
Abstract
Keywords
The available evidence about the use of ‘as needed’ (PRN; from the Latin pro re nata: for an occasion that has arisen) medications in acute inpatient mental health care settings units has remained consistent over a number of years. Recent investigations show that 63–82% of adult inpatients receive a PRN medication as part of their clinical management [1–6]. In earlier findings (with exception of Walker [7]) there was a slightly lower rate of administration, with reports of <51% of admitted patients receiving a PRN medication [8–11]. The evidence indicates that this practice remains a routine aspect of inpatient mental health care.
While the evidence indicates that PRN medication use in acute inpatient mental health care is routine, it is a practice based on clinical experience and expert/consensus guidelines rather than on high-quality evidence from controlled clinical trials [12]. The use of PRN medications is based on the clinical rationale that nursing staff need to be able to administer medications in a timely fashion when caring for distressed and aggressive patients, and that calling a doctor for a medication order could delay action, placing staff and patient safety under threat [10], [12]. But these fears about safety were not realized in one study that compared rates of PRN medication use before and after implementation of a policy that required a medical order for each PRN medication administration [4]. While the rate of PRN administration decreased significantly during the study period, there was no accompanying increase in physical aggression, or restraint and seclusion rates.
The investigations in the literature to date have relied on retrospective chart audits [1–11]. The audits indicate poor and inadequate prescribing practices for PRN medication in acute mental health care. For example, there was no indication for the drug in the PRN prescription, in as much as 84% of the time [2], [7], [9]. Bowden found poor compliance with British consensus guidelines; for example, i.m. and oral dosages were the same for a given drug and dosages were ranged, thus the nurse administering the medication determined the dosage [13]. More importantly from a patient safety perspective are reports that a higher than 1000 mg chlorpromazine equivalence per day was being prescribed when PRNs were added to the daily medication schedule [13], [14]. Although amounts greater than 1000 mg chlorpromazine equivalence may be safely administered in certain clinical circumstances, the concern is the potentially ‘hidden’ nature of the high dosages when PRNs are added routinely to regular medications.
In addition to inadequate prescribing practices, the findings of these studies show that nurses did not provide written documentation explaining why they administered a PRN medication in up to 41% of cases [1], [2], [5], [10]. Other studies reported a lack of documentation regarding the effects of the medication that occurred in up to 64% of the times a nurse administered a PRN medication [1–3], [5], [7].
Some investigators suggest that the standard use of PRN psychotropic medications is problematic. First, there is the potential risk of psychotropic polypharmacy, especially when PRN medications are a different class than those regularly prescribed [4]. The introduction of second-generation antipsychotics (SGAs) heralded the routine use of benzodiazepines (a different drug classification) as PRN medications. Currently it is standard practice to combine more than one drug type in acute mental health care [15] and this is consistent with current expert opinion and clinical guidelines in acute mental health care [16], [17]. Second, potential problems have been raised about this routine practice because the safe use of benzodiazepines in cases of alcohol and drug comorbidity, an increasing feature of mental health patient presentations, has been questioned [18].
The administration of psychotropic medication is based on the therapeutic principle that symptom reduction enables patients to engage in other therapeutic endeavours such as psychosocial recovery. Nonetheless, PRN medications are potentially restrictive, and therefore problematic, if they are used as a substitute for engaging patients in other therapeutic activities such as developing coping and life skills [18]. In a recent Australian study Thomas et al. reported a significant reduction in PRN use when an activities programme was introduced on a high-dependency mental health unit [19]. Years earlier, Craig and Braken speculated that higher rates of PRN usage were associated with units that had lower staff: patient ratio, suggesting that PRN medications could be used as an alternative to interpersonal engagement with patients [8].
This study was a chart audit of PRN medication use across four acute, inpatient mental health care units in public hospitals of metropolitan Sydney. The aim of the study was to provide a detailed description of the circumstances surrounding the use of PRN medications with particular focus on why nurses administered PRN medications and how they evaluated their effects. Uncovering the context of PRN medication use helps to explicate the knowledge that is embedded in this routine clinical practice. The affiliated university and each of the local hospitals’ human research ethics committees approved the investigation as minimal risk research.
Method
The health-care records of all patients admitted for >24 h during a 2 month period were reviewed. The audits were not limited to this time frame because the medication records for the entire admission were audited for these patients. The entire admission was audited even when it extended beyond this period. The 2 month time frame was selected in order to yield approximately 100 admissions for each site, thus making across-site comparisons reasonable and enabling collection of a data set large enough to conduct meaningful statistical analyses.
Admission data sheets, including initial clinical assessment, and discharge summary sheets were audited. For each patient the following demographic data were recorded: age, gender, country of birth, language spoken at home, and Indigenous Australian status. In addition to the demographic data, recorded clinical data included presenting problem and legal status on admission, primary medical diagnosis and coexisting illness at discharge, and length of hospital stay (LOS).
Medication records were reviewed for the prescribing information in relation to both regular and PRN medications. For regular medications the name of the medication, its dose, frequency and route of administration were recorded, as well as changes to any of these parameters. For each PRN prescription the drug name, dose, route of administration, indications for use and daily dosage limits were recorded.
Each patient record was then audited to identify each episode of a PRN medication administration and the following data were collected: (i) name, dosage and route of administration; (ii) initiator of the administration (clinician or patient); (iii) date and time of day; (iv) day of admission (in relation to LOS); and (v) documented ‘reasons for’ and ‘outcomes of’ PRN administration recorded.
