
Abstract
Pro re nata (PRN; ‘as needed’) medication is an archetypal mainstay for managing acute psychiatric inpatient symptoms and behaviours. Psychiatric and mental health nursing practices have circumnavigated the development of a uniform medical–ethical standard for the administration of PRN psychotropic medication. This paper examines the evidence for administration of PRN psychotropic medications and, in the context of evidence-based best practice, current mental health policy and professional ethics, proposes a standardized Australian PRN administration protocol. The procedures and circumstances leading to a nurse administering psychotropic PRN medication are divided into five simple steps, namely (i) medical prescription; (ii) nurse evaluation of patient indications for an intervention; (iii) nurse consideration of therapeutic options; (iv) obtaining patient informed consent; and (v) documentation of outcomes of PRN administration. The literature associated with each step is reviewed, along with national and international professional ethics, guidelines and patient rights documents pertaining to the care of mental health patients. Recommendations for best-practise care are discussed for each step. There is a lacuna of published evidence supporting the use of PRN medications in psychiatric inpatients. Yet there is published evidence that PRN medications are associated with increased risks of morbidity, inappropriate use, may result in above-recommended dosages or polypharmacy, and complicate the assessment of efficacy of regular scheduled medicines. Alternative non-pharmacological treatment options to PRN medication are effective and associated with fewer side-effects. There are no national explicit standards, operational criteria or quality assurance for the use of PRN medication in inpatient psychiatric units. Contemporary PRN practices are largely unregulated and driven by essentially anecdotal evidence, leaving the clinicians and the service open to claims of poor accountability and misuse (intentional and unintentional) of psychotropic medications. Development of best practice guidelines for the use of PRN administration is essential.
Keywords
Admissions to psychiatric inpatient units are usually reserved for acute exacerbations of a mental disorder requiring evidence-based treatment that cannot be provided in the community. Hospitalization can be critical for reducing acute symptomatology, developing or modifying management plans, establishing or re-establishing a therapeutic alliance and providing patients with coping skills and support in preparation for living in the community [1], [2]. Especially in the acute phase of the illness, pro re nata (PRN; ‘as needed’) medication is an archetypal mainstay for managing inpatient symptoms and behaviours.
Administration of PRN medication for psychiatric inpatients is quotidian, with 63–82% of Australian psychiatric inpatients being given PRN medications in settings including open general hospital psychiatric units and secure inpatient units [3–7]. Reported PRN rates for psychiatric patients in the USA are 23–50% [8], [9], Canada 50% [10], and UK 50% [11], [12]. Although the settings for international PRN prevalence may not be directly comparable to the Australian data, we note that the prevalence of PRN medications in Australia is higher than other developed countries. Patient request of PRN medication comprises only 20–36% of PRN administrations, with the remainder being instigated by a nurse [3], [8], [11], [13–15].
For the nursing staff there are definite advantages to PRN psychotropic prescriptions in that it allows administration of medication rapidly in acute situations, supposedly reducing the need for more invasive and restrictive interventions such as physical restraint or isolation, and reduces the need to contact the treating medical practitioner [16], [17]. It has been suggested that over-reliance on PRN medication has propagated restraint, albeit chemical rather than physical [18], [19]. Restraint of any form is associated with ethical quandaries. One proposition is that PRN orders may titrate medication to symptoms, resulting in lower dosages [20], although this was not borne out in a recent study [15]. There are significant risks associated with PRN medication. PRN medication can confound the assessment of the efficacy of regular medication [21], may result in high (above-recommended) dosages [22], polypharmacy (e.g. mixture of typical and atypical antipsychotics) [5], [23], adverse drug interactions [12] and increased morbidity [1], [5], [21], [24]. Some evidence indicates that administration of PRN medication may be more for nursing reassurance than a patient's clinical need [17]. Contemporary PRN practices are largely unregulated and driven by essentially anecdotal evidence, leaving the clinicians and the service open to claims of poor accountability and misuse (intentional and unintentional) of psychotropic medications.
