
Abstract
Patients diagnosed with borderline personality disorder (BPD) are major users of mental health services and emergency medicine. With mortality rates as high as 10%, there is clearly room for improvement in the clinical management of this patient group [1]. The clinical challenge in providing adequate management is often derived from the confronting and pervasive patterns of behaviour that affect the way these patients relate interpersonally. Impulsivity, issues with abandonment, poor self-image, and feelings of emptiness, all contribute to the self-harming behaviours, and difficulties observed in treatment planning and provision. As such, working with patients with BPD involves well-acknowledged challenges, not the least of which is that attempts to prevent further self-injury or overdose can appear ineffectual in the context of recurrent self-harming behaviour.
As a result there has been an increasing focus in examining the way that health professionals relate to this patient group. According to the research, attitudes of professionals towards patients diagnosed with BPD tend to be negative and derogatory [2–4]. The self-harming actions tend to be managed with behavioural techniques, such as seclusion and restraint, or diversion and distraction. This can be ineffective when the patient's reasoning behind their self-harming behaviour is not investigated; due to their diagnostic label and frequent presentations, their compulsions to continue to self-harm are frequently misunderstood [4]. The pessimistic attitudes and reactive behavioural management strategies then act as a major barrier to effective service provision for this group of patients [2], [4], [5]. Whether these attitudes may be directly demonstrated or covertly disguised, patients may sense derogatory attitudes through the clinician's demeanour and manner [3], which may prompt further self-harm and suicidal behaviour [5].
The impediment to effective clinical interventions derived from negative professional attitudes has been well documented in studies [6–8]. Johnstone found that once a diagnosis of BPD is made, inquiry tends to cease and staff see the disorder rather than the person with the disorder, resulting in a failure to explore the reasons behind the patient's self-harm [6]. Alston and Robinson also found that clinicians held negative attitudes towards self-harming patients and, when faced with such patients, the clinicians experienced a multitude of mixed emotions causing them distress and inner conflict, which disposed them towards an absence of empathy, regardless of the need for therapeutic understanding [7]. This was further supported by Vivekananda and even extended to general public opinion, including families and carers of patients who self-harm, who often experienced shame when their loved one self-harmed [8].
In a study conducted specifically with mental health staff in the UK in 2000, 75% of such staff reported that self-harming behaviour in their patients was difficult to manage and 65% of the sample also reported that they found it difficult to build a relationship with clients who self-harm [9]. Similarly, Boyes reported that emergency medicine staff report frustration at their inability to cure the patient, because they often re-present with similar injuries despite recent medical treatment for their self-harming behaviours [10].
To date few of these studies have drawn comparisons of professional attitudes between mental health and emergency department settings and few studies have investigated attitudes of different professions [3]. Although it would be reasonable to expect that clinicians within the mental health setting would have more positive attitudes towards working with BPD patients who self-harm, findings remain equivocal. Platt and Salter, for instance, found that when compared with psychiatrists, nurses in emergency medicine were more likely to view overdose as ‘attention seeking’ behaviour [11]. Anderson, however found no differences in attitudes when comparing a sample of nursing staff in a community mental health setting to those in an emergency department [12].
Education regarding patients with BPD has been shown to have a significant effect on the type of professional attitudes towards working with BPD. Krawitz found that after training on BPD was conducted over a 2 day period, clinicians displayed increased optimism, enthusiasm and positive feeling towards working with BPD patients, which was maintained at 3–5 month follow-up [13]. Further assessment of attitudes using a larger representative sample of clinicians from public mental health and substance abuse services also supported an increase in confidence in working with BPD following specific training in the area [14].
The current study compared the attitudes of different professional groups to working with BPD patients who self-harm. It was hypothesized that the clinician's gender, primary occupation and service setting, level of university training and years of experience, frequency of clinical contact, and completion of specific training in BPD would influence the reported attitudes of health professionals towards working with BPD patients who engage in self-harm. It was expected that mental health clinicians would report more positive attitudes compared to emergency medicine, with higher levels of clinical experience and university training, greater frequency of clinical contact, and completion of specific training in BPD also expected to influence more positive attitudes to this patient group.
Methods
Participants
The participants in this study were 140 registered health practitioners across two Australian health services, Ballarat Health Services (n = 52) and Barwon Health (n = 32), and a New Zealand health service, Nelson Marlborough District Health Board (n = 56). Mental health and emergency department staff of these health services were asked to participate if in the course of their employment they encountered patients diagnosed with BPD, with the rate of participation being approximately 61% of clinicians approached at departments within Ballarat Health Services, 14% of clinicians approached at departments within Barwon Health, and 43% of clinicians approached at departments within Nelson Marlborough District Health Board. All participants were eligible for participation in the current study if they were a registered health practitioner and no exclusion criteria were used.