All data were recorded using standardized audit tools developed for the study (available on request). Medications were grouped under the classifications first-generation antipsychotics (FGAs), SGAs, benzodiazepines, mood stabilizers, anticholinergics and injectables. All data were assigned codes, with the exception of ‘reasons for’ and ‘outcomes of’ a PRN administration. Initially these were recorded verbatim from clinical file notes then coded after the first 100 charts were audited.
The following codes were derived from the terminology used by nursing staff; ‘threatening behaviour, physical aggression’, ‘threatening behaviour, verbal aggression’, and ‘agitated’. The first code ‘threatening behaviour, physical aggression’ was designed to reflect chart entries such as ‘throwing objects’, ‘punching’, ‘fighting’ and ‘kicking’. This code was differentiated from ‘threatening behaviour, verbal aggression’, which represented entries into the patient records such as ‘shouting’, ‘screaming’, ‘yelling’, ‘demanding’, and ‘verbally abusive’. The term ‘agitated’ consistently appeared across all patient records, and thus became a code. This code encompassed other terms used by nursing staff that indicated agitation; these included, ‘restless’, ‘unsettled’, ‘edgy’, and ‘unable to calm down’. The initial codes were included in the audit tool and used for the remainder of the data collection. At final analysis these codes were collapsed into categories for the purpose of reporting only.
Codes for the documented ‘outcomes of’ PRN administrations also were based on actual terms used by nurses in chart entries. These terms were more standardized than those of ‘reasons for’ administration and included terms such as ‘effective’ and ‘settling’. When the chart entry immediately after the administration of a PRN medication stated that the patient was ‘asleep’, this was recorded as an outcome even if not directly linked to the PRN administration in the documentation.
All data were entered into SPSS, version 14 (SPSS, Chicago, IL, USA). Tests for differences (ANOVA for differences between means, and χ2 tests for categorical data) between the four hospitals were performed. There were no significant differences between the hospitals on age of patient, length of stay or on primary diagnosis, but significant differences were found in the gender of the patients (p = 0.025). One site had a higher proportion of male patients (69.3% compared to 54% for the other three hospitals combined). The frequency of PRN administrations also did not vary significantly across sites. As a result, data for all four hospitals were combined.
Results
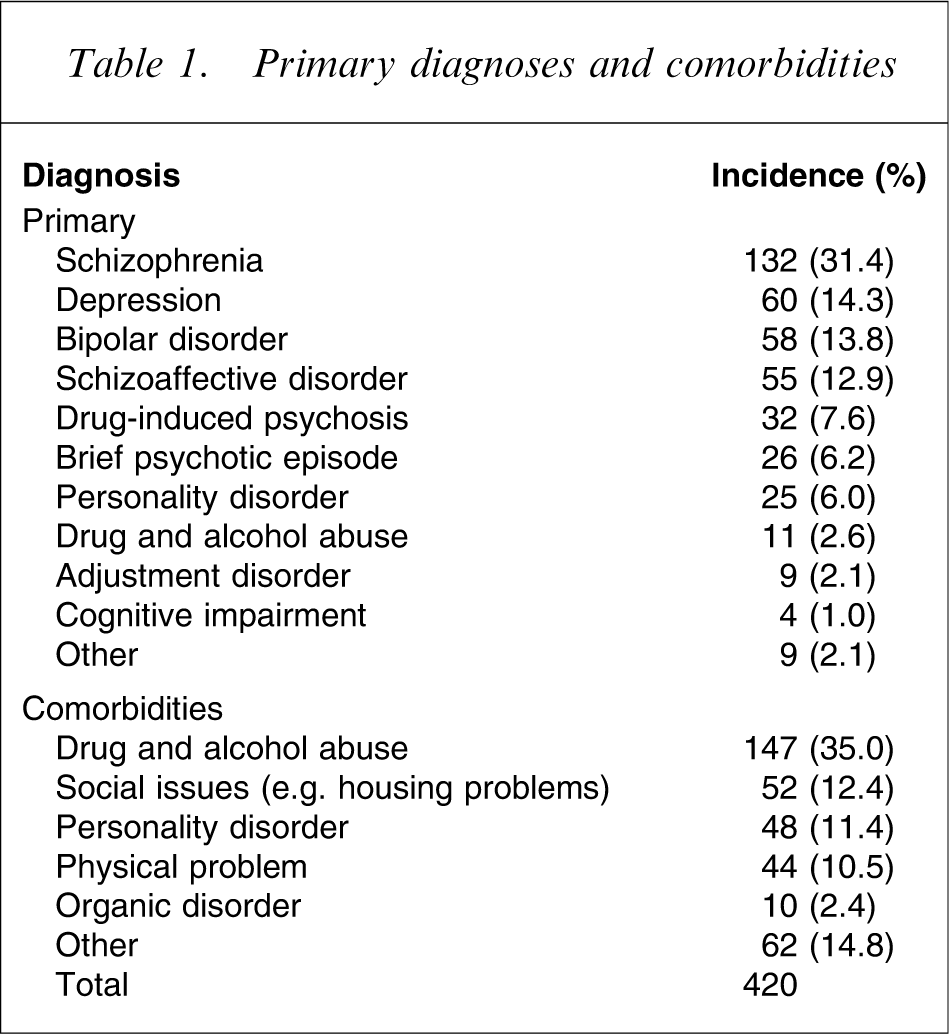
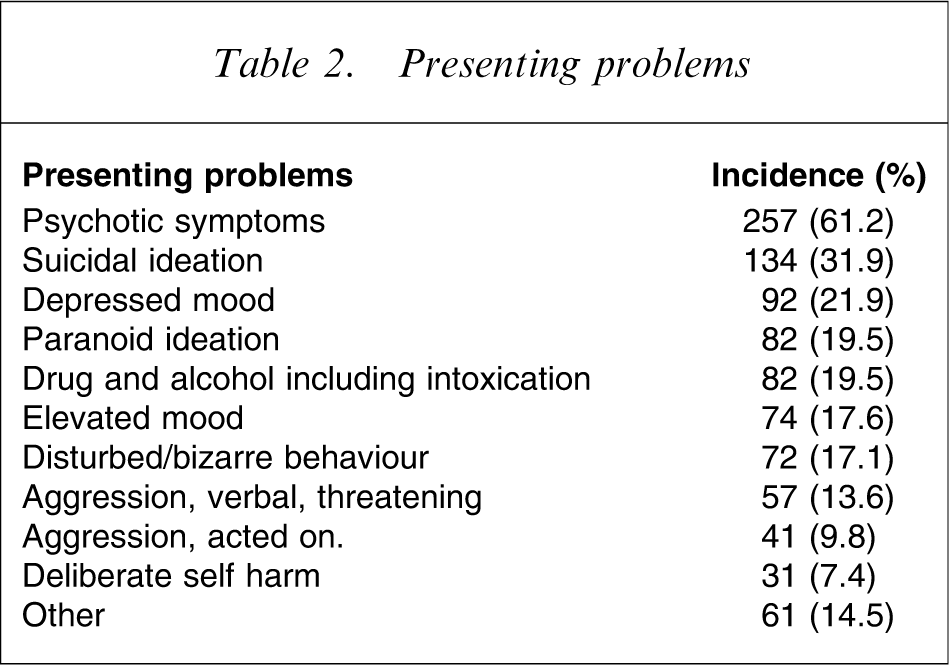
A total of 420 records were audited. In the sample population there were 57.6% male, 42.4% female, with an average age of 38.63 years (range = 16–83 years) and an average length of stay of 20.45 days (range = 1–270 days). Primary diagnoses, comorbidities and presenting problems showing number and percent of patients in each category are found in Tables 1 and 2.
