
Abstract
Suicide is a major external cause of death in Australia; in 2005 there were 2201 suicide deaths, with an overall rate of 10.3 per 100 000 [1]. Hanging, poisoning and firearms were the three most frequently used methods.
Suicide through a collision with a train is a method of suicide that may account for up to 12% of all suicide cases [2–4]. ‘Train suicide’ is a highly lethal method, with up to 94% of attempts resulting in death [4]. The cost of train suicide is very high in terms of loss of life, serious physical injury, traumatic impact on the family of the deceased and railway staff, as well as passengers witnessing the incident [5]. Also, suicide by train has financial and organizational costs to railway networks, including delays in services and driver absenteeism [6], [7].
There appear to be particular patterns of risk factors related to the choice of this method. These include young age [8–10], psychopathology (especially major depression and schizophrenia) [11], [12] and a history of psychiatric hospitalization [13], [14]. Environmental and psychological factors, including ease of access to the rail track [15], proximity to mental health institutions [16], and imitation and contagion [17] also might increase the risk and contribute to the popularity of train suicide hot spots [18].
There are no official data on the incidence of rail suicide in Australia because the Australian Bureau of Statistics does not provide disaggregated data for the ICD-10 X81 category of ‘intentional self-harm by jumping or lying before a moving object’, which encompasses jumping and lying in front of trains, trams, cars and trucks [19]. Three studies on train suicide in Australia have been published to date, all from Queensland: Nixon et al. analysed 211 rail accidents (including 10 suicides) for 1978–1981 [20], Emmerson and Cantor presented data on 23 cases of train suicide in Brisbane for 1980–1986 [8], and Milne and Williams reported on 49 rail-related deaths (including 30 suicides) in south-east Queensland for 1990–1994 [21].
The aim of the present study was to report the incidence of suicide on the railway network in Queensland for the period 1990–2004. Sociodemographic, clinical and environmental risk factors are presented and discussed. This work originated from a grant from Queensland Rail in response to an apparent increase of suicide fatalities in recent years.
Methods
Two sources of data were used for the analysis: the Queensland Suicide Register (QSR) and the Queensland Rail (QR) Incident Surveillance Information System (ISIS). QSR is a comprehensive suicide mortality database maintained by the Australian Institute for Suicide Research and Prevention (AISRAP) since 1990. The database contains information from police investigation (inclusive of clinical information), post-mortem, toxicology and psychological autopsy reports (Form 1, which contains all questions formulated by police officers). The psychological autopsy reports are completed by Queensland Police officers in the investigation of possible suicides, following interviews with those close to the deceased, and include information pertaining to psychosocial, behavioural, and demographic data. Form 1 has been designed by AISRAP in collaboration with the Office of the State Coroner. Its last revision was made on March 2007. ISIS is a database system created by QR specifically for the needs of accident and incident (near-miss) reporting to allow analysis of accident and incident trends, and to inform decisions regarding accident reduction and safety improvement strategies.
The databases were cross-checked for cases of deaths on the railway network, which were coded as intentional self-harm by jumping or lying before a moving object (ICD-10 code X-81) or intentional self-harm by crashing of motor vehicle (ICD-10 code X-82). The analysis covers suicide deaths during 1990–2004, the period for which there was complete annual mortality data on both databases. In addition, data on non-fatal suicidal behaviour by collision with a train for the period 1993–2006 were extracted from ISIS records.
Data on sociodemographic and clinical characteristics of rail suicide victims (where available) were obtained from the QSR. Information on gender of individuals involved in non-fatal suicidal behaviour, as well as location and timing of the incidents came from ISIS database.
Results
Fatal suicidal behaviour
There were 8220 suicides recorded in the QSR for the period 1990–2004. This included 161 cases of rail suicide, which accounted for 2% of all suicide deaths in Queensland. On average, there were 11 rail suicide cases per year (minimum of seven in 2001 and maximum of 17 in 2000; Figure 1). The mean overall rail suicide rate of 0.32 per 100 000 remained consistent over the study period (SD = 0.079; SE = 0.02). Based upon data in the QSR and ISIS regarding the incidence of fatal and non-fatal suicidal behaviour, the fatality rate for rail suicides for the period 1993–2004 was 88.7%.