Materials
Participants were provided with a purpose-designed demographic questionnaire. No identifying information was collected. Participants were asked to indicate their gender, years of experience, education completed, primary occupation, service setting, and average clinical contact with BPD patients. The participants also completed the Attitudes Towards Deliberate Self-Harm Questionnaire (ADSHQ) [3], which consists of 33 items on a 4-point Likert scale, ranging from 1 = strongly disagree to 4 = strongly agree, and in order to reduce response bias, one-third of items are phrased in the negative direction and no neutral response is allocated. All statements must be responded to with an indication of agree or disagree. The range of possible scores on the ADSHQ is 33–132, with higher scores reflecting more positive attitudes. Sample items are: Dealing with self-harm patients is a waste of the health-care professional's time; I deal effectively with deliberate self-harm patients; Self-harm patients just clog up the system. The ADSHQ consists of four factors that reflect a person's attitude towards deliberate self-harm (DSH) patients: perceived confidence in assessment and referral of DSH patients; ability to deal effectively with DSH patients; use of an empathetic approach; and hospital regulations that guide practice. McAllister et al. report reliability of the ADHSQ using Cronbach's α for each of these four dimensions as 0.71, 0.74, 0.67, and 0.57, respectively [3].
Procedure
Following consultation with management staff, and completion of the requirements for ethical approval at the three health services, participants were provided with an explanatory statement and a consent form that was signed prior to their participation. Participants were provided with the demographic questionnaire (gender, years of experience, education completed, primary occupation, and average clinical contact with BPD patients) and were given the ADSHQ [3]. All participants were requested to consider their responses on the ADSHQ in relation to their contacts with DSH patients diagnosed with BPD only. Responses and completed demographic questionnaires were then returned in a sealed envelope, separate from the completed consent forms. Approximately one-third of the questionnaires were distributed via mail, particularly to those staff who were employed in outlying areas, with a response rate of 89.4%. The majority were distributed to staff at their routine clinical meetings or staff development sessions, where they were collected immediately following completion. A total of 92.3% of clinicians at the staff meetings and development sessions completed the questionnaire.
Results
Statistical analysis was performed using SPSS, version 9.0 (SPSS, Chicago, IL, USA). Examination of the initial dataset indicated a normal distribution and acceptable levels of skew and kurtosis for all variables. No cases required deleting where data were missing.
The cohort of participants in this study included 48 men and 92 women, with 64.3% (n = 90) of the sample working within the mental health component of the health service; the remaining participants were employed in the department of emergency medicine. The primary field of occupation of the participants was 69.3% (n = 97) in nursing (including both general and mental health registration), 17.1% (n = 24) in allied health (including psychology, social work, and occupational therapy), and 13.6% (n = 19) in the medical field (medical or psychiatric registrars and officers, or psychiatrists). A total of 32.1% (n = 45) recorded between 0 and 5 years of clinical experience, and 30.7% (n = 43) reported having clinical experience of ≥16 years. In terms of level of education completed, 36.4% (n = 51) had completed undergraduate degrees, 48.6% (n = 68) had completed further postgraduate qualification such as graduate diplomas; the remaining 15.0% of participants (n = 21) had completed hospital training only.
In terms of specific training in BPD, 47.1% (n = 66) reported attending such training. Participants were also asked to record the average clinical contact that they have with patients diagnosed with BPD and reported daily (26.4%, n = 37), weekly (43.6%, n = 61), fortnightly (11.4%, n = 16), monthly or longer (18.6%, n = 26) frequency of contact.
The mean scores and standard deviations on the ADSHQ for the sample are presented in Table 1 according to comparison groups of service setting, gender of clinician, frequency of contact, level of university training, years of clinical experience, completion of prior training in BPD, and area of occupation. Analysis of these mean differences found that mental health clinicians had a significantly more positive attitude score towards BPD patients who engage in DSH compared to clinicians working in emergency medicine. There was also a significant difference between the ADSHQ score for male and female clinicians, with female staff reporting a more positive attitude towards the patient group. As predicted, clinicians across the mental health and emergency department service settings who had attended prior training specifically in the area of BPD demonstrated significantly more positive attitudes towards working with this patient group (t(139) = − 3.01, p = 0.003).
