delusional conviction independently, and emotions are not associated with reasoning processes [11]. Garety et al., however, used questionnaire measures of trait depression and anxiety and recommended that future studies should assess state anxiety [11]. In a subsequent study, Ellett et al. found that when people with persecutory delusions were randomly exposed to a mildly anxiety-provoking urban street environment or to a relaxation condition, those in the street exposure condition showed both an increase in state anxiety and higher levels of JTC compared to the relaxation control [18]. This suggested that state anxiety might increase JTC but it is possible, given the research design, that some other aspect of the study procedure (e.g. exposure to a social setting) rather than anxiety alone might have accounted for the effect on JTC.
Using an experimental manipulation procedure, the aim of the present study was therefore to investigate whether level of state anxiety has a causal relationship to the JTC reasoning bias in a group of Hong Kong Chinese patients with first-episode psychosis. The present hypotheses were as follows: (i) that the JTC reasoning bias will be replicated in a Hong Kong Chinese population of individuals with delusions; (ii) that patients with psychotic disorders will show a higher level of JTC than the non-clinical controls; and (iii) that people with increased state anxiety will show a higher JTC reasoning bias than those with decreased state anxiety.
In addition, the present study aimed to further investigate the hypothesized continuum of psychotic symptoms. As suggested by previous studies, people with psychosis and the non-clinical population share some psychotic-like experiences but differ in delusional explanation and emotional distress [19–21]. The present study measured and compared several dimensions of delusional beliefs in patients with psychosis and in non-clinical controls.
Methods
Participants
Two groups of participants were involved in the present study. The delusion group consisted of patients who were recruited from an intervention programme for people with first-episode psychosis in Hong Kong. Patients with psychosis were invited to participate in the study if they were assessed by their treating psychiatrists to have an active delusion, were aged between 15 and 30 years, and gave informed consent. Both inpatients and outpatients were recruited. Psychiatric diagnosis was determined by the patient's treating psychiatrist according to the ICD-10 criteria. Patients were excluded if their major diagnosis was drug-induced psychosis or organic brain disorders or if they had a learning disability. The control group consisted of non-clinical individuals recruited from a university, a secondary school, and a church.
Procedure
Randomization and induction
Both patients and controls were randomly allocated to one of two experimental conditions: induction of state anxiety, or reduction of state anxiety. Randomization was conducted by a research assistant who was blind to the study procedures. Randomization was stratified according to recruitment site.
Major study procedures were conducted by the same experimenter (S.H.S.). Patients were interviewed soon after they were referred by their psychiatrists to the study, hence there were variations in length of stay and duration of treatment. Inpatients were interviewed in a quiet consultation room in their wards, whereas outpatients were interviewed in the psychiatric clinic. Non-clinical controls were interviewed in a quiet room in a university, a secondary school, and a church, respectively. All interviews took place during the day and in an environment that participants were familiar with. Procedures of the study were explained to the participants before written consent was obtained.
Experimental anxiety state manipulation
In condition 1 participants were asked to recall an everyday situation in which they had been slightly anxious. They were instructed to visualize this circumstance for a period of 5 min. In condition 2, participants were similarly invited to engage in relaxation imagery for 5 min. Visual analogue scales were used before and after to check the mood manipulations. Previous studies have found mental imagery to be an effective method in temporarily manipulating state anxiety in non-clinical individuals and anxiety patients [22], [23]. The current study is the first attempt to adopt mental imagery technique for manipulating state anxiety in psychotic patients.
Experimental task
After mood states were manipulated and measured, participants in both conditions undertook a reasoning task, namely the beads task [7]. Two versions of the beads task were used in the present study. In each version of the task the participants were asked to decide from which jar the beads were drawn. Two jars of 85:15 different coloured beads were used in the first version, and another two jars of 60:40 different coloured beads were used in the second version. The key variable was the number of beads requested before making a decision (‘draws to decision’). JTC was defined as reaching a decision after two or fewer beads [11].