Primary diagnoses and comorbidities
Presenting problems
For the four hospitals combined, 55 of the admissions (13.1%) were for patients with no fixed abode, and 334 (79.5%) of the admissions were involuntary. The reported prevalence of a drug and alcohol-related comorbidity was 35.0%, and is higher than the 26.6% reported in the most recent Australian study for which this detail is reported [2].
At least one PRN medication was administered to 83.8% of all admitted patients. Although the percentage of admitted patients receiving a PRN was slightly higher at one site, this was not statistically significant. The administration of PRN medications did not vary significantly with gender, legal status or age, therefore data from all sites were combined for analysis.
Prescription medication
Prescription of regular medications
All but 26 of the 420 admitted patients, that is, 93.8%, were prescribed regular medications. Of the 1106 prescriptions recorded, 34.8% were written for SGAs, with olanzapine accounting for 17.5%. This contrasts with 5% of prescriptions for FGAs. The second highest rate of prescription medications was the benzodiazepines at 22.6%, with diazepam accounting for 18.2% of the total prescribed regular prescriptions. This was followed by mood stabilizers (anti-mania), prescribed at a rate of 16.3%, and antidepressants at 14.9%. The anticholinergic medication, benztropine, accounted for 1.8% of the prescriptions.
Prescription of PRN medications
Ninety-seven per cent of the patients (408/420) were prescribed PRN medications, with a total of 1398 PRN prescriptions written during the study period. The most frequently prescribed medications for use as a PRN were benzodiazepines, with diazepam and midazolam representing 29.6% and 21.6%, respectively, of all prescriptions written. The third most frequently prescribed PRN medications were the FGAs, representing 16.6% of the total PRN prescriptions written.
Episodes of PRN administrations
For the 420 admissions there was a total of 3868 episodes of PRN medications administered during the study period.
PRNs and diagnosis
Figure 1 shows a box plot of total PRNs per day for each diagnosis. An ANOVA was carried out using Tukey post-hoc tests to determine any significant differences between different diagnoses. Total PRNs per day was significantly higher for patients diagnosed with a personality disorder than for those experiencing depression, brief psychotic episode, schizophrenia and schizoaffective disorder. Total PRNs per day was also significantly higher for patients with drug and alcohol abuse than for those with depression, brief psychotic episode and schizophrenia. The other differences were not significant. There are, however, a number of outliers in most groups.