Clinician attitudes to self-harm (n = 140)
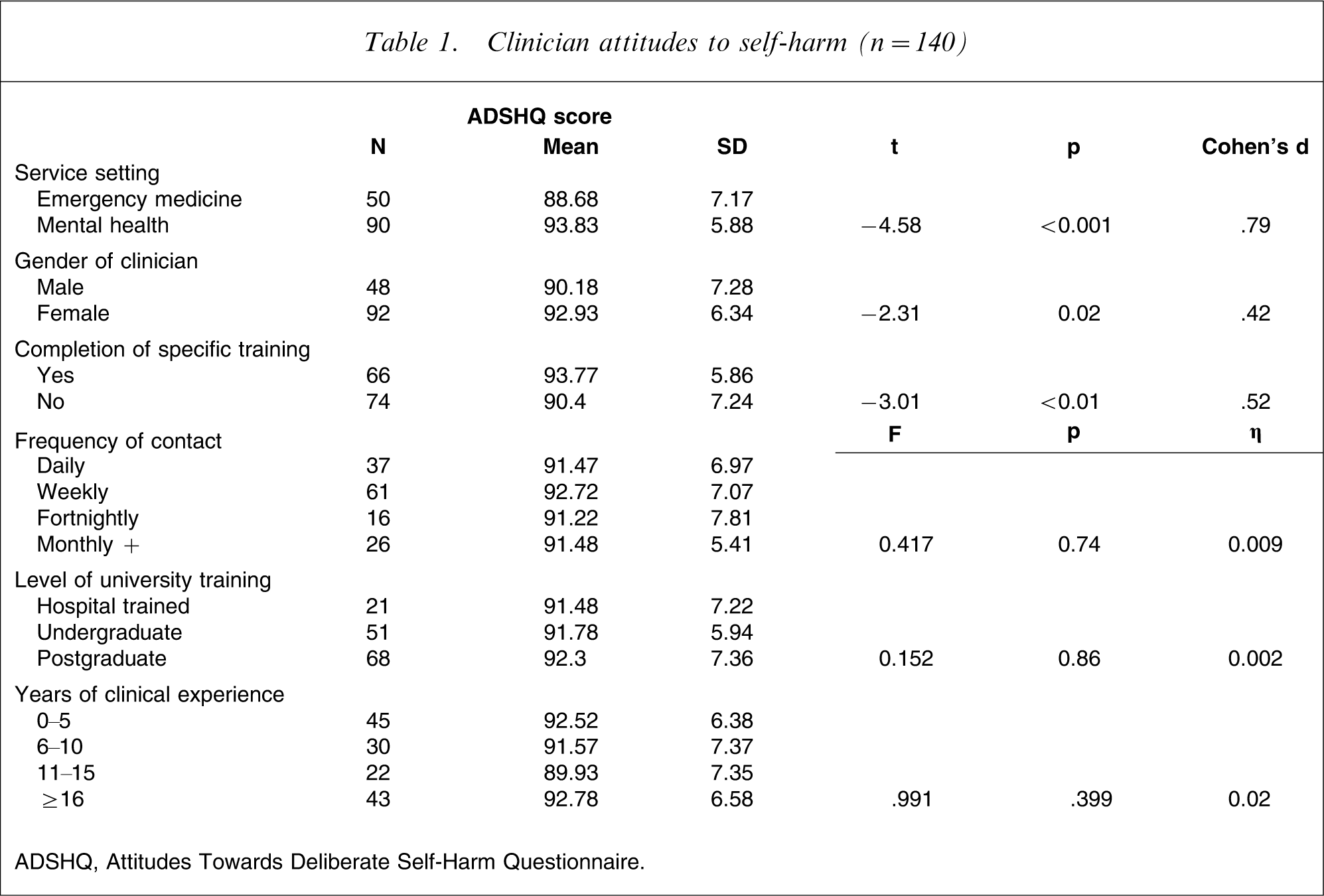
ADSHQ, Attitudes Towards Deliberate Self-Harm Questionnaire.