After administration of the beads task, another mood check was carried out for all participants. If the anxiety state had not then returned to baseline level, debriefing and anxiety reduction procedures were provided.
Measures
The following measures were used in the present study:
Positive and Negative Syndrome Scale
The Positive and Negative Syndrome Scale (PANSS) is a commonly used clinical rating tool for schizophrenia [24]. It has 33 items and consists of the following scales: positive symptoms, negative symptoms, general symptoms and impulsivity symptoms. It was rated by the patient's treating psychiatrist before the anxiety manipulation procedure. A total of five psychiatrists administered the PANSS.
Depression Anxiety Stress Scale
The Depression Anxiety Stress Scale (DASS) is a self-reported questionnaire measuring current experience of depression, anxiety and stress symptoms [25]. It was used to assess trait anxiety and depression in both patients and normal controls in the present study. This study adopted a 21-item short-form of this scale, which was measured before the anxiety manipulation procedure (i.e. at baseline).
Peters et al. Delusions Inventory
The Peters et al. Delusions Inventory (PDI) measures delusional ideation and incorporates the multidimensional assessments of the three key dimensions of conviction, frequency and distress in relation to 21 delusional beliefs [19]. It is suitable for both patients with psychosis and for non-clinical individuals. The PDI was administered before the anxiety manipulation procedure.
Subjective Units of Distress Scale
Participants were asked ‘how anxious are you feeling right now’ and ‘how depressed are you feeling right now’, to be indicated on a visual analogue scale. The Subjective Units of Distress Scale (SUDS) for both state anxiety and state depression were rated by the participants before and after the beads task, and after the debriefing procedure in cases where it was provided. In addition, the patients were asked at baseline, on a visual analogue scale, how much they believed in their delusion. This was to ensure that patients were actively deluded when they performed the experimental task.
Statistical analysis
The data were analysed using SPSS version 13.0 (SPSS, Chicago, IL, USA). Scores on key measures between the two experimental conditions were compared using independent-samples t-test and χ2 tests as appropriate. Paired-sample t-test was used to compare means before and after experimental manipulation, while correlational analyses were used to examine relationships between variables. All hypothesis testing was two-tailed.
Results
Demographic variables
Thirty patients with delusions and 30 non-clinical controls participated. Fifteen of the group with delusions were inpatients, while 15 were outpatients. Eighteen of the patients were diagnosed with schizophrenia, four with acute schizophrenia-like psychotic disorder, three with delusional disorder, two with bipolar affective disorder, one with psychotic depression, and one with psychosis not otherwise specified (NOS). The mean age of the patients (21.60 years, SD = 3.77) and controls (20.07 years, SD = 3.46) was not significantly different (p > 0.05). The patient group, however, had significantly lower levels of education (p = 0.013) and family income (p = 0.019) than the control group.
Baseline clinical measures
According to the patient clinical records, the subtype of the primary delusion was persecution in 17 of the patients, reference in nine patients, and grandiose in two patients. The mean level of delusional conviction in the patients as indicated on the SUDS was 57.2% (SD = 29.3). On a visual analogue scale, 10% of the patients reported 100% conviction, 20% reported 75–99.9% conviction, 30% reported 50–74.9% conviction, 26.67% reported 25–49.9% conviction, and 13.33% reported <25% conviction. The mean PANSS delusion score was 3.53 (SD = 1.383) and the mean PANSS positive subscore was 18.53 (SD = 7.727). Delusional conviction on the SUDS and PANSS subscores were not significantly different between the patients in the two experimental conditions (p > 0.05).
As measured on the PDI before the mood state manipulation, there was no statistically significant difference between psychotic patients and non-clinical controls in number of delusional beliefs endorsed, or in the frequency and conviction measures (p > 0.05, Table 1). In contrast, there was a significant difference (t = 3.27, p = 0.002) in average level of delusional distress between the patient group (2.77, SD = 0.89) and the control group (2.08, SD = 0.71). There was no significant difference between participants in the two experimental conditions (anxiety or relaxation manipulation) on all PDI measures.