The evolution of psychiatry and mental health nursing best practice has skirted the development of a uniform medical–ethical standard for the administration of PRN psychotropic medication. Currently, for psychiatric inpatients, the decision to administer PRN medication resides with a single nurse who has little in the way of standards to guide their decision. In this area, psychiatry and nursing have not fulfilled their commitment to provide best-practice evidence-based ethical care. This paper examines what evidence there is for administration of PRN psychotropic medications and, in the context of current mental health policy and professional ethics, proposes a standardized Australian PRN administration protocol.
The decision-making process in the administration of PRN medication occurs in the complex settings of patient–doctor, patient–nurse, nurse–doctor interactions, patient history, mental state and operational demands/local policy. Complicating this system is that mental health inpatient units involve patients with protean symptoms. This apparent complexity has, in all probability, perpetuated the belief that individual nursing judgements are most appropriate in deciding what, when and how much PRN medication to administer. The perceived complexity may have also precluded the development of standardized procedures for the administration of PRN medication. Due to enhanced identification and classification of mental disorders, the advent of a wider range of pharmacotherapies, a greater understanding of the benefits of psychological therapies, better recognition of morbidity associated with medications (including PRN use of medication), lack of empirical evidence on the long-term efficacy of PRN medication and a greater appreciation of the rights of mental health patients, the process of PRN drug administration warrants a critical review. The World Health Organization (WHO) Guidelines for the Promotion of Human Rights of Persons with Mental Disorders (p.20) [25], Principle 10 states that only medication ‘… of known and demonstrated efficacy …’ be used for mental health patients and that ‘there should be guidelines on the indications and use of drug therapies’. This paper deconstructs the PRN process into simple compartmentalized steps to facilitate the development of such guidelines.
Step 1: PRN prescriptions
The first step in the PRN system is the prescription of medication(s). The prescribing physician deliberates their clinical findings and considers guidance from the nursing staff. In an Australian study, Geffen et al. found that only 6% of medical PRN prescriptions specify indications for administration of medications [5]. This focuses the responsibility for the interpretation of ‘as needed’ almost exclusively on the nursing staff. In Australia it has been noted that nurse views on indications for giving PRN medications to inpatients substantially differ from the prescribers’ intention [1], a view supported by UK research [17]. Many psychiatric nurses do not have the knowledge or experience to assess patients for PRN drug administration [21], [26]. Nurses, more commonly than doctors, supply PRN medications inappropriate for the presenting symptoms (e.g. anticholinergics for tardive dyskinesia) [1]. Additionally, it is common practice for physicians to prescribe different PRN medications concurrently, leaving the decision of which medication to administer to the nurses [1]. It is routine for PRN orders to contain a range of medication dose [8], [21], so that the nurse is responsible for determining the PRN dose necessary.
In line with the WHO recommendations [25], the Royal Australian and New Zealand College of Psychiatrists (RANZCP) Code of ethics clearly states that ‘Psychiatrists shall seek informed consent from their patients before undertaking any procedure or treatment’ [27]. The ethics statement makes clear that informed consent is an explanation and discussion of risks, side-effects, and alternative therapies. PRN medication doubtlessly falls into the category of ‘any procedure or treatment’. Thus, in the case of multiple drug PRN prescriptions each medication needs an explanation and rationale presented to the patient. If varying dosages are present on the PRN prescription, the rationale for this requires discussion with the patient.
Previously, recommendations have suggested that PRN medication orders specify indications for use and a maximum frequency or maximum daily dose [5], [10]. A recent (2007) Delphi study on best practice for PRN psychotropic medication in the UK shows the consensus of expert opinion, in regards to the prescription of PRN medication, to be: (i) a clear focus as the purpose of PRN medication; (ii) clear goals underpinning the use of PRN; (iii) clear description of indications; (iv) a time-limited PRN prescription with regular review; and (v) an awareness of any potential side-effects, drug interactions and/or allergies when prescribing PRN [28].