Upon examination of the frequency of contact with patients diagnosed with BPD, there were very small and not statistically significant differences between the ADSHQ scores (F(3,136) = 0.417, p = 0.741, η2=0.01); clinicians who had contact on a daily basis with such patients had similar attitude ratings to those clinicians who experienced contact on a monthly or longer basis. There were very small and not statistically significant differences observed in attitude ratings for participants who had completed hospital-based training, undergraduate study, or further postgraduate study (F(3,136) = 0.152, p = 0.86, η2=0.002). Furthermore, there were no significant differences on the ADSHQ scores according to years of clinical experience, with clinicians across the four time periods of 0–5 years, 6–10 years, 11–15 years, and ≥16 years experience recording similar attitude ratings towards borderline patients presenting with DSH (F(3,136) = 0.991, p = 0.399, η2=0.02).
A review of mean ADSHQ scores for participants from the three occupation areas of nursing, allied health and medical fields, indicated a significant difference between the attitude ratings recorded (F(3,136) = 3.29, p = 0.04). Upon closer examination, clinicians registered as allied health professionals demonstrated significantly higher attitude ratings towards patients with BPD than the other two occupation areas: nursing (t(119) = −2.47, p = 0.015) and medical (t(41) = 2.04, p = 0.048). There was no significant difference between the attitude ratings of nursing and medical staff (t(114) = 0.48, p = 0.63).
Following a review of these results, further statistical analyses were completed to determine if attitude scores changed across areas of primary occupation according to the completion of prior training in BPD. The mean scores and standard deviations on the ADSHQ for the participant groups are presented in Table 2. Interestingly, there was a significantly higher attitude score among the nursing participants who had received training (t(95) = 2.70, p = 0.008) with a medium effect size (Cohen's d = 0.55). When combining the results for all medical staff, it was apparent that they too showed an improved attitude following training (t(17) = 2.06, p = 0.05) with a larger effect (Cohen's d = 1.17). The same comparisons, however, made among the combined group of allied health clinicians showed that attendance at training on BPD had no significant effect on the clinician's attitude towards working with this client group, compared to other allied health clinicians who had not attended targeted education (t(22) = 0.16, p = 0.87).
Attitudes to self-harm by professional group versus specific training (n = 140)
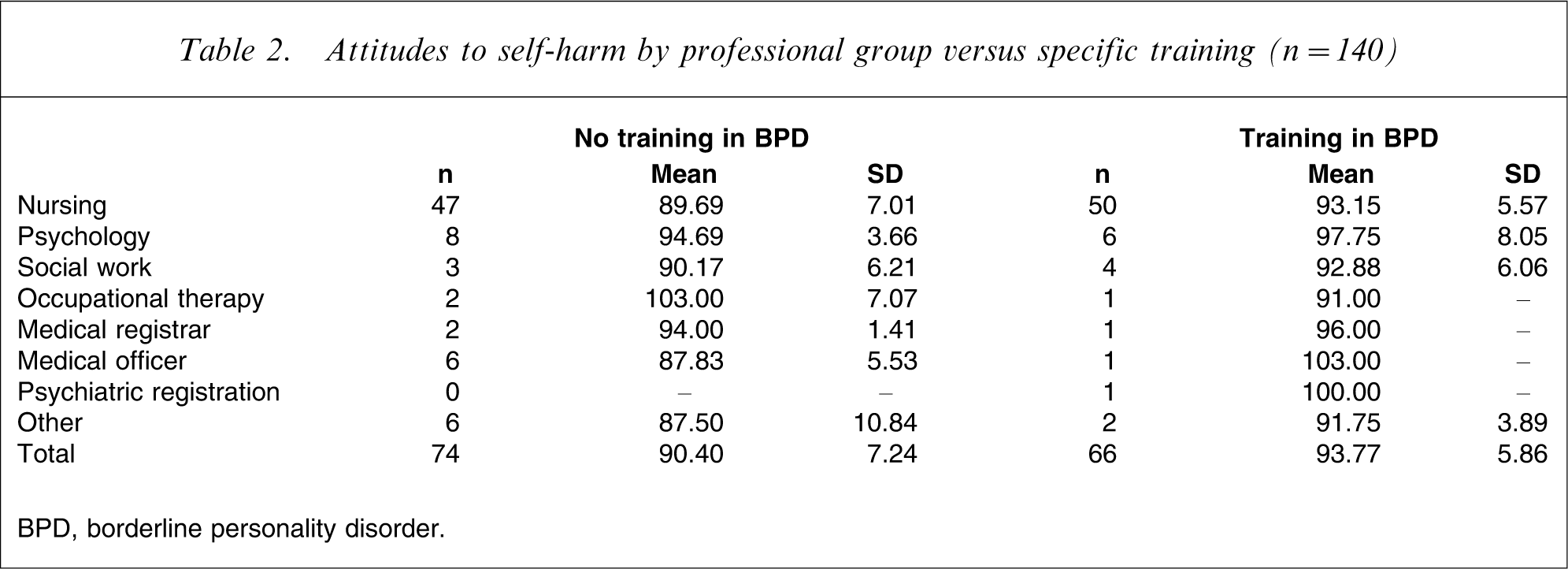
BPD, borderline personality disorder.