PRNs day−1 by diagnosis. PRN, pro re nata (for an occasion that has arisen; as needed).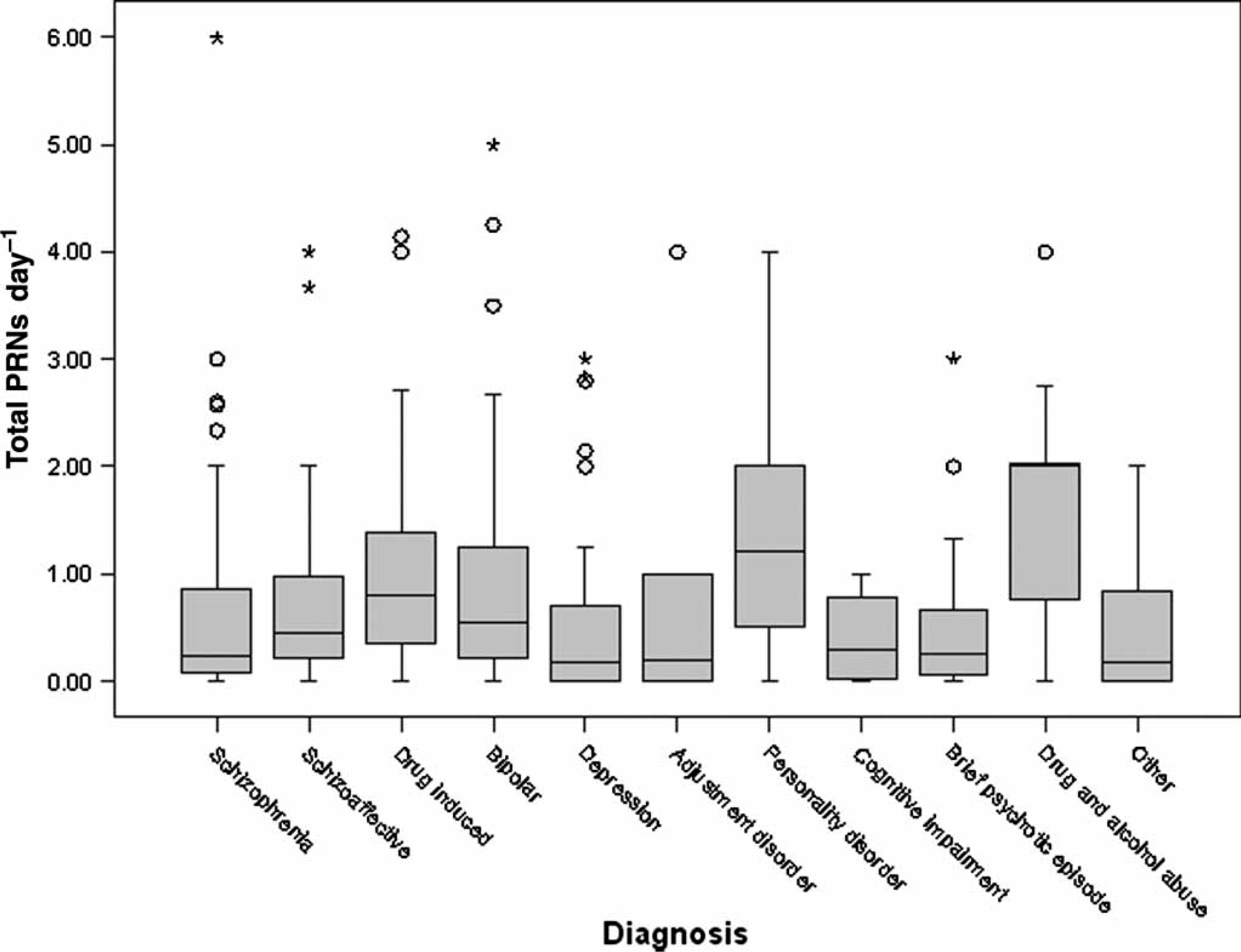
Types of PRN medications
The most frequently administered PRN medications were benzodiazepines (70.7%), with diazepam accounting for 53.5% of the total administrations. The next most frequently administered PRN medications were FGAs (18.1%), followed by benztropine (4.3%).
Documented reason for PRN administration
There was a documented reason for a PRN medication in 63.2% of all administrations. The reasons are categorized in Table 3 and are reported in relation to the classification of the medication administered.
Stated reason in relation to type of medication administered
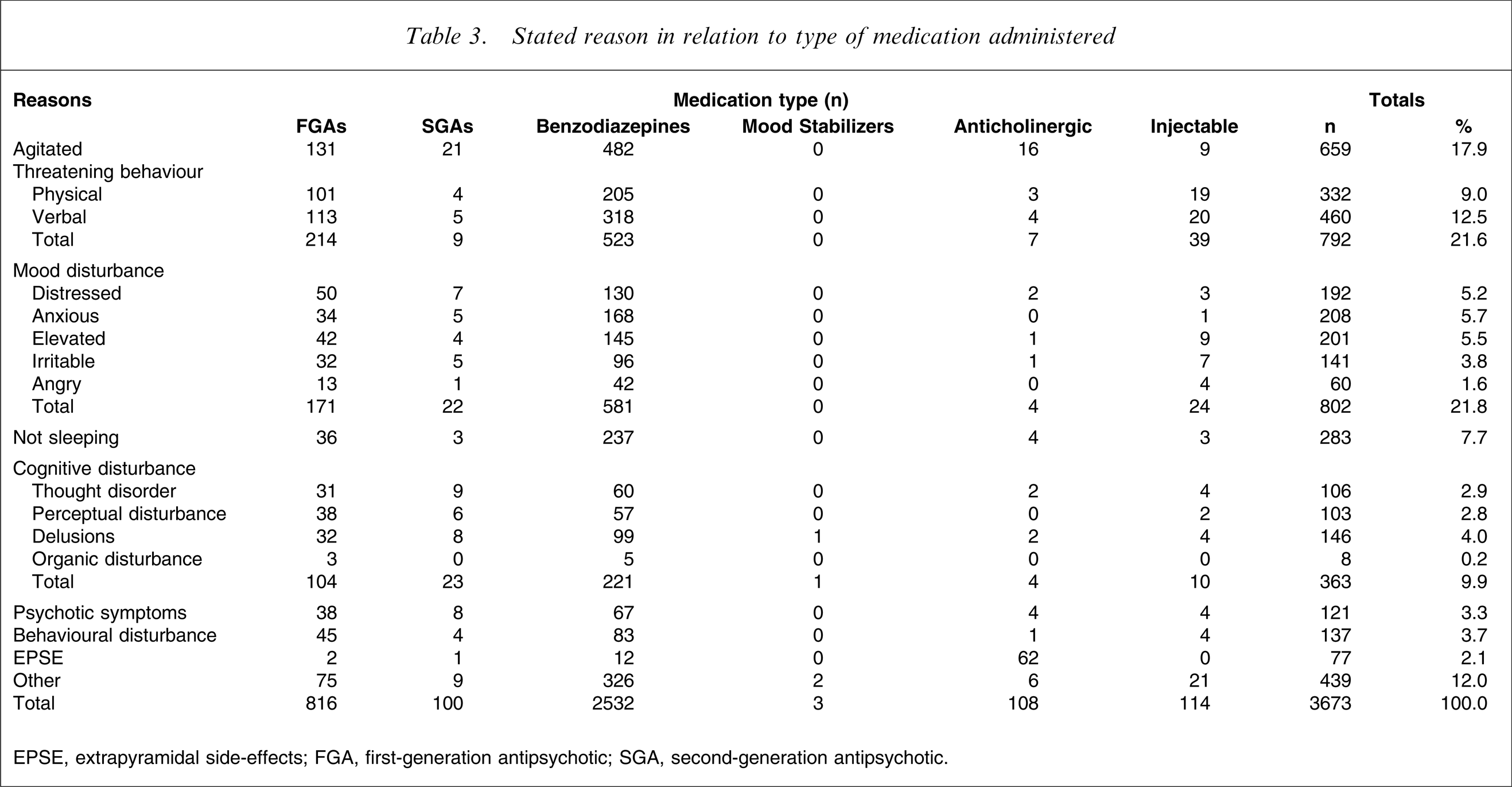
EPSE, extrapyramidal side-effects; FGA, first-generation antipsychotic; SGA, second-generation antipsychotic.
Some of the medication administrations involved more than one medication and the reason recorded may not be specific to that medication. For example, when a typical antipsychotic was administered with prophylactic benztropine, then the reason recorded could simply be psychotic symptoms, thereby giving the impression that benztropine was administered for that reason. Nevertheless, Table 3 indicates the possibility that medications were administered for reasons other than correct indications.
Initiation of the PRN
The PRN medication administration was initiated by staff 60.7% of the time and by patients 10.8% of the time. There was no written indication of who initiated the medication in 28.5% of the PRN administration episodes.
Time of day
The highest percentage of PRN medication administrations occurred during 20:00 and 23:59 hours (32.3%). A further 17.7% of the PRN medication administrations occurred between 16:00 and 19:59 hours. Thus, the majority of PRN medications were given during evening and bedtime hours. Approximately 31% of the PRNs were given during the day, between 08:00 and 16:00 hours. Only 5% of PRN medications were given between 04:00 and 07:59 hours.
Documented outcome of PRN administrations
In nearly half of PRN medications that were given there was no documentation of an outcome, that is, there was no further record of the medication after administration. Of the PRN episodes when an outcome was recorded, 48.6% noted that the medication was ‘effective’. The medication was recorded as ‘not effective’ in 17.6% of these cases and ‘patient asleep’ was noted in 31.2% of the documented outcomes. The records also indicated that patients were secluded in 7.3% of the episodes in which there was chart entry related to PRN outcome.
Patients who received numerous PRN medications
Within the group of patients who received PRN medications there was a small subset of patients (n = 18) who received >40 administrations of PRN medication during their admission. This subgroup, which comprised <5% of all admitted patients, received approximately one-third of all PRN administrations. Their characteristics can be found in Table 4.