In developing a standardized PRN policy, we recommend that prescribing medical practitioners: (i) include clear indications for use when prescribing PRN medications; (ii) limit the number of PRN medications to the minimum required; (iii) specify medication doses and/or maximum daily dose; and (iv) unless otherwise indicated in statutory provisions, ensure that the patient consents to the reason for use of the medications and understands potential side-effects and alternatives.
Step 2: Nurse evaluation of indication for intervention
The prevailing reasons for PRN administration of medications to inpatients are to ameliorate agitation, patient distress, anxiety, sleep disturbance and prevention of aggression or hostility [3–6], [8], [10], [13], [14], [17], [29]. Although standardized rating scales for assessing levels of agitation, sleep disturbance or many other symptomatic domains exist, the use of these individual symptom scales in regards to PRN medication in a clinical setting has not been well researched. The appropriate scale to select in what circumstance and the best way to administer it poses inherent difficulties. The development and testing of an appropriate, and broadly applicably scale, for the administration of PRN medications in psychiatric inpatients would be immensely useful. This is common practice in the treatment of alcohol withdrawal, where the Alcohol Withdrawal Scale (AWS) determines the use of PRN medication. Until such a time, for consistency and ease of implementation, a comprehensive clinical evaluation by the nurse (which could include the use of standardized rating scales) is likely to be the best option for assessing the need for PRN medication.
Four Australian studies in psychiatric inpatient units reported that nurses failed to record the indications for use of PRN medication for between 38% and 63% of administrations [3], [5–7]. Two other Australian studies in much smaller close observation psychiatric units (eight and nine beds) reported PRN indication documentation failure rates of 9% and 14% [4], [30]. Variability in nurse documentation of indication for PRN medication may be related to the size and function of the inpatient units.
The six Australian studies discussed here are limited to one or two inpatient sites [3–7], [30]. There are no large-scale data on PRN administration in Australia but the existing evidence points to great variability in PRN practices between inpatient mental health units. An absence of clear national standardized guidelines on the use of psychotropic PRN medications may contribute to this variability.
The failure of nursing staff in these studies to record the indication for PRN medicines leaves open the question as to what evaluation was undertaken to arrive at the decision to use the medication and, if there was an indication, whether it corresponded to that of the prescribing physician. The standards of practice for mental health nursing in Australia state that one of the requirements of a mental health nurse is to ‘document assessment results, health care/treatment plan, strategies for care and outcomes of care’ [31]. The available evidence suggests that this nursing standard, as applied to PRN medication, is not being met on many occasions. The WHO Guidelines for the promotion of human rights of persons with mental disorders Principle 8.2 states that, ‘every patient shall be protected from harm, including unjustified medication …’ [25]. Any lack of clinical assessment prior to PRN administration and/or an absence of recording of indications in the clinical record jeopardize the basic right of the patient to have medication that is clinically justified. Overseas evidence suggests that these concerns are warranted. Baker et al. in the UK found that 71% of mental health professionals surveyed encountered instances when PRN medication was used for reasons other than the prescribed indications [17]. Furthermore, item 8.2.6 of the WHO guidelines raises the questions, ‘Are medication orders left such that nursing staff may administer drugs on an ‘as needed’ basis? If so is this practice ever abused for the convenience of the staff?’ [25]. Baker et al. reported that two-thirds of PRN medication was administered at regular medication round times for convenience [17].
In developing a standardized PRN policy, we recommend that: (i) a clinical assessment is mandatory prior to the use of PRN medication; (ii) the indications for the PRN intervention and circumstances leading up to the intervention are to be clearly documented in the patient's clinical record; and (iii) unless otherwise indicated in statutory provisions, nurse-initiated PRN medication must be in accordance with documented medical indications.