In order to examine the relative contribution of clinician characteristics, a multiple regression was conducted and is reported in Table 3. Primary field of work, years of experience and specific training made the strongest contributions to the prediction of attitudes towards self-harm in this regression equation, accounting for 8%, 2% and 2% of the variance explained, respectively.
Multiple regression for clinician characteristics predicting ATDSH in BPD patients (n = 140)
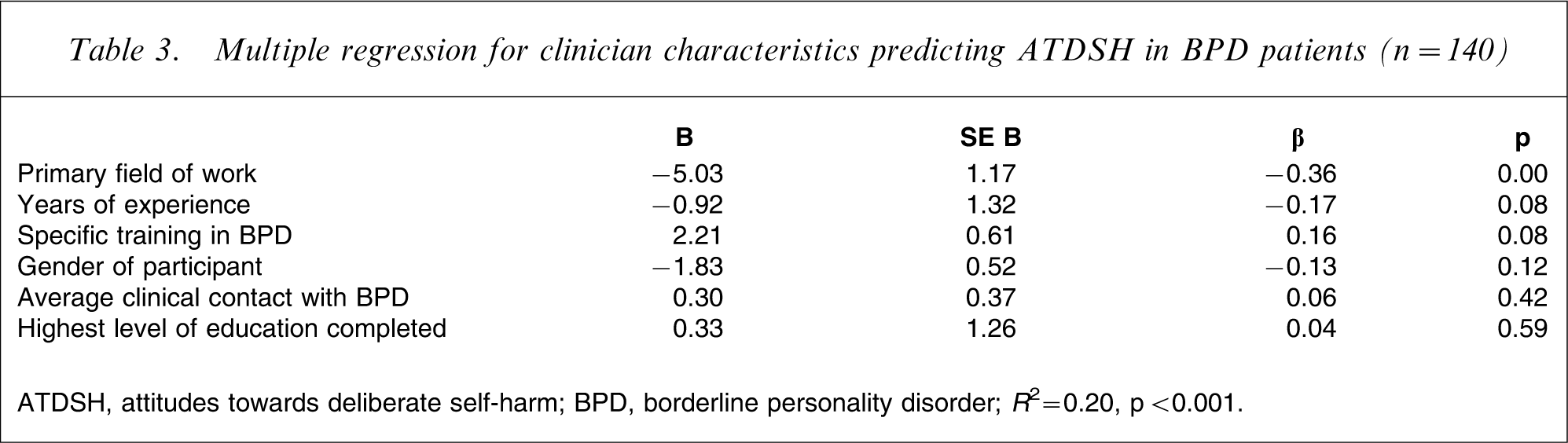
ATDSH, attitudes towards deliberate self-harm; BPD, borderline personality disorder.
R 2=0.20, p < 0.001.
Discussion
The present results suggest that, in this cohort of participants, a number of factors do influence a professional's attitude towards BPD patients who engage in self-harm. These include the professional's service setting, their level of experience and whether they have undertaken training specific to developing an understanding of BPD. More specifically, there was a statistically significant and large difference found between the attitude ratings of clinicians employed in the mental health service setting, compared with clinicians working in the area of emergency medicine. The significantly lower attitude scores of the clinicians from emergency medicine may be a function of the form of contact that this group typically has with BPD patients. Emergency medicine clinicians are required to provide urgent medical attention to the patient with BPD following episodes of self-harm and this may result in such professionals having a greater difficulty in maintaining an empathetic attitude to such patients. This may also be influenced by the high level of distress in which the patient with BPD presents in the emergency department immediately following self-mutilation or a suicide attempt. Mental health clinicians who provide ongoing management and treatment for BPD have more positive attitudes to working with this patient group, and this may be influenced by their more sustained and involved level of care, where they are able to appreciate the development of the disorder and the specific difficulties experienced in the patient's personal life.