Patients who received >40 PRNs
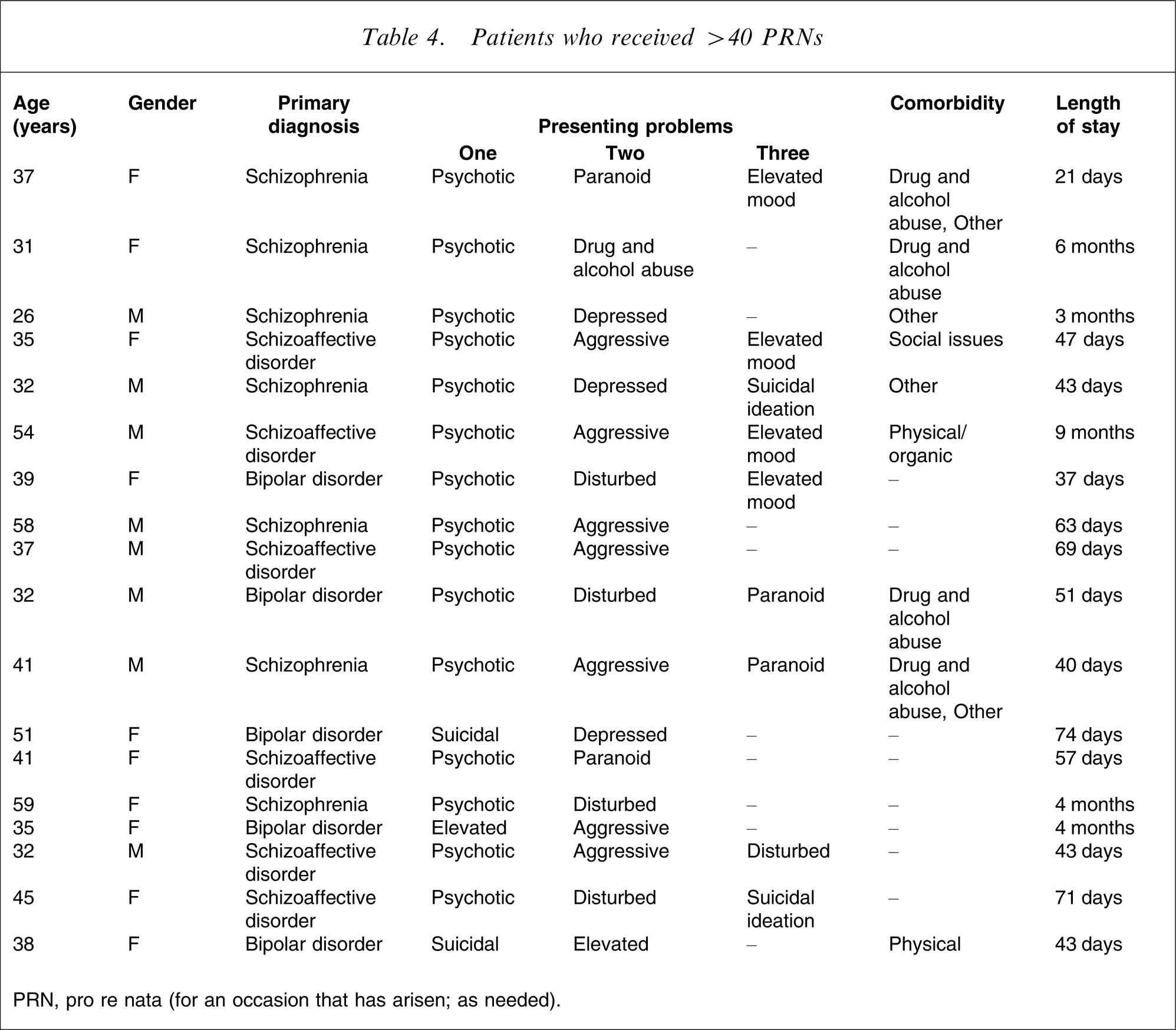
PRN, pro re nata (for an occasion that has arisen; as needed).
Of the 18 members of the >40 PRNs group, eight were male and 10 were female. The age distribution of the >40 PRNs group was more compact than that for the others. The age range for admissions overall was 16–83 years, but the 18 people in the >40 PRNs admissions ranged in age from 26 to 59 years.
The diagnosis of schizophrenia and schizoaffective disorder accounted for approximately two-thirds of these patients in this subgroup. As can be seen in Table 5 the initial diagnosis for the 18 >40 PRNs group was schizophrenia (seven patients), schizoaffective disorder (six patients) or bipolar disorder (five patients).
Primary diagnosis of patients who received >40 PRNs
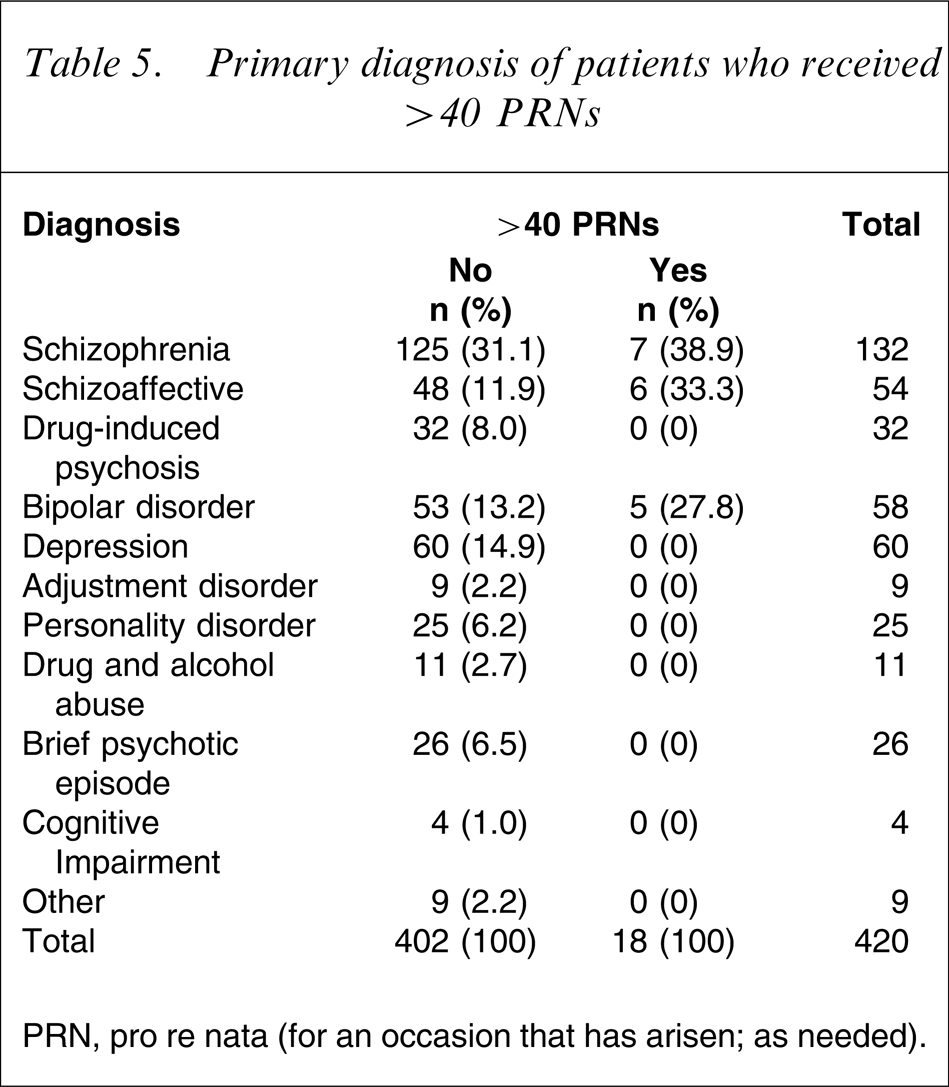
PRN, pro re nata (for an occasion that has arisen; as needed).