Baseline measurements
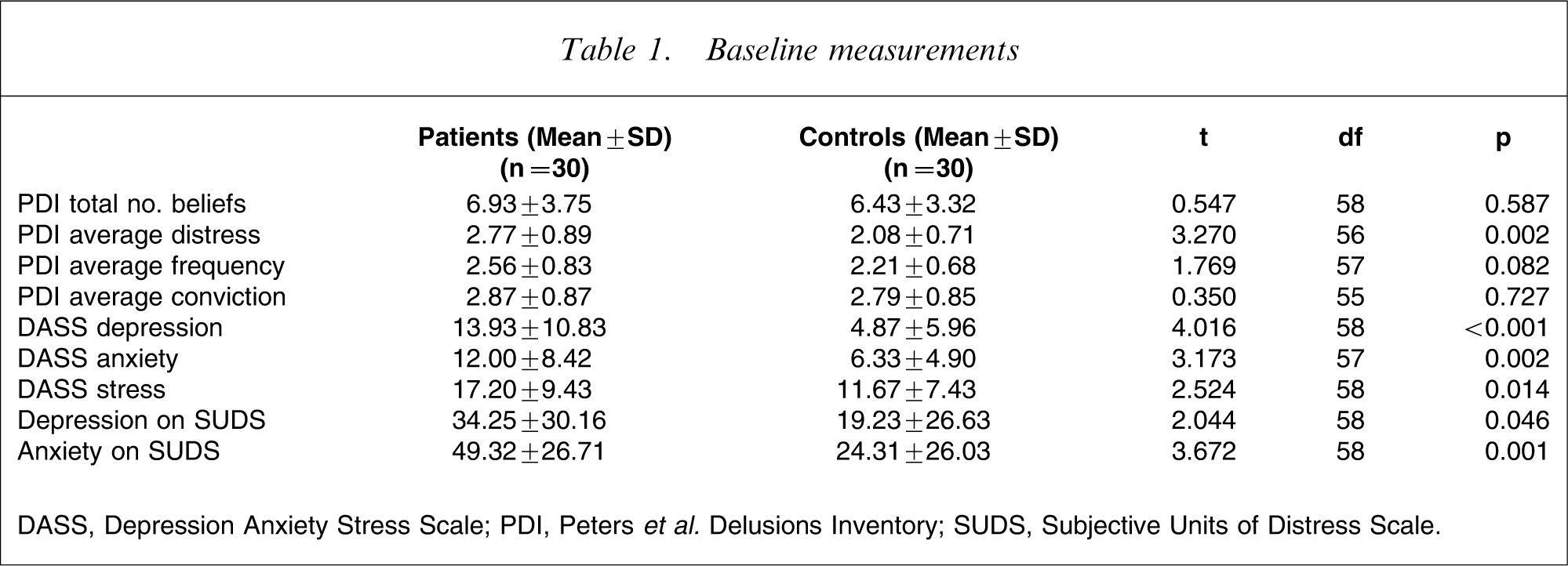
DASS, Depression Anxiety Stress Scale; PDI, Peters et al. Delusions Inventory; SUDS, Subjective Units of Distress Scale.
Trait anxiety as measured on the DASS was correlated with PDI variables including number of beliefs endorsed (r = 0.447, p < 0.001), average level of distress (r = 0.398, p = 0.002), and average level of frequency (r = 0.522, p < 0.001). Both the DASS anxiety subscore and state anxiety as measured on SUDS were not correlated with level of PDI conviction (p > 0.05).
Effect of anxiety state manipulation
As shown in Table 1, trait and state depression and anxiety as measured on DASS at baseline were significantly higher among the patients than the non-clinical controls.