Rail suicide deaths by year, Queensland, 1990–2004.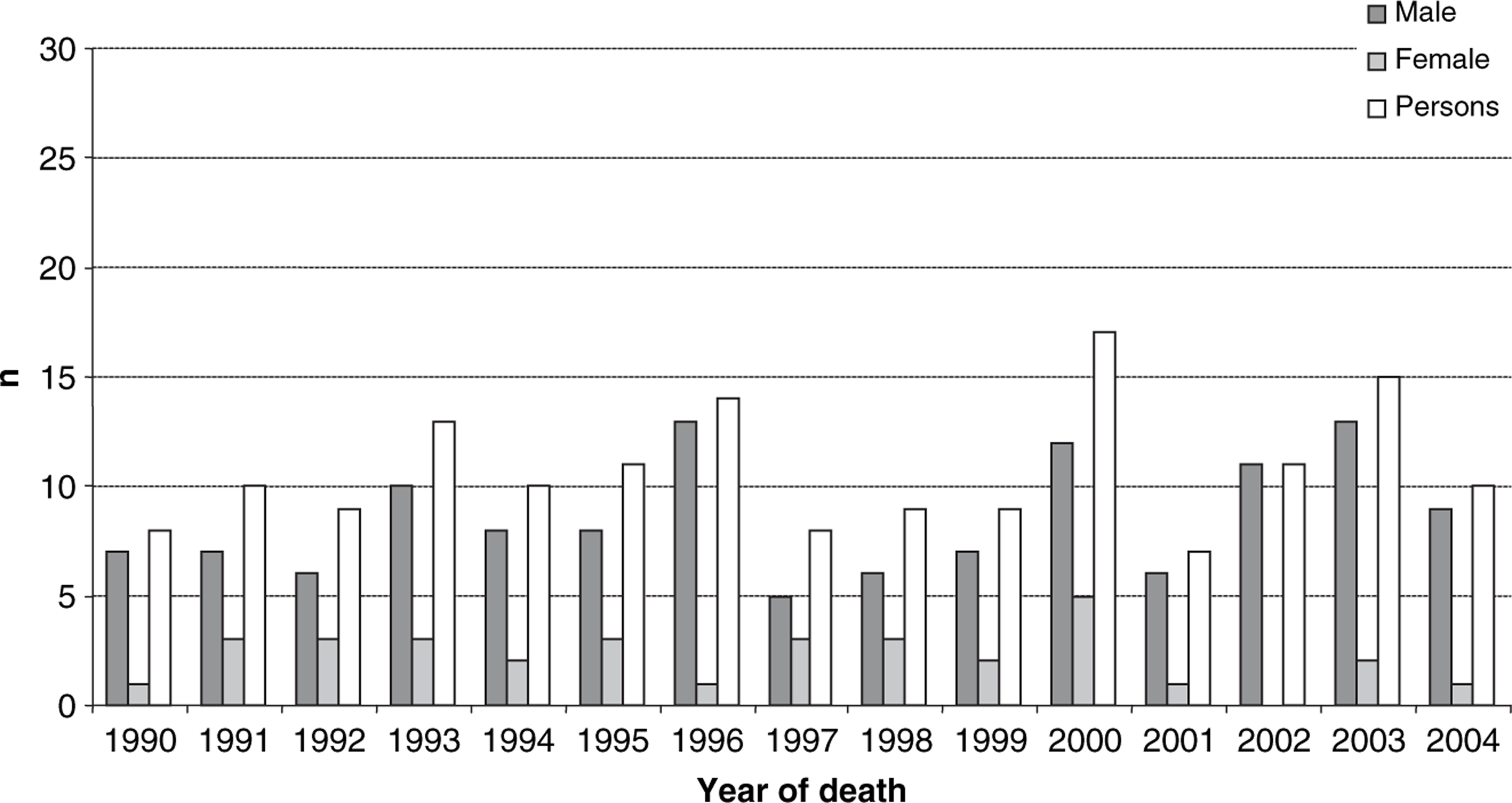
Sociodemographic characteristics
Table 1 presents data on sociodemographic characteristics of rail suicide victims. The male: female suicide ratio was 4:1, with male subjects comprising the majority of the 161 rail suicide victims (n = 128; 79.5%). The mean age of a person dying in a train suicide incident was 32.1 years (SD = 14.3), with young adults between the age of 15 and 34 accounting for 63.9% of cases (n = 103; Figure 2). Although for both genders there were few cases of suicide in subjects >65 years of age (n = 3; 1.8%), the age distribution of rail suicide was different for male and female subjects. There was a peak in the incidence of male rail suicide in the 15–24 age group (n = 48; 29.8%) and a gradual decline with increasing age (χ2=139.48, df = 7, p = 0.000). For female subjects the numbers of suicides were distributed evenly across the 10 year age groups (χ2=10.00, df = 5, n.s.).