More than one-third of these patients had presenting behaviour on admission that was described as aggression (36%), and another 30% had a presenting problem documented as ‘elevated mood’.
The >40 PRNs group was more likely to present with psychotic symptoms (83.3% of this group compared with 57.6% of the rest), paranoid ideation, elevated mood, disturbed/bizarre behaviour and physical aggression (Table 6).
Presenting problems for >40 PRNs group
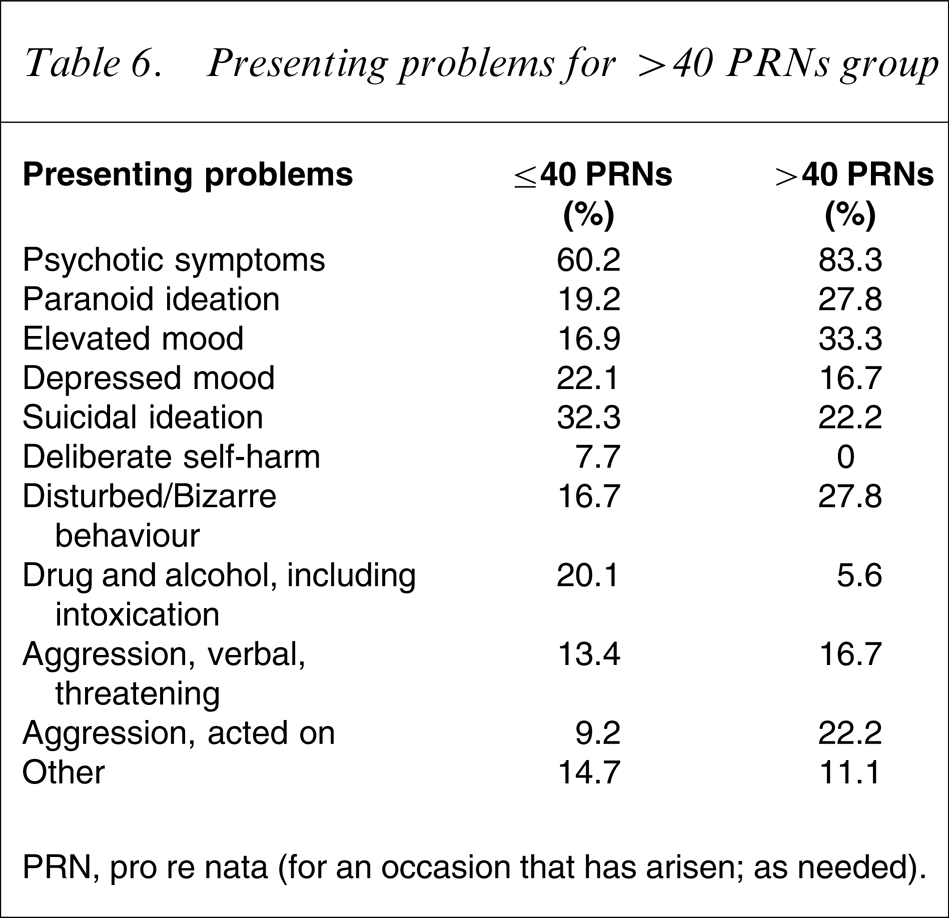
PRN, pro re nata (for an occasion that has arisen; as needed).
Their LOS was much longer than the average LOS for other patients admitted during the time frame, but the relationship between LOS and number of PRN administrations was not clear-cut. There was a positive correlation of 0.495 between LOS and total number of PRN administrations, indicating as expected a positive relationship between the two. Mean LOS for the >40 PRNs group was 83.11 days compared with 17.65 days for the rest, but there was a lot of overlap. LOS for the <40 PRNs group ranged from 1 to 270 days and for the >40 PRNs group, from 37 to 267 days.
Discussion
As in the present study, the most commonly reported singular reason for administration of PRN medications in acute mental health setting continues to be patient agitation [1–3], [7–9]. Three other studies in which the most frequent reason was reported have noted different results [5], [11], [14], with patient request, distress and insomnia being the most commonly stated reasons.
In the present audit, as in other studies, there was little descriptive evidence of what nurses meant when they used the term ‘agitation’ in their documentation. Established guidelines suggest that agitation not be used as a reason when prescribing PRN medication because of the difficult differentiation between agitation and akathisia [4], a potential side-effect of psychotropic medications. Without descriptive evidence, it is unclear whether nurses who administered the medications attempted to or actually made this differentiation. It is unclear as to whether nurses in the present study considered akathisia as a possible reason for what was described as patient agitation. That is, the motor restlessness that accompanies agitation could be due to psychotropic medication.