After the anxiety induction the patients had a marginally significant increase in state depression, whereas the non-clinical controls had a significant increase in state depression and state anxiety (Table 2). After anxiety reduction both the patients and control groups had significant reductions in state depression and state anxiety. One patient and six controls needed debriefing after the tests because their anxiety level remained higher than the baseline level of anxiety.
Mood state measurements
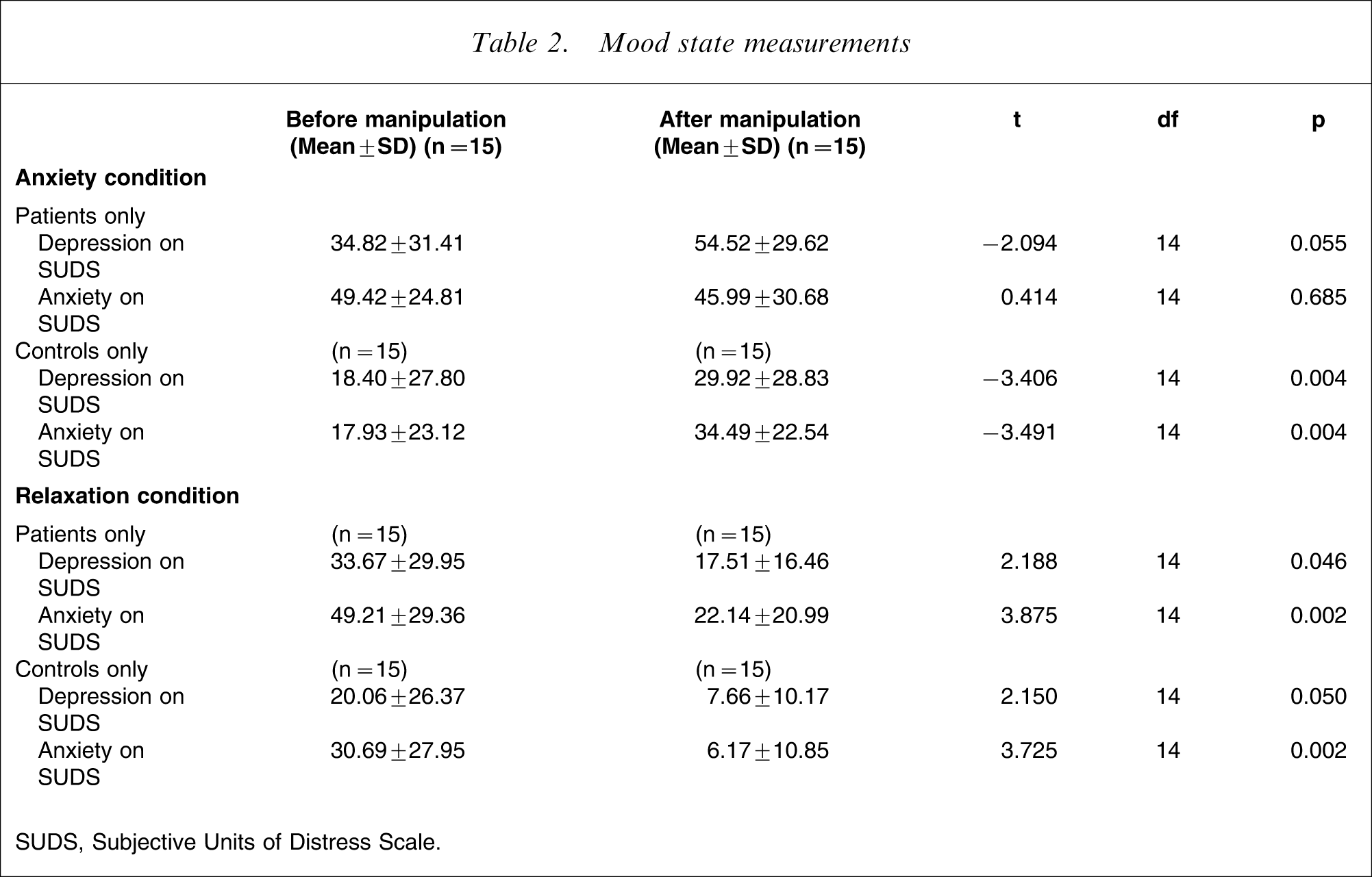
SUDS, Subjective Units of Distress Scale.