Rail suicide deaths by age and gender, Queensland, 1990–2004.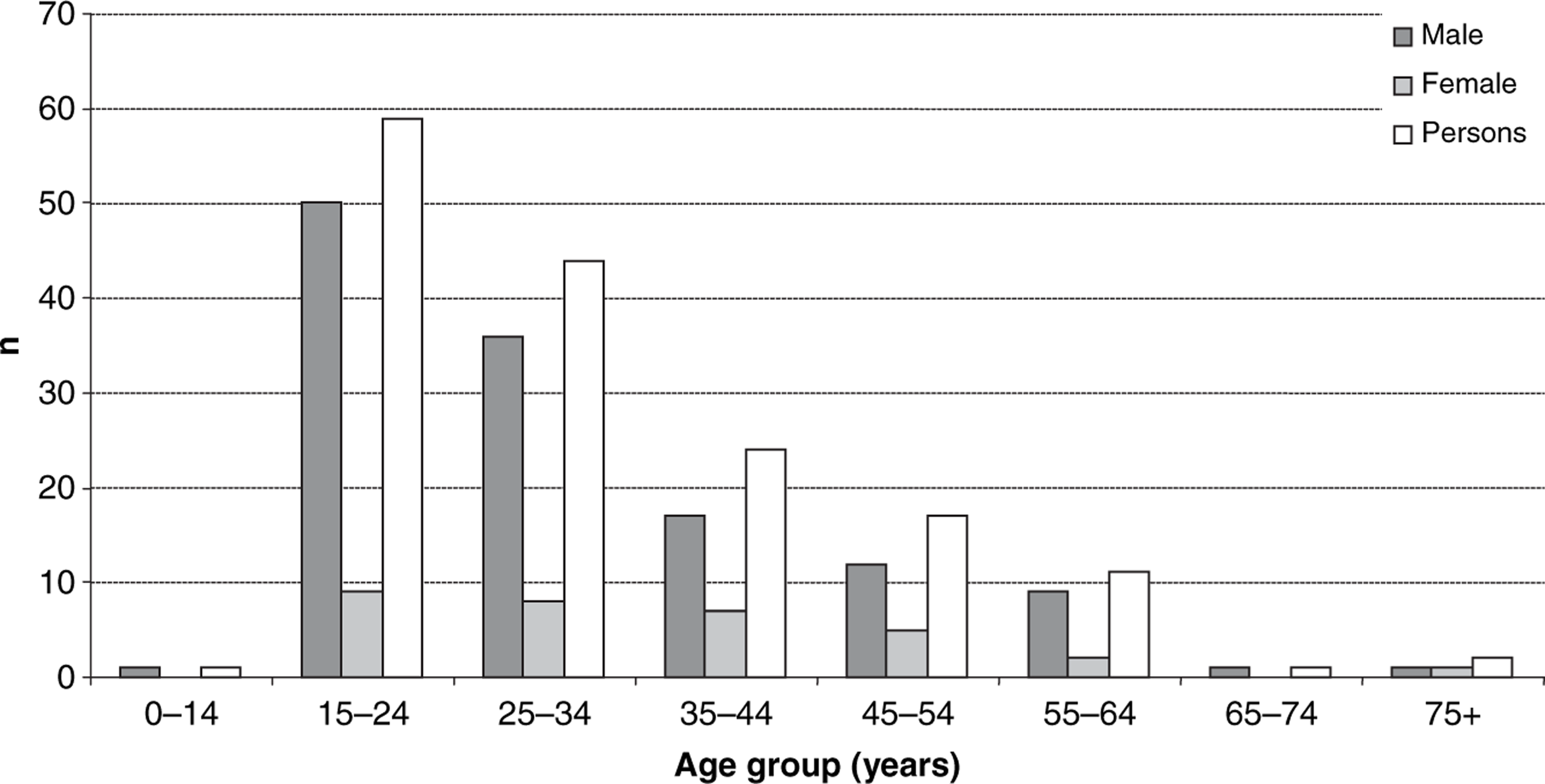
Sociodemographics of suicide victims (n = 161) in Queensland, 1990–2004
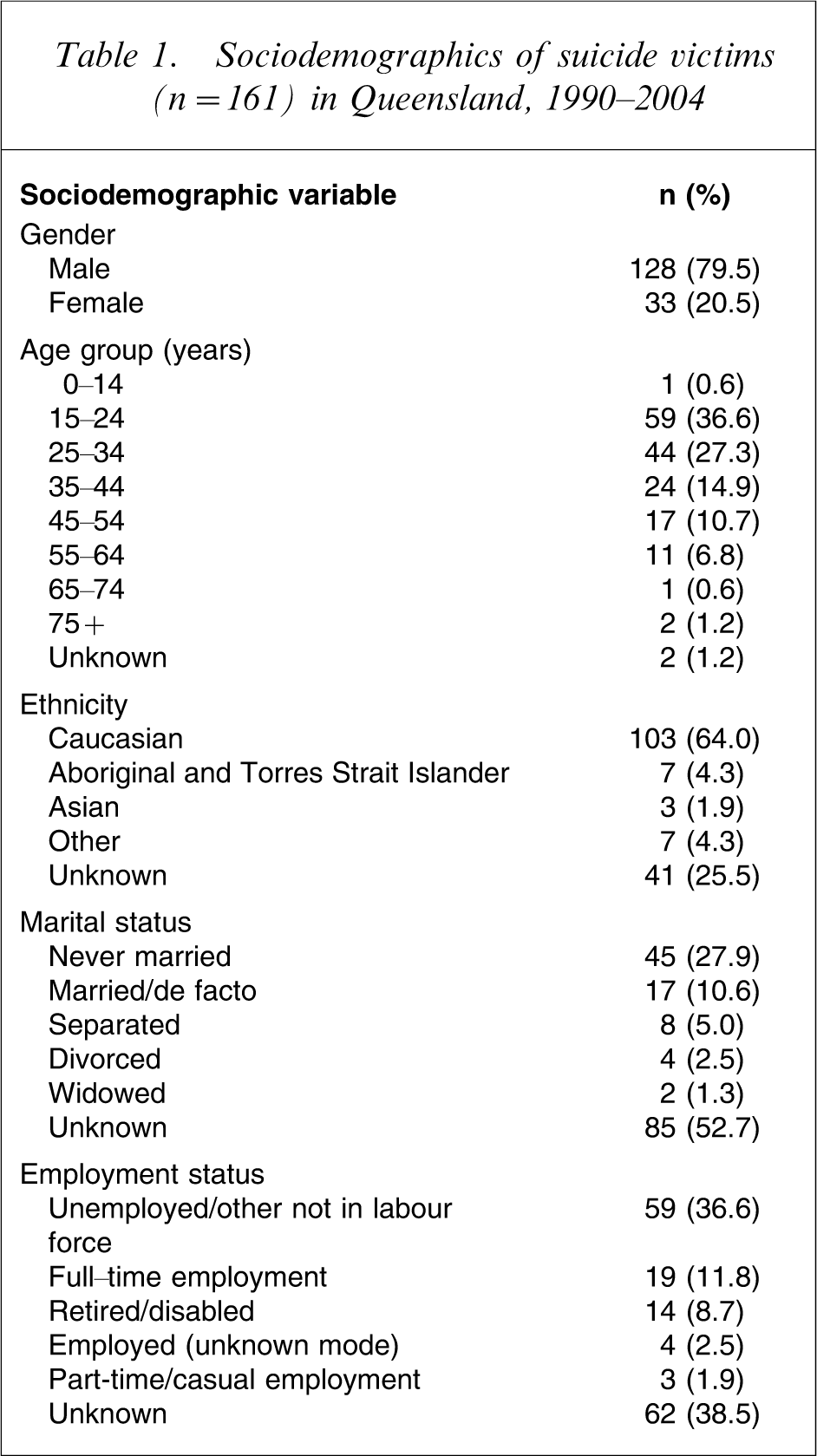
Where information was recorded, more than half of the victims were Caucasian (n = 103; 63.3%; Table 1). Approximately one-quarter of rail suicide victims had never been married (n = 45; 27.9%), while 17 individuals were married or in a de facto relationship (10.6%). Separated, divorced and widowed accounted for approximately 9% of rail suicide cases. A remarkable proportion of victims were either unemployed or not in the labour force (36.6%).
Clinical characteristics
Table 2 presents information on clinical characteristics of people who died on the rail track. Alcohol consumption was particularly frequent in the subsample 15–24 years of age: where toxicological reports were available (55 cases), 26 subjects had positive blood alcohol content (47.3%).