The documentation regarding the ‘reasons for administration’ audited in the present study were slightly more complete than the documentation used in previous studies [1], [2], [5], [10]. It is encouraging to note that documentation regarding the ‘outcome of administration’ was recorded in significantly more of the patient records audited in the present study, than in prior studies [1–3], [5], [7].
Benzodiazepines were the most commonly administered class of drugs as PRNs in the present study, as is the case in most other studies [1], [3], [5], [10], [20]. The exception to this is Geffen et al., who reported that the FGA, haloperidol, was the most frequently administered PRN [2]. Other exceptions were reported in earlier studies that were conducted before the widespread use of SGAs. For example, Gray et al. found that the most commonly given PRN was an anticholinergic [20]; and Walker reported that FGAs were most frequently given [7]. In the earliest study Craven et al. reported sedative-hypnotics, such as chloral hydrate, as the most frequently administered PRN [9].
The most common time for a PRN medication to be administered, between 20:00 and 24:00 hours, is the same as in all other studies in which time of day of PRN medication administration was reported [1], [5], [9], [10], [14]. This time of day is consistent with settling people at bedtime, because sleep disturbances are often present in acute mental illness. Insomnia, however, was documented as a reason for PRN medication administration in only 8.1% of all PRNs given.
The present study shows that in the majority of PRN administrations were initiated by nurses rather than patients, an outcome that closely reflects the findings of two of the four previous studies that reported this aspect [1], [11]. Usher et al. found nurse-initiated and patient-initiated to be almost equal, and that insomnia, not agitation, was the most common reason for PRN administration [5]. There was a much higher percentage of voluntary patients in the Usher et al. study, and this could account for the higher frequency of patient request for medication. Milton et al. found that patient ‘request’ was the most common reason why a PRN was administered and that anticholinergics were the most commonly given medication [14].
The small subset of patients (n = 18) who received more than 40 PRNs in their admission, received approximately 30% of all PRNs; this is noteworthy. Similar results were reported in the Thapa et al. study, with <10% of the patients receiving approximately 50% of all PRN medications in that study [4]; in the McKenzie et al. study, in which 3.6% of patients received 9.9% of all PRNs [3]; and in the Craig and Braken study, in which 2.4% received 44.2% of the PRNs [8]. In all likelihood the sheer volume of PRN administrations reported in the present study (n = 3000 +) enabled the identification of this subset. For example Thapa et al. reported on 2788 administrations [4] while other studies, such as the Curtis and Capp study, reported on only 450 administrations [1].
The profile of patients who received a large number of PRN medications reveals some interesting findings. First, there were more female than male patients in the present population. In addition, they were more likely to be psychotic, paranoid, and experiencing an elevated mood. Also, their presenting behaviour was more likely to be described as bizarre and disturbed. This profile may indicate a group of patients for whom much care should be taken when prescribing regular medications because the high frequency of PRN use could indicate a failure of regular medications in controlling symptoms.
Limitations
Like many previous studies [1–11], the present study used retrospective audit methods and the limitations of such a design cannot be overlooked. The major limitation in a study such as this is the reliance on documentation, which is often inadequate and lacking. Not only are records lacking in details about PRN medication administration, but there is no way of ascertaining what other strategies besides PRNs were attempted.
Caution should be exercised when comparing the present findings with those of past studies because the documented sample sizes were small, the studies were conducted using different methodologies, and the clinical context may have been different. For example, unlike the present study, in which 79.6% of patients were admitted involuntarily, 70% of patients in the Usher et al. study were voluntary [5]. Other differences elucidated in the current findings compared to those of past studies, such as the Milton et al. study [14], may reflect not only the evolving nature of psychopharmacology, especially the introduction of SGAs in the early 1990s, but also differences in local prescribing practices.
Conclusions
Administration of PRN medication is a clinical practice in which nurses and doctors function interdependently. Doctors prescribe PRN medications and nurses make the final decision as to the circumstances that warrant their administration. Both doctors and nurses in the Geffen et al. study demonstrated less than adequate clinical knowledge required for such decision-making [21]. Although there are descriptive studies of the practice of PRN medication use, there is little evidence to indicate the knowledge that doctors and nurses use to make decisions about the use of PRN medications.
The present study highlights the circumstances surrounding the use of PRN medications, with particular interest in the reasons ascribed by nurses for administration, and the subsequent evaluation of the administration effectiveness. As reported in many previous studies, documentation in patient notes is either missing or incomplete [1–5], [7], [10].
The use of benzodiazepines as the most commonly administered PRN medications reflects the nature of current practice in the use of SGAs. Indeed, practice guideline recommendations include the use of SGAs in conjunction with benzodiazepines for management of acute psychotic conditions, with the latter being recommended for sedating and anxiolytic effects [17], [22].
A unique contribution of this research was the isolation of a small subset of patients (5%) who accounted for a large portion of the PRN medication administrations. The volume of PRN administration episodes (3000 +) is the largest reported in the literature and this enabled the identification and description of this subset. While there have been reports of a small percentage of patients being overrepresented in the PRN medication administrations in other studies [3], [4], [8], these patients have not been fully described. Further investigation of this group is important because the demographics and diagnoses representing this group appear markedly different from those of patients who received less PRN medication.