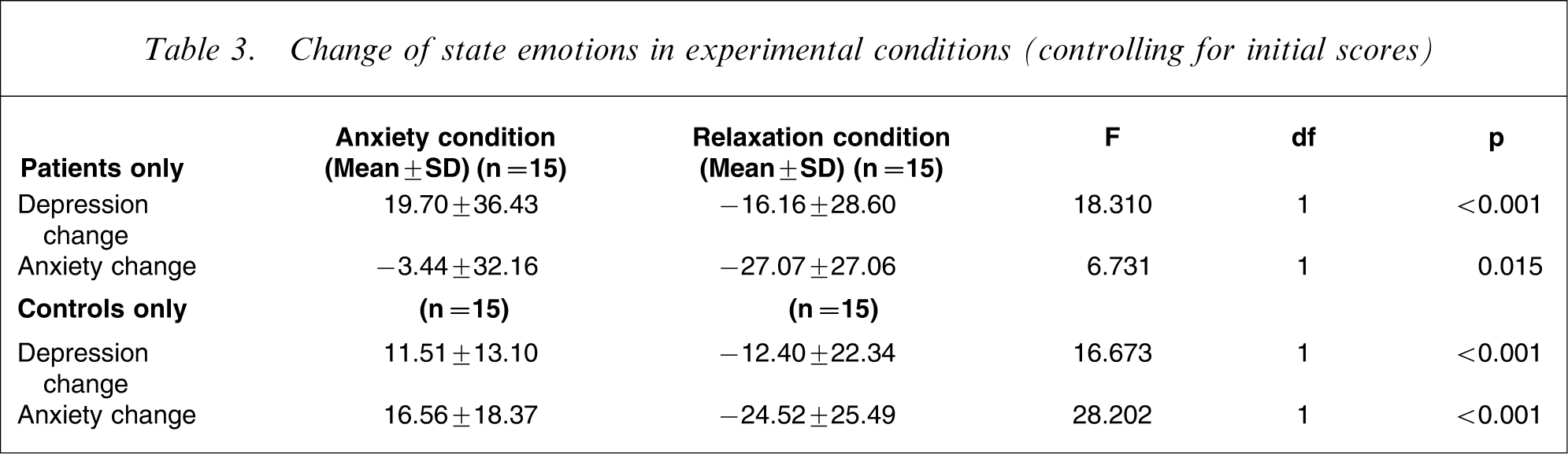
Table 3 shows results of multivariate analyses of covariance. Changes in mood were significantly different between the experimental conditions after controlling for pre-manipulation scores.