Step 3: Nurse consideration of alternative therapies
For a mental health inpatient with acute symptoms and behavioural disturbance, it is time efficient and relatively uncomplicated for the nursing staff to use PRN medication. Alternative, non-pharmacological treatment options may be overlooked. In an Australian study, Curtis et al. found that in 73% of PRN administrations no other therapeutic intervention was documented as occurring prior to the use of the PRN medication [7]. Constant reliance on PRN medication does not teach the patient the coping skills required to function in the community [15], [32]. The alternatives to PRN medication involve some form of therapeutic psychological treatment (such as de-escalation, counselling, distraction, time out, reality testing, relaxation and cognitive behavioural therapy), which are more labour intensive than pharmacological interventions. In certain circumstances, talking with the patient about the issue may resolve the problem, reducing the need for medication [19], [33] and facilitate the acquisition of life skills required on discharge [2]. Talking strategies/treatments are associated with the least risk to the patient, and should be considered the first line of treatment [7], [18], [34], [35].
In mental health nursing, as in any profession, a gradient of experience and expertise exists. Nurse seniority is related to the perceived number of available alternatives that can be used instead of PRN medication [1]. The standards of practice for mental health nursing in Australia state that ‘mental health nurses be familiar with the principles and process of counselling and its role in health care provision’ [31].
Low staffing levels, organizational and environment pressures, time restraints, a lack of skill and experience are factors contributing to a preference for nurses to administer PRN medications over non-pharmacological treatments [17], [36–38]. Reports indicate that only 5–7% of qualified nursing time is spent on nurse–patient psychotherapeutic activities [39], [40]. It has been demonstrated in the USA that increases in nursing staff levels in inpatient units decreases seclusion and restraint [41]. It is likely that such a relationship exists for PRN medications. Studies have linked nursing evening and night-time shifts with increased PRN administration [3], [7], [8], [10], [13]. This suggests that reduced staffing levels may promote PRN medication, but additional time-of-day effects cannot be ruled out from these studies. A survey of nurses identified that their ability to use non-pharmacological treatments was tempered by the hospital ward milieu and staff skill levels [1].
It is important to recognize the clinical skill of mental health nurses, the emerging role of clinical nurse practitioners and the individuality of patient requirements. Any guidelines for use of PRN medications must have a provision that allows for the nursing staff to make a clinical decision to administer medication if they have legitimately determined that this is needed by the patient, or in circumstances where there is imminent danger of self-harm or harm to others. Senior nurse practitioners, who have additional training in clinical assessment and treatment, would be expected to be able to apply critical decision making in alternative therapies. To improve accountability in the administration of PRN medication where ambiguity exists in the medical documentation or the patient's clinical presentation, less experienced nurses should discuss the situation with a more experienced nurse and document that discussion in the clinical record. This may serve to minimize intra-individual variability in the assessment of the requirement for PRN administration.
In general, it is recommended that psychiatric inpatient units have access to senior nurses and sufficient nursing staff on duty to allow the provision of non-pharmacological therapies to patients where this is clinically indicated in lieu of PRN medication. In developing a standardized PRN policy we recommend that the following.
Each inpatient unit determines a level of nursing qualifications and experience, below which the clinical assessment/needs of the patient are discussed with a senior nurse/colleague and the outcomes of discussion documented before administration of PRN medication. Non-pharmacological treatments are always considered prior to the use of PRN medication. Reasons for deciding that PRN medication is more appropriate than non-pharmacological treatments are recorded in the patient's clinical record.
Step 4: Patient informed and consented
When it comes to PRN medications, patient informed consent is frequently overlooked [17]. A failure to provide patients and relatives or carers with information about PRN medication has been identified in Australia [30] and the UK [17], [42]. The issue of psychiatric inpatient informed consent for PRN drug administration is beset by a history of inadequate clinical practice guidelines, inconsistency and poor documentation. Baker et al. found that the consensus of expert opinion in 2007 was that the patient, wherever possible, should be involved in the decision-making process (including the rationale and indications), and should receive information about any perceived risks and have their questions answered [28].
The WHO Guidelines for the promotion of human rights of persons with mental disorders Principle 11 states the following.