Another significant finding was that the female clinicians across both mental health and emergency medicine service settings had more positive attitudes towards patients with BPD, although this difference was not significant when controlling for other factors. The ability of female clinicians to empathize with the patient may be related to the traditional sex role of the female being more able to nurture patients with significant emotional difficulties [15], [16]. Furthermore, the difference observed in the attitude ratings between male and female clinicians may be related to the higher presentation of female patients being diagnosed with BPD. Men are in the minority of patients receiving the diagnosis of BPD [17], with 70–75% of patients with the disorder being female [18].
In the present sample, factors such as the frequency of contact with patients with BPD, level of university training completed, and years of clinical experience held by the clinicians across mental health and emergency medicine were not associated with attitude ratings towards such patients. In terms of maintaining an empathetic approach and positive attitude towards DSH in patients diagnosed with BPD, this suggests an alternative to the conventional wisdom that it is always necessary to allocate BPD patients to highly trained and experienced health professionals for all aspects of their clinical management. The present results at least suggest that all clinicians across various skill and education levels appear to be equivalent in their attitudinal ratings and that other factors are more predictive of positive attitudes to BPD patients. It needs to be noted, however, that this implication of the study can be drawn only in relation to professional attitudes, and this may not be a reflection of the knowledge or ability of the clinician to provide necessary and effective medical and psychotherapeutic treatment to BPD patients.
The difference found in attitude ratings towards BPD in health professionals who have acquired specific and specialized training in BPD was moderate in size and remained close to statistical significance when controlling for other factors. This finding is consistent with previous research [13], [14]. Further analysis, however, of the data suggests that such training is more effective for nursing and medical clinicians, who showed significant improvement in their attitude ratings if they had attended training. Interestingly, the allied health participants such as social workers and psychologists did not appear to further improve in their attitude scores if they had received specific training in BPD. They did, however, report significantly more positive attitude ratings to working with BPD than the nursing and medical clinicians.
These differences in professional groups may suggest that basic professional trainings in psychosocial factors in mental illness may predispose allied health clinical to more positive attitudes to patients with severe personality disorders than traditional biomedical trainings. Such differences found between the attitude ratings among allied health professionals and their nursing and medical counterparts may be related to the limited efficacy in the use of the medical model in the psychotherapeutic treatment of BPD. Nursing and medical training may place greater emphasis on the biology of health conditions, including mental disorders, than that of standardized allied health training. Unfortunately the use of psychopharmacology in the treatment of BPD has yielded inconsistent results, with only limited efficacy found for some antipsychotic and antidepressant drugs, and mood stabilizers in symptom reduction with BPD [19]. Although all disciplines consistently strive for evidence-based practice, it could be argued that the training of allied health professionals in the realm of mental disorders appreciates more the aetiological constellations of personality disorder, and the treatment focus remains fixed on psychotherapeutic strategies to achieve change in the disturbed behaviours typically observed in BPD. The basic training of allied health clinicians appears to promote more empathetic attitudes towards working with BPD, which remain positive regardless of access to targeted education on BPD. Regardless of university or hospital training, both nursing and medical health professionals show significantly improved attitudes to working with DSH in patients with BPD with access to specific training on the disorder.
In the words of Marsha Linehan, ‘individuals meeting the criteria for BPD are flooding mental health centres and practitioners’ offices … Borderline patients are so numerous that most practitioners must treat at least one …’ [20]. Contact with patients diagnosed with BPD who display serious and sometimes chronic self-harm is a common experience for most clinicians. Pessimistic attitudes regarding prognosis and the failure to maintain a positive approach, and therefore respond therapeutically, can result in the patient feeling critically judged and dismissed. This in turn limits the efficacy of interventions and may well add to the chronicity of such severe presentations [21]. Although traditionally clinicians equate BPD patients manipulativity and therefore are reluctant to engage with them [22], there is emerging evidence that training and education can assist in the improvement of professional attitudes toward working with this patient group. The current study found that significant improvements in attitudes of health professionals, across both mental health and emergency medicine service settings, can be achieved with access to specific training and education in the area of BPD. Greater empathy and understanding can be achieved through improving health professionals’ attitudes towards working with self-harm in patients with BPD, resulting in a more considered and tolerant approach to the patients’ behavioural difficulties.
Footnotes
Acknowledgements
Thanks to all participants across the three health services who gave their time to complete the necessary questionnaires, Neroli Sawyer for her data analysis support, and Dr Leonardo Rodriguez for his guidance and main supervision of the research area. This work was undertaken in part fulfilment of a Doctor of Philosophy in Psychological Medicine by Amanda Commons Treloar at Monash University, Melbourne, Australia.