Change of state emotions in experimental conditions (controlling for initial scores)
‘Jumping to conclusions’ cognitive bias
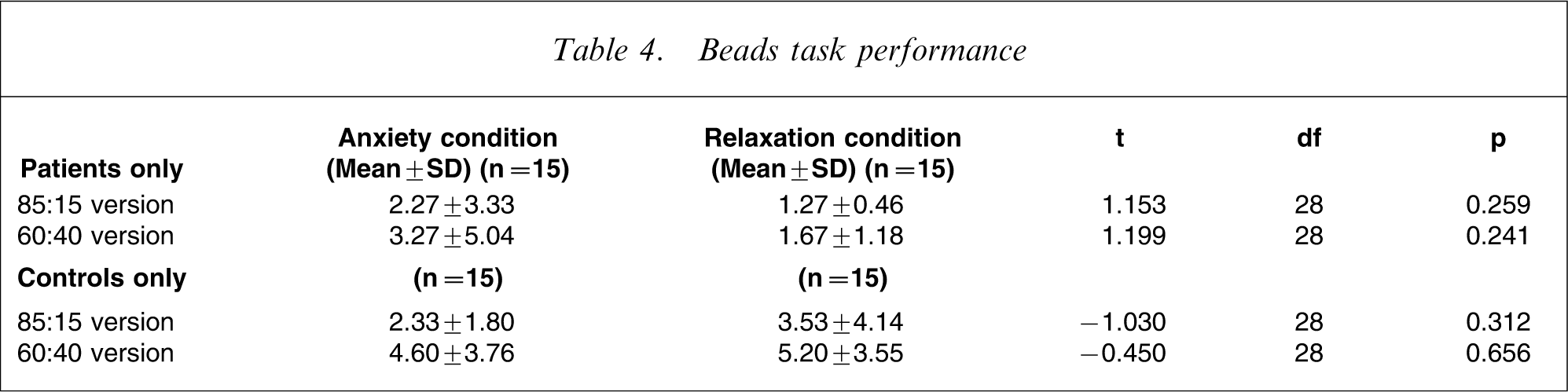
A higher proportion of patients (90% on the 85:15 task, 76% on the 60:40 task) than controls (66.7% on the 85:15 task, and 33.3% on the 60:40 task) reached a decision in the first two draws (hence showing the JTC reasoning bias). This difference was statistically significant for both the 85:15 beads task (χ2=4.812, p = 0.028) and the 60:40 beads task (χ2=11.380, p = 0.001). The average number of beads drawn to decision by patients (2.47, SD = 3.68) and controls (4.90, SD = 3.60) was significantly different (t = − 2.586, p = 0.012) on the 60:40 version of the beads task. No significant difference in mean beads drawn was found for the 85:15 version (patients: 1.77, SD = 2.39; controls: 2.93, SD = 3.19; t = − 1.602, p = 0.115). When analysed separately (Table 4) there was no significant difference in beads drawn or on number of participants showing JTC (p > 0.05) between anxiety induction or reduction experimental conditions, in patients or controls. The number of beads drawn was not correlated to the PDI scores (p > 0.05), in patients or controls.
Beads task performance
Discussion
This study is the first to investigate anxiety state manipulation experimentally in patients with first-episode psychosis, in a group of Hong Kong Chinese subjects. The relationship between changes in state anxiety and the JTC cognitive bias in patients with delusions and in non-clinical controls was investigated.
Imagery induced an effect on mood state in the present study. After the manipulation procedure, in both clinical and non-clinical groups the change in current emotion differed between experimental conditions, even after baseline emotions were controlled for. This is consistent with previous studies using a similar anxiety induction procedure [22], [23]. Patients with psychosis had higher levels of anxiety at baseline. Although both participant groups were responsive to the relaxation (anxiety reduction) imagery, non-clinical controls were more responsive to anxiety induction than patients with psychosis. Therefore, the present study essentially investigated the effects of anxiety reduction in the delusion group and of anxiety induction versus anxiety reduction in the control group.
One possible explanation for the participant groups’ different responses to mood manipulation is that the anxiety imagery procedure required participants to recall and describe an anxiety-inducing situation in detail. This called for memory, organizational power and trust in the experimenter, which might be impaired in patients with psychosis [26], [27]. Furthermore, given the existing high levels of anxiety in the clinical group, the experimenter was careful not to induce especially high levels of anxiety in the clinical group, which might have rendered the procedure less effective.
More patients than controls reached a decision within the first two draws, in both versions of the beads task, thus showing the extreme JTC reasoning bias. Psychotic patients took on average fewer draws than controls before reaching a decision in the more difficult (i.e. 60:40) version of the Beads task. This is consistent with previous studies, in which patients with psychotic delusions had more marked JTC cognitive bias [7], [8].
