
Abstract
Keywords
Attitudes of health professionals towards patients diagnosed with borderline personality disorder (BPD), or those presenting with deliberate self-harm (DSH) behaviours have generally been shown to be negative and derogatory [1–3], across both mental health and emergency medicine service settings [4–7]. A review of these studies shows that health professionals across many different services and indeed countries often avoid contact with patients with BPD, or fail to engage them in any meaningful dialogue as to the reasons behind their DSH behaviours. BPD patients are reported to often be left to wait in the emergency department upon presentation to such departments for attention to their self-injury, and the allocation of these patients to mental health clinicians upon entry to mental health services is also problematic, with many clinicians not wanting to work with this disorder [1], [4–6]. Given that the clinical picture of BPD is of severe functional impairment that often includes unemployment, substance abuse, and distressing interpersonal relationships [8], and that such impairments often impact on the ability of the patient with BPD to commit to and participate in ongoing treatment or therapy, the task of keeping the BPD patient in therapy is primarily dependent upon a strong therapeutic alliance with a mental health professional. For this reason, maintaining an appropriate professional attitude towards patients with BPD who engage in DSH behaviours is essential.
Negative countertransference reactions, particularly in response to the behavioural patterns of recurrent self-mutilation and self-poisoning, unfortunately impact on the patient's engagement in therapy, and thus the provision and efficacy of treatment interventions. Working with patients with BPD has well-acknowledged challenges, not the least of which is that attempts to prevent further self-injury or overdose can appear ineffectual in the context of recurrent DSH behaviour [1]. The importance of tolerance and understanding of the patients’ difficulties is paramount, because unsympathetic responses also tend to escalate behavioural disturbance [9]. Many studies have suggested the provision of targeted clinical education on BPD in an attempt to improve clinician attitudes and produce more consistent and empathetic behavioural response to patients with this particular disorder [10], [11]. A person's attitude is constructed from past experience, feelings, behavioural responses and knowledge on a particular object, and as such this can be further consolidated or even changed or altered with the use of educational methods, such as conceptual frameworks and guided practice standards, where further knowledge can be provided and therapeutic responses instructed to reduce feelings of inadequacy or confusion [12]. Holding a particular attitude increases the probability that a person will act in a certain way [13], and unfortunately negative and derogatory attitudes in clinicians, as shown by the literature, can result in clinicians being less likely to produce empathetic or compassionate responses in contact with BPD patients in the health system.
To assist the clinician in the maintenance of empathy, access to clinical training in BPD has been shown to improve professional attitudes towards working with BPD in some preliminary studies. Following training on BPD conducted over a 2-day period, clinicians found an increased optimism, enthusiasm and positive feeling towards working the BPD patients, which was maintained at 3–5-month follow up [14]. Further assessment of attitudes using a larger representative sample of clinicians from public mental health and substance abuse services also supported an increase in confidence in working with BPD following specific training in the area [15]. Given that patients with BPD also frequently present to emergency medicine facilities, in addition to mental health services, an assessment of the use of education with this group of health professionals is also warranted, although not a focus of the current literature.
Using clinical education to address the negative attitudes of mental health and emergency medicine clinicians, through providing a theoretical basis for which to interpret the common behavioural disturbance of DSH in BPD, was the primary aim of the present study. The current study examined the effect of attending targeted clinical education on clinician attitudes towards working with DSH behaviours in BPD. The targeted clinical education programs were provided to two target groups of health professionals: emergency medicine and mental health clinicians. The influences of the clinician's service setting, occupational area, gender, level of university training, years of clinical experience, and completion of prior training in BPD on the change in attitudes of health professionals towards working with BPD patients who engage in DSH behaviours were also examined.
Method
Participants
The participants in this study were 99 registered practitioners across two Australian health services, Ballarat Health Services (n = 13) and Barwon Health (n = 30), and a New Zealand health service, Nelson Marlborough District Health Board (n = 56). Mental health and emergency department staff of these health services were asked to participate if, in the course of their employment, they encountered patients diagnosed with BPD. The rate of participation was 24.07% of clinicians approached at departments within Ballarat Health Services, 13.39% of clinicians approached at departments within Barwon Health, and 42.42% of clinicians approached at departments within Nelson Marlborough District Health Board. All participants were eligible for participation in the current study if they were a registered health practitioner. No exclusion criteria were used.
Materials
Participants were provided with a purpose-designed demographic questionnaire. Demographic questions included gender, years of clinical experience, formal education completed, primary occupation, service setting, and average clinical contact with BPD patients. The participants were also given the Attitudes Towards Deliberate Self-Harm Questionnaire (ADSHQ), which consists of 33 items scored on a 4-point Likert scale, ranging from 1 = strongly disagree to 4 = strongly agree, with no neutral response being allocated [16]. In order to reduce response bias, one-third of the items are phrased in the negative direction. The range of possible scores on the ADSHQ is 33–132, with higher scores reflecting more positive attitudes. Sample items are: Dealing with self-harm patients is a waste of the health-care professional's time; I deal effectively with deliberate self-harm patients; Self-harm patients just clog up the system. Factor analysis conducted on the ADSHQ produced four primary factors: (i) perceived confidence in assessment and referral of DSH patients; (ii) ability to deal effectively with DSH patients; (iii) use of an empathetic approach; and (iv) hospital regulations that guide practice. The reliability of the ADHSQ using Cronbach's αfor each of these four dimensions is: 0.71, 0.74, 0.67, and 0.57, respectively [16]. In the current study, the Cronbach's αcoefficient for the total scale was 0.75.
The clinical education programs were compiled using Microsoft PowerPoint and contained the following information: research findings on attitudes to BPD, prevalence rates, DSM-IV diagnostic criteria, aetiological factors, definitions and rates of self-harm and suicide, and therapeutic responses to BPD. Each education session then illustrated the applicable concepts of the theoretical discussions on BPD using the presentation of case studies of three female patients diagnosed with BPD. Clinical guidelines to working with BPD, including Crisis Intervention in Emergency Department Guidelines [17] and National Clinical Practice Guideline Number 16: Self-harm [18] were also provided at the end of the education program. The education material was presented in a lecture format with 90 minutes of lecturing by the first author. Participants also discussed the content in a seminar style for 30 minutes with input from the educator.
Procedure
Following consultation with management staff, and completion of the requirements for ethical approval at the three health services, the education programs were delivered during staff development time at the relevant health service. Upon arrival at the education program, participants were provided with an explanatory statement and a consent form, and outcome measures were administered. All participants were requested to consider their responses on the ADSHQ in relation to their contacts with DSH patients diagnosed with BPD only. Responses and completed demographic questionnaires were then returned in a sealed envelope, separate from the completed consent forms prior to the education being provided. At the completion of the education program all participants were required to complete the ADSHQ again, which were collected immediately prior to the participants returning to their usual clinical practice. The participants were not able to review their previous responses on the ADSHQ, before education attendance, because these were collected prior to the provision of clinical training. The coding of the questionnaires, however, enabled the pairing of post-education participant responses with the pre-education attitude ratings. No coding was used on the consent forms to protect the anonymity of the participant response from the researcher.
Results
Following a review of the initial data set that indicated a normal distribution and equal variance among the responses, univariate and multivariate analyses were conducted. No cases required deleting due to missing data.
The demographic information of this cohort of 99 participants are presented in Table 1. The sample consisted of 33 emergency medicine clinicians and 66 mental health clinicians across the three health services.
Subject details (n = 99)