No treatments shall be given to a patient without his or her informed consent. … Except in the certain instances such as the patient is held as an involuntary patient or, an independent authority has judged that the patient is not capable of the capacity to give or retain consent or, imminent harm to the patient or others, among other circumstances. [25]
The lack of documentation of indications for PRN administration (discussed previously) calls into question the issue of whether the patient has supplied informed consent for taking the PRN medication. Research indicates that <50% of psychiatric inpatients receive information about their PRN medication and that discussions about possible side-effects tend to occur when the staff did not want a patient to take a particular drug [17]. The quandary is, have the indications for use, potential side-effects and alternative therapeutic options been adequately explained to the patient? A prescription for PRN medication does not abrogate the medical or nursing responsibility to obtain informed consent prior to prescription or administration because, as highlighted in the RANZCP code of ethics [27], a patients’ consent may fluctuate over time. The Australian Nursing and Midwifery Council, Royal College of Nursing, Australia, Australian Nursing Federation Code of ethics for nurses in Australia value statement 2.1 states the following.
Individuals have the right to make decisions related to their own health care, based on accurate and complete information given by health care providers. Nurses must be satisfied that they have the person's consent for any care or treatment they are providing. If individuals are not able to provide consent for themselves, nurses have a role in ensuring that valid consent is obtained from the appropriate substitute decision-maker. [43]
This statement makes it clear that PRN (any care or treatment) requires informed consent, unless there are statutory reasons to proceed without it.
The Australian Mental Health Statement of Rights and Responsibilities of mental health patients does not specifically address PRN medication but rather treatment in general. Considering PRN medication as treatment, there are three key patient rights pertaining to administering PRN medication: (i) the right to appropriate and comprehensive information, education and training about their mental health problem or mental disorder, its treatment and services available to meet their needs; (ii) the right to interact with health-care providers, particularly in decision making regarding treatment, care and rehabilitation; and (iii) the right to refuse treatment (unless subject to mental health legislation) [44].
Thus, a patient has the right to information and education about PRN medication, a right to be involved in the decision-making process of PRN medication and the right to refuse medication. This position is supported by the National Standards for Mental Health Services [45], which state the following.
The MHS (Mental Health Service) obtains the informed consent of the consumer prior to the administration of medication or use of other medical technologies such as electroconvulsive therapy.
The consumer and their carers are provided with understandable written and verbal information on the potential benefits, adverse effects, costs and choices with regard to the use of medication and other technologies.
Although none of these policy documents specifically defines PRN medication as a treatment, this is implicit. Therefore, we recommend that the nurse must obtain the patient's informed consent at the time of delivery of PRN medication. Patients have the right to refuse PRN medication (except in statutory defined circumstances where involuntary treatment is authorized). Because patient informed consent is a key ethical and moral right, we recommend that patient consent to PRN medication be annotated in their clinical record.
Step 5: Outcome of intervention recorded
Assessment of PRN medication outcomes has been lackadaisical at best, with between 23% and 61% of PRN administrations clinical outcomes not recorded [3–7], [30]. Additionally, in only 4% of nurses and 0% of doctors was an assessment of side-effects considered as an outcome of PRN medication [1]. Lack of documentation and evaluation of side-effects is a serious problem with PRN psychotropic medications and casts doubt on whether adequate assessment of the patient was performed after PRN medication administration. Because all psychoactive drugs have been associated with the potential for disabling side-effects, and PRN medication significantly relates to morbidity [5], a clinical documented review of the patient following PRN administration should be a nursing requirement.
Standard 10 of the National practice standards for the mental health workforce state: ‘Mental health professionals maintain a high standard of documentation and information systems on clinical interventions and service development, implementation and evaluation to ensure data collection meets clinical, monitoring and evaluation needs’ [46]. The available evidence suggests that appropriate documentation of PRN medication outcome does not meet national practice standards and is in need of urgent attention. If outcomes and side-effects are not recorded then it is impossible to determine clinical effect, thus restricting the doctor's ability to formulate informed decisions regarding future prescriptions/treatments. We recommend that (i) clinical outcome of PRN medication be assessed and documented; and (ii) an evaluation of side-effects is conducted, including feedback from the patient on their experience of the PRN medication, and that these are documented.