Clinical characteristics of suicide victims (n = 161) in Queensland, 1990–2004
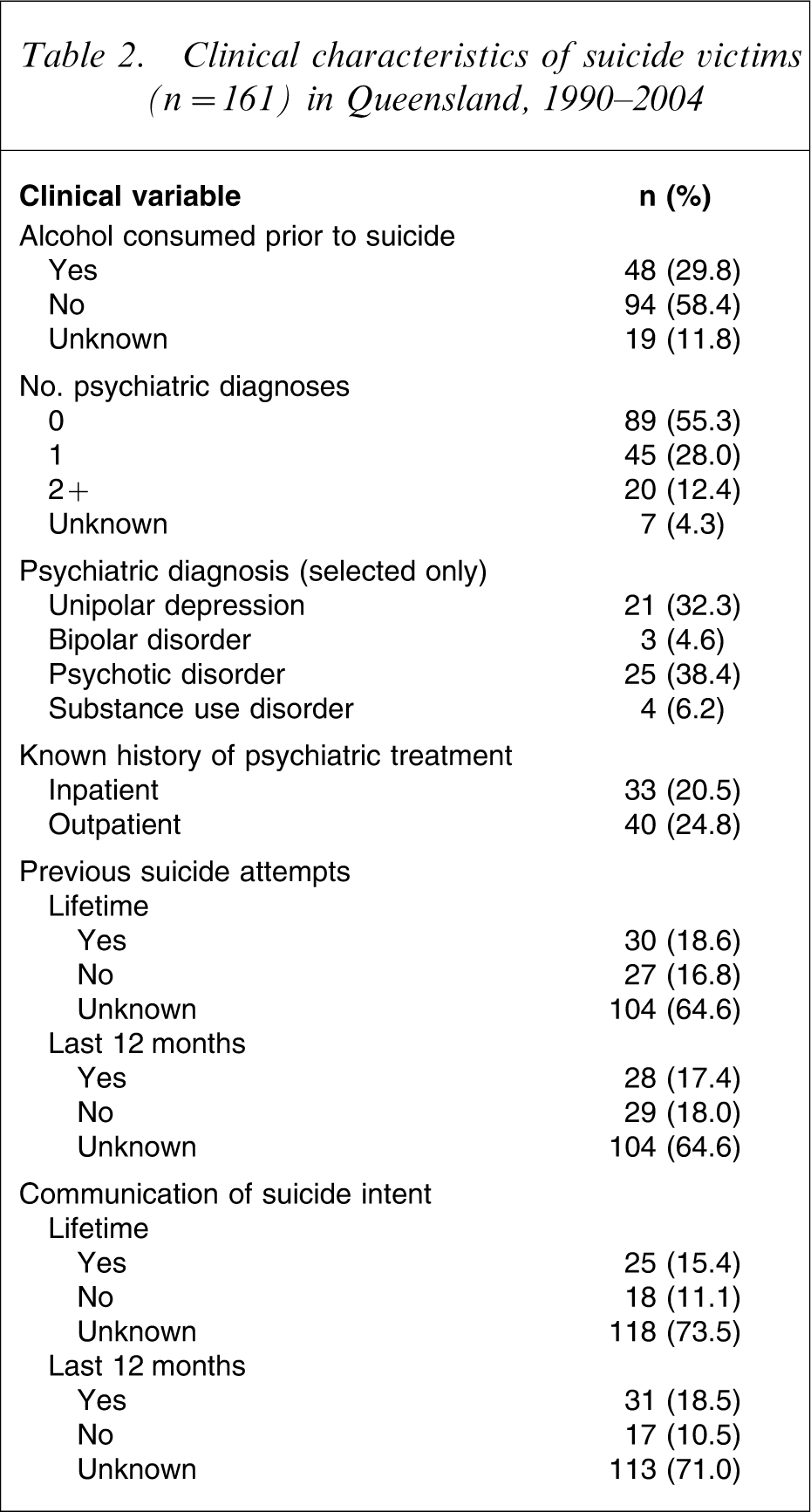
A number of rail suicide victims had at least one documented psychiatric diagnosis (n = 65; 40.4%), mostly psychotic disorder and unipolar depression (38.4% and 32.3%; respectively; Table 2). Other psychiatric diagnoses included substance abuse disorder (n = 4; 6.2%) and bipolar disorder (n = 3; 4.6%). A psychiatric diagnosis was present in 20 subjects aged 15–24 (33.9%); in 24 subjects aged 25–34 (61.5%); in 13 aged 35–44 (56.5%); in four aged 45–54 (30.8%); in three aged 55–64 (27.3%) and in one of the two subjects above the age of 65 years.