Both patients and controls in the present study had much higher rates of JTC than in previous studies (previous studies: patients, one-half–two-thirds; controls, 10–20% [10]; present study: patients, 90%; controls, 66.7%). It is not known why this might have occurred. This is the first study in which the beads task was administered in the Chinese language and with Chinese participants. Although translation and back-translation were carefully done, it is not known whether a change in language affected the participants’ performance on the beads task. Also, Chinese people have been found to be authoritarian and to incline to ‘defer to authority figures, anyone who is believed to possess more knowledge than oneself on a given subject’ [28]. It is not clear whether the participants might regard the experimenter as an authority figure and hence became more ready to give quicker responses.
Contrary to the study hypothesis, participants in the anxiety condition did not have more marked JTC cognitive bias than those in the relaxation condition. More specifically, within the patient group, relaxation did not reduce JTC; within the control group, anxiety increase versus decrease had no effect on JTC. This implies that state anxiety and JTC are separate.
Except for delusional distress, patients and controls had no significant differences in other dimensions of psychotic-like delusions. This finding might be considered as partially consistent with previous findings in which a proportion of the non-clinical population shared delusion-like beliefs with patients with psychosis [19–21]. As suggested by other studies, it might be delusional distress that particularly distinguishes the clinical from the non-clinical population [28–30]. It is not typical, however, and indeed surprising, to find no differences between clinical and non-clinical groups in the number of delusional items endorsed and in the levels of delusional conviction; in the present study the clinical group had a wide range of conviction scores, including low conviction. Although other studies also measured patients with active delusions [31–34], the results are not directly comparable due to the use of different assessment tools. Furthermore, the controls had somewhat higher scores on the PDI compared to other studies [31]. There is no apparent reason why the PDI in the present controls was higher. In both the present study and the Peters and Garety study, non-clinical controls indicated neither psychiatric history nor active psychiatric treatment [32]. The unexpected finding of few differences in levels of delusional ideation between the clinical and non-clinical groups produces difficulty for the interpretation of the results.
Consistent with previous findings [35], trait and state anxiety was higher in psychotic patients than in non-clinical controls. Anxiety was correlated only with frequency and distress of delusions, but not with conviction. This finding is consistent with that of the Startup et al. study [13].
Conclusions
This is the first study to investigate the relationship between mood state manipulation and the JTC cognitive bias, conducted in a first-episode population, with Chinese participants, using an experimental manipulation procedure. The key novel finding of the present study is that there is no evidence of a systematic link between state anxiety and JTC. This is consistent with the findings of Garety et al., who suggested that anxiety might exert effects on delusions independent of reasoning, indicating that cognitive and emotional processes act on separate pathways in delusions [11]. Given the present study's methodological issues, however, which we discuss here, this must be considered tentative until replicated. Second, the JTC bias was demonstrated to be present in Chinese patients with a first episode of psychosis, suggesting that it applies across cultures, to Chinese populations as well as to European and North American samples.
Some findings were unexpected and some methodological issues require attention. In particular, there were high rates of JTC in both psychotic and non-clinical groups and we have offered some ideas concerning this. Of the greatest methodological importance, the mood manipulation did not increase anxiety in the psychotic group. We suggest that the imaginal procedure for increasing anxiety may not be feasible or ethically acceptable for patients with psychosis, because it is a methodological challenge to increase the level of anxiety mildly in patients with psychosis, without the risk of an excessive increase that might elicit paranoid ideas. Therefore, different ways of manipulating anxiety in this group need to be explored. Future studies should further explore the relationship between mood state and the JTC bias using newer experimental methods and with more control of possible confounds.
Footnotes
Acknowledgements
This study was not supported by any financial grants or funding. The authors would like to thank Dr P. M. Chan of Kwai Chung Hospital, Dr Steve Tso of Castle Peak Hospital, Professor Patrick Leung of Chinese University of Hong Kong, and other colleagues of these institutions in facilitating recruitment of participants for the present study.