Other issues
Covert administration of PRN medication
In aged care facilities, covert medication administration is common practice [47], [48], but there is no literature on the presence or prevalence of covert administration of PRN medication in psychiatric inpatient facilities. Although covert medication is likely to be less frequent in psychiatric units than in aged care facilities, it is the authors’ experience that the practice does occur.
There have been efforts to develop policies to address the need for covert administration of PRN medications in aged care facilities [47], but we believe that there is no situation in which covert administration of PRN medication should occur in mental health facilities. Even an involuntarily detained patient receiving involuntary treatment should have information about their treatment and the right to participate in the decision-making process. Informed consent for medication is a basic right of persons with mental disorders specifically mentioned by the WHO [25], the RANZCP Code of ethics [27], the Australian Nursing and Midwifery Council Code of Ethics [43], the Commonwealth Mental Health Statements of Rights and Responsibilities [44], and the National standards for mental health services [45]. There is no research or documentation discussing the application of covert medication. Due to an absence of any empirical evidence, ethical or procedural guidance there is no argument that can substantiate covert psychotropic medication. We recommend that a national policy on PRN psychotropic medication prohibit covert PRN medication.
Involuntary admission and/or treatment of mental health patients
In regards to involuntary patients, the recommendations discussed here still apply. There should be appropriate, accountable prescribing of PRN medication, adequate clinical assessment of need for PRN medication, recording of indications, consideration for non-pharmacological therapies and a clinical record of outcomes. The only difference is informed consent. In fact, the only difference is consent. The involuntary patient retains the right to be informed about medications, side-effects and possible alternatives.
Discussion
The Australian National Mental health statement of rights and responsibilities under ‘Standards’ states that ‘The consumer has the right to have explicit standards set for all sectors of service delivery and that such standards should have operational criteria by which they can be assessed’, and ‘The consumer has the right to have services subjected to quality assurance to identify inadequacies and to ensure standards are met’ [44]. Currently, despite 30 years of sporadic research on the inadequacies of PRN medication practice, there are no national explicit standards, operational criteria or quality assurance for the use of PRN medication in inpatient psychiatric units.
The National standards for mental health services state, ‘Medication and other technologies used are evidence-based and reflect internationally accepted medical standards’ [45]. National and international codes of practice and ethics documents discussed in the current paper indicate that mental health patients have a right to evidence-based treatments. A recent systematic review found no studies comparing the effects of regularly scheduled medication to PRN medications for psychotic illnesses [20]. There is a lacuna of published information indicating that PRN medication results in better long-term clinical patient outcomes than regular scheduled medication or non-pharmacological interventions. Psychoactive PRN medications are, in many cases, administered to achieve secondary short-term outcomes, such as sedation, in response to primary situations such as agitation or a perceived patient danger to themselves or others. Thapa et al. demonstrate that the occurrence of patient restraints, patient seclusions, aggressive incidents or employee injury reports (all surrogates of short-term outcomes) are not significantly different between times when PRN was allowed and not allowed in an inpatient unit [15]. Policies and procedures for the prescription and administration of PRN medications in psychiatry and allied services have been grandfathered in from practices pre-dating the development of ethical guidelines for the treatment of psychiatric patients. This is not to suggest that no benefits to PRN medication exist but rather, there is a dire need for quality research to establish an evidence base for the use of PRN medication, if its use is to continue.
There is a small evidence base indicating that PRN medication does not significantly change patient long-term or short-term outcomes [15]. There is published evidence that PRN medications are associated with substantially increased risks of morbidity [1], [5], [21], [24] and potentially mortality [12], inappropriate [1] or unnecessary [15] use, may result in above-recommended dosages [22], complicate the assessment of efficacy of regular scheduled medicines [21], and have the potential for polypharmacy [5], [23] and physical addiction [19]. Alternative non-pharmacological treatment options to PRN medication are associated with reduced side-effects and have been shown to be effective [15], [19], [32], [33].