Almost half of suicide victims had a known history of inpatient (n = 33; 20.5%) or outpatient (n = 40; 24.8%) psychiatric treatment. A history of suicidal behaviour in the last 12 months before death was reported for 17.3% of rail suicide victims (n = 28) and a lifetime history of previous attempt(s) in 18.5% of cases (n = 30). Although information was available for a minority of cases only (approx. 28%), almost one in five rail suicides had communicated their suicide intent in the last 12 months and one in six communicated the intent in their lifetime (18.5% and 15.4%, respectively).
Circumstances of death
Ten subjects committed suicide while absconding from a psychiatric ward. Two of those cases involved voluntary treatment. In 22 cases a mental health facility was within 500 m of the occurrence of suicide.
The majority of deaths (72.7%) happened in the midsection area (i.e. anywhere on railway land in between a station and a level crossing), and 33 incidents (20.5%) were recorded at stations/platforms. Only a few accidents took place at other locations, that is, level crossings, overhead structures and in a yard (n = 3, n = 3, and n = 1, respectively).
Almost half of the victims (n = 76) died while lying or sitting on track. The remaining victims either jumped/run in front of an approaching train or were hit by a rain while standing/walking on the rail line (n = 34 and n = 33, respectively). There were also four suicides using other methods of death: two crashed their car against an oncoming train, one rode on a bicycle in front of the approaching train, and one was caught by a train while sitting on the edge of a platform.
Several suicide hot spots (i.e. locations with three or more suicides during the study period) were identified. Suicides on three lines (out of 11) accounted for 73.2% of all cases, and deaths at 13 stations (out of 178) comprised one-third of all incidents (34.2%). The highest number of suicide deaths recorded at one station during 15 years was nine suicides.
Timing of suicide
Almost half of suicides (n = 76; 47.2%) occurred in March–May and September–October, while the lowest incidence was observed in June (nine cases during 15 years), but the difference was not statistically significant (χ2=5.882, df = 11, n.s.). Furthermore, the highest numbers of rail suicides were observed on Thursdays (n = 28) and Fridays (n = 29), while the lowest incidence was recorded on Wednesdays and Saturdays (18 cases each), but the difference did not reach statistical significance (χ2=5.043, df = 6; n.s.). Suicide incidents were not distributed equally over the day, but a late afternoon/early evening peak was observed; almost one-third of suicides (n = 50; 31.1%) were recorded between 5pm and 9pm.
Non-fatal suicidal behaviour
There were 18 cases of attempted suicide on the railways in Queensland for 1993–2006: 13 attempts by male subjects (72%) and five (28%) by female subjects. Unfortunately the ISIS dataset was incomplete on several variables: age was recorded for 11 cases only, showing in these cases that eight subjects were between 15 and 34 years old (72.7%); ethnicity was not recorded in two cases; all other but one (an Asian subject) were Australian Caucasian. Clinical information was not available.
Almost half of the attempts (n = 8) involved jumping or running in front of approaching trains; three persons sustained injuries while lying or sitting on the track and one walked onto a track in front of an oncoming train. Three people were injured while getting down onto the track from the platform. There is lack of information regarding the type of suicidal behaviour of three attempters. The attempts were recorded on 17 stations; only one station had two attempts recorded.
Discussion
Queensland Rail commissioned a study descriptive of the population of train suicides. A controlled investigation (e.g. vs accident victims or the general population of suicides in Queensland) was beyond the commissioner's scope and budget, but access to the QSR database permitted a few comparative considerations on some general characteristics.
First, the presence of psychiatric conditions in train suicide cases (40.4%) was in line with the percentage of diagnoses of the entire QSR database: 39.6% (AISRAP: unpublished data, 2008). It is important to underline that data on diagnoses in the QSR are collected by police officers and may involve interviewing (Form 1) several proxies and the general practitioner [22]. Different types of quality-control studies performed by AISRAP on its database have produced different results in terms of frequency of psychiatric diagnoses. When a trained psychologist performed the same interview (Form 1) on proxies of the deceased at 6 month distance from the event, the percentage of detectable psychiatric conditions rose to 55% (representative sample of 100 cases) [23]. When the Structured Clinical Interview for DSM-IV [24] was added to the interview, the percentage increased to 67.5% (consecutive sample of 260 cases; De Leo et al.: unpublished data, 2008). In the present study a high proportion of psychiatric diagnoses was found only in the group aged 25–34 (61.5%), followed by the group 35–44 (56.5%). In the most numerous group (15–24 years of age), however, diagnoses were present only in one-third of subjects.