The mental health system has been inadvertently recalcitrant in supporting a risky practice that has a skeletal evidence base to promote it. To protect patient health, well-being and rights, and the professional standing of mental health staff, specific standard operating procedures for the prescription and administration of PRN medications are required. Numerous reports over the last 30 years have discussed individual problems of PRN medications but none has fused the scientific information with codes of best practice and ethics statements to establish a set of suggested recommendations for the development of national guidelines/standards pertaining to PRN medication for psychiatric inpatients. Figure 1 is a suggested decision-making process and key clinical documentation required in the prescription of PRN medications and the nursing response to inpatient situations requiring an intervention (non-pharmacological treatments, PRN medication, restraint etc.).
Suggested protocol and decision-making process for the administration of pro re nata (PRN; ‘as needed’) medication to psychiatric inpatients. This figure excludes those on an involuntary treatment order and is not meant to supersede standardized best-practice procedures for the prescription and administration of medication. Rather, the decision-making process indicated should supplement and encourage adherence to best-practice procedures.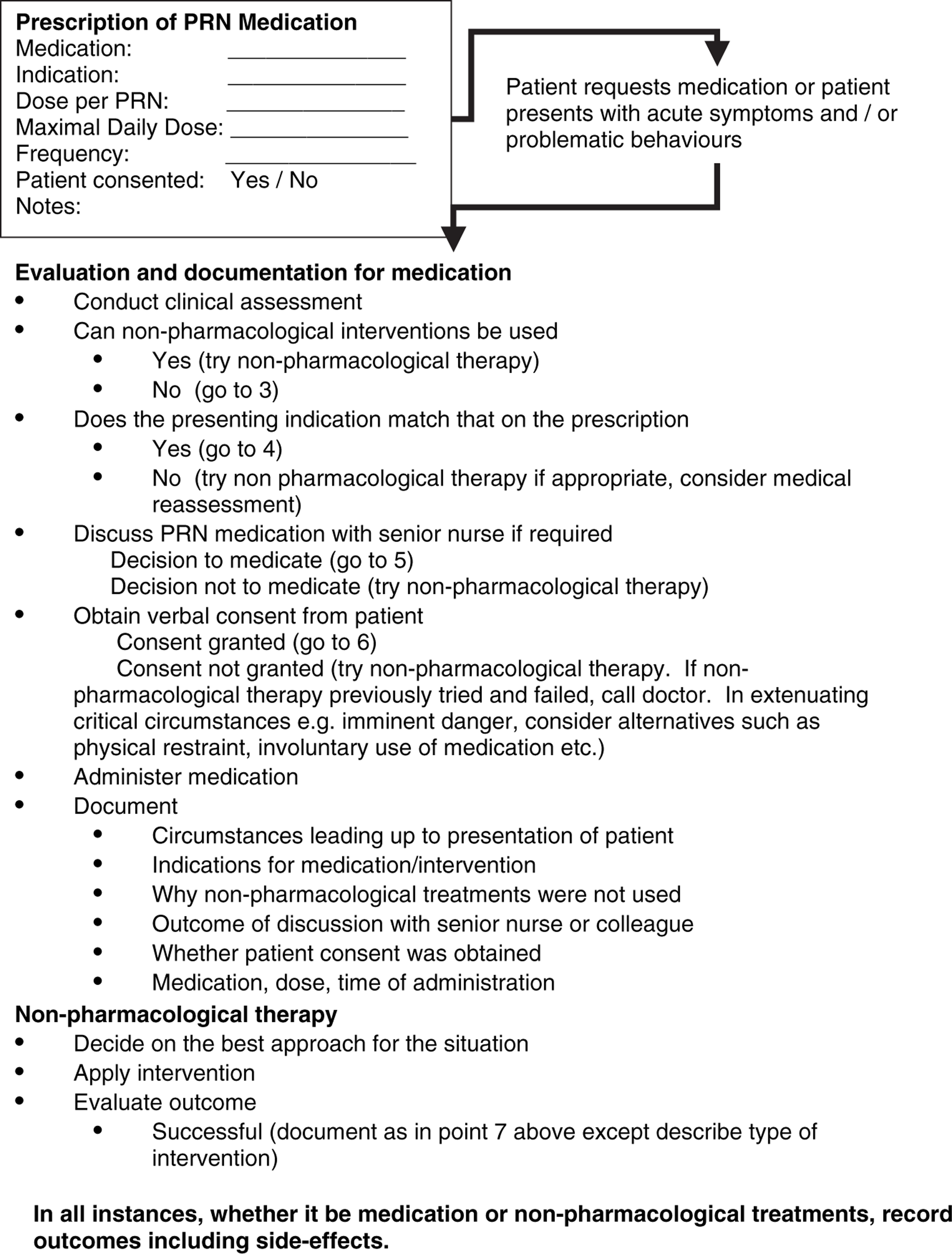
Psychological treatments are effective, have fewer side-effects than medication, and prepare the patient with coping skills for discharge [2]. It is ethical to consider the least restrictive and invasive treatment option available first. The Expert Consensus on Behavioural Emergencies in the US [35], Australian research [7], [34] and a literature review [18] agree that psychological (talking) therapies are the first line of treatment in an acutely symptomatic psychiatric inpatient. The astounding data that <7% of nursing time is dedicated to psychotherapeutic interventions [39], [40] reaffirms that the synergistic nurse–patient therapeutic interaction has been dramatically eroded. The development of standard PRN procedures may be a catalyst for change, but it will have to be supported by the cornerstone of adequate nursing resources and training.
The role that psychiatrists occupy in encouraging non-pharmacological interventions has been overlooked in all previous studies and reviews. When PRN prescriptions are written, the psychiatrist could prescribe a pragmatic approach in that non-pharmacological treatments are attempted prior to resorting to medication. It has been noted that some doctors, especially junior doctors, succumb to nurse pressure to prescribe PRN medications [17]. This suggests that more appropriate medical training is required with regards to psychotropic PRN administration.
One of the major problems with the administration of PRN medication is the apparent lack of obtaining of patient informed consent prior to medication administration [17], [30], [42]. Psychiatric patients have the ethical right to informed consent [25], [44], [45] and it is an Australian nursing and medical ethical code of practice to obtain informed consent prior to medication [27], [43]. Informed consent is not ‘I'm giving you this as you seem out of sorts’ but a discussion on the indications for use, the potential effects and side-effects of the medication and possible alternatives. One potential nursing objection to obtaining informed consent from a patient is the perception that the patient may refuse the medication. But the potential to refuse medication or treatments is a reason to obtain informed consent because refusal of treatment in an inherent right of the patient. There is no evidence to indicate whether obtaining informed consent or not results in more or less medication refusals. There is evidence to indicate that not obtaining informed consent increases patient dissatisfaction [30]. Figure 1 highlights that informed consent is required both on the prescription on the PRN medication(s) [27] and the administration by nursing staff [43]. Because informed consent is such an important human right, our suggestion is that it is annotated in the clinical record.
Clinical assessment of the benefits and side-effects of any prescribed medication is standard practice for psychiatrists and the general nursing profession. Psychiatric nursing practices typically do not record outcomes of PRN medication and almost never document side-effects [1], [3–7], [30]. To ensure the safety of the patient, and to inform future clinical decisions on medication prescription, nursing practices require an overhaul to guarantee that outcomes (including side-effects) of PRN medication are annotated.
The Australian Commission on Safety and Quality in Health Care, as well as various state and territory equivalents, are working to improve the safety and quality of health care in our hospitals. The Commission has, as one main focus, recommendations for inpatient medication [49], which are consistent with our recommendations. To ensure the safety and a high quality of care for psychiatric inpatients, standardized protocols for the administration of psychotropic PRN medication are essential. This is especially important because psychiatry is one of the very few areas in medicine where a patients’ right to consent to treatment can be overridden. This responsibility should not be undermined by poor professional practice. To operationalize the recommendations in this review, and facilitate adherence to agreed protocols, there should be a standard application of the recommendations in every inpatient mental health unit in Australia. Figure 1 provides an example of how these units could implement our recommendations.