Apart from overlapping proportions of psychiatric diagnoses, the sample of train suicides is representative of the population of all Queensland suicides only in terms of gender ratio (four male subjects per one female subject). Although in Queensland suicide affects male subjects especially between the ages of 25 and 34 years (followed by the group 35–44 years old) [22], in the sample of suicides examined in the present study it was the group 15–24 years old that was the most affected, both for male and female subjects. Sixty of the 161 subjects in the present study were below the age of 25 years.
In the QSR databank, subjects below the age of 25 had the lowest presence of identified mental disorders: 23% only (AISRAP: unpublished data, 2008). It is of interest to note that in the case of train suicides, the percentage of detected psychiatric conditions for the same age group was remarkably higher (33.9%). Compared to all other cases of train suicide, however, the age group 15–24 was characterized by the lowest percentage of psychiatric conditions.
Positive blood alcohol content was detected in approximately one in two subjects under 25 years of age (47.3%). This is higher than that previously reported in Queensland in a general sample of suicide victims of the same age (43%) [25]. The small number of cases involved imposes a cautious approach to all considerations; but the effects of alcohol on impulsiveness are well-documented [26]. Lack of fencing or barriers along the rail system may allow actualization of suicide impulses.
The present results agree with outcomes of earlier studies on rail suicide in Queensland and internationally in pointing out the relatively small incidence of suicide by collision with a train and its high lethality. Rail suicide accounted for 2% of suicide cases in Queensland and there was no significant increase or decrease in its incidence between 1990 and 2004. Similar results were reported by Emmerson and Cantor in their study of rail suicide in Brisbane for 1980–1986 [8]. Compared to their data, however, in the present investigation the proportion of psychiatric diagnoses was much lower (less than half). The number of fatalities occurring in the vicinity of mental health facilities was also smaller than in the Emmerson and Cantor study: only 22 cases in the present study (13.7%) versus 50% of cases in the previous Queensland investigation. It would be tempting to attribute this noticeable difference to improved psychiatric care (and vigilance) in recent years, as compared to the 1980s to which the Emmerson and Cantor study refers. It is probable, however, that the small number of cases involved in that study (23 vs 161 of the present investigation) constitutes a more plausible explanation.
The present study found that almost nine out of 10 people who attempt suicide on railway tracks in Queensland die as a result of their action (88.7%). Fatality rates reported in other studies range between 43% [2], [26] and 94% [4], [27], with the higher rates observed on railway networks and the lower rates on subway/metro systems. Such a difference might be related to varying levels of controllability of the environment and presence of suicide prevention measures, including blocking access to track and size of area covered by video cameras and other monitoring devices [28]. Clearly, underground metropolitan rail tracks, with access from platforms only, might offer less opportunity for suicidal behaviour than kilometres of easily accessible open track in the countryside (as is the case of QR).
Preponderance of male gender and individuals in younger age groups (15–34 years), as well as vulnerability of people with a history of psychopathology and psychiatric hospitalization observed in the present study, partly confirm findings reported by Abbott et al. [11], Emmerson and Cantor [8], Kerkhof [15], Ladwig and Baumert [9] and Rådbo et al. [10]. Disappointing evidence from the present study is represented by the number of subjects who committed suicide while absconding from psychiatric wards (n = 10). Suicide in this group of people should constitute a very preventable outcome.
Unfortunately there are hardly any data in the literature regarding ethnic, marital, and employment status of train suicides, although a study by Abbott et al. also showed that a large number (36.8%) of rail suicide victims in the UK were unemployed [11].
The overwhelming majority of suicide incidents reported in the study happened in the midsection area (72.7%): approximately 20% of incidents were recorded at stations, and the remaining 4.4% took place at some other location (i.e. a level crossing, an overhead structure, a yard). Similar data concerning location of deaths was reported by the Rail Safety and Standards Board in the UK: approximately 50–60% of suicides occurred on an open track, 30% at stations and 10% at level crossings [29].
Furthermore, almost half of individuals who were hit by a train died while lying or sitting on track, and almost equal, proportions (approx. one in five in each category) jumped/ran in front of an approaching train or were hit by a rain while standing/walking on the rail line. There is a paucity of data concerning behaviour in rail suicides in the published literature and studies use different classifications of behaviour [10], [30], [31]; consequently, it is difficult to compare data in the current study with other studies. A study in Sweden, however, found a different distribution of behaviour patterns in victims: almost half of the suicide victims (44.8%) died when standing or walking on the track, 35.2% were lying or sitting on the track and 14.5% jumped in front of an oncoming train [10].
An autumn peak (March–May) and a spring peak (September–October) were observed. Such peaks were also reported in other studies [10], [32–34]. Contrary to international data, however, the highest numbers of rail suicides in Queensland were observed on Thursdays and Fridays and during late afternoon/early evening hours. The pattern frequently found in the international literature is Monday (and Tuesday) peaks and a low incidence of rail suicide during weekends [9], [17], [32], [33], [35]. Also, late morning and/or early afternoon [9], [32], [34], [35] or midday peaks [2], [36], [37] are frequently reported. Differences in frequency of services during the day/week, and daylight visibility could at least partly account for such diversities among international networks.
Several hot spots were located in proximity to mental health facilities, and/or in the lower socioeconomic status areas, and both factors might affect the choice of a particular station as a popular site of suicide [11], [15]. For example, in the Netherlands 20% of rail suicides happened near large psychiatric institutions [15].
Both databases, QSR and ISIS, included the suicide of Greg Maddox, chief of Energex, which happened on September 2004. The case was amply debated by the media, given the personality involved and the political implications. Apparently, from October 2004 until December 2005 (AISRAP database: unpublished data, 2008), no imitative behaviours eventuated in an increased number of train suicide cases.
Regarding non-fatal suicidal behaviour, there were 18 cases of attempted suicide in Queensland in 1993–2006. Few international studies have looked at non-fatal suicidal behaviour on railway networks [2], [4] and it is difficult to compare Queensland data against their results. What is of particular interest here is the high male: female ratio among Queensland attempters (approx. 4:1), very similar to the gender ratio among completed suicides. A similar result (ratio of 3:1) was found in a study of suicidal behaviour on the subway system in Hong Kong [2]. Although in general female suicide attempters outnumber male attempters [38], the atypical gender ratio found in the present study may be related to the violence of train collision as a method of suicide, which may discourage women from choosing this mode and may indicate a strong motivation to die. This probably means that many, if not most, of those suicide attempts were actually failed suicides.
Limitations
Available datasets were incomplete for a number of variables. Among the sociodemographic ones, the dimension of the unknown was especially relevant with regard to ethnicity (not reported in 25.5% of cases), marital status (not indicated in 52.7% of cases), and employment (not referred in 38.5% of subjects). Prior suicidal behaviour and communication of intent were not indicated in the majority of cases. Generalizability of results involving these variables and some of the sociodemographic ones is consequently limited. Psychiatric diagnoses were reported as a result of police investigation and interviews with the next of kin, as presented in Form 1. It might be that in a certain number of cases diagnoses remained undetected, especially for those conditions not requiring hospital admissions or involving illicit drug use [23].
Conclusions
Almost all railway systems around the world report cases of fatal and non-fatal suicidal behaviour. In Europe – possibly in relation to both population and rail network density – suicidal collision with a train is reported frequently [3], [15]. The proportion of suicides through this method in Queensland is lower (2% on average) and has remained constant in the 15 years examined.
Based upon the largest dataset on suicide by train ever published in Australia, the study allowed for a detailed analysis of incidence of rail suicide in Queensland and sociodemographic and clinical profiles of victims.
The extremely high lethality of collision with a train, comparable to lethality of more frequent suicide methods such as firearms and hanging, calls for special attention regarding research and prevention. The present results agree with other published data, but in the present study a few characteristics emerged more strongly than in previous studies: the particularly young age of many victims, the relatively low percentage of psychiatric diagnoses and the high incidence of positive blood alcohol content in the group of subjects 15–24 years of age.
In the small number of suicide attempts recorded, age and gender ratio were similar to that of suicide victims, possibly indicating serious intention to die of suicide attempters.
Several environmental factors might increase the risk of suicide, including ease of access to the rail track, especially in the case of people using mental health services, potentially contributing to the choice and popularity of the suicide hot spots. Recognition of typical behavioural patterns and popular spots on the rail track can help to identify high-risk locations and design effective approaches to prevention.
Footnotes
Acknowledgements
Thanks are due to Queensland Rail for their financial support and cooperation during all stages of the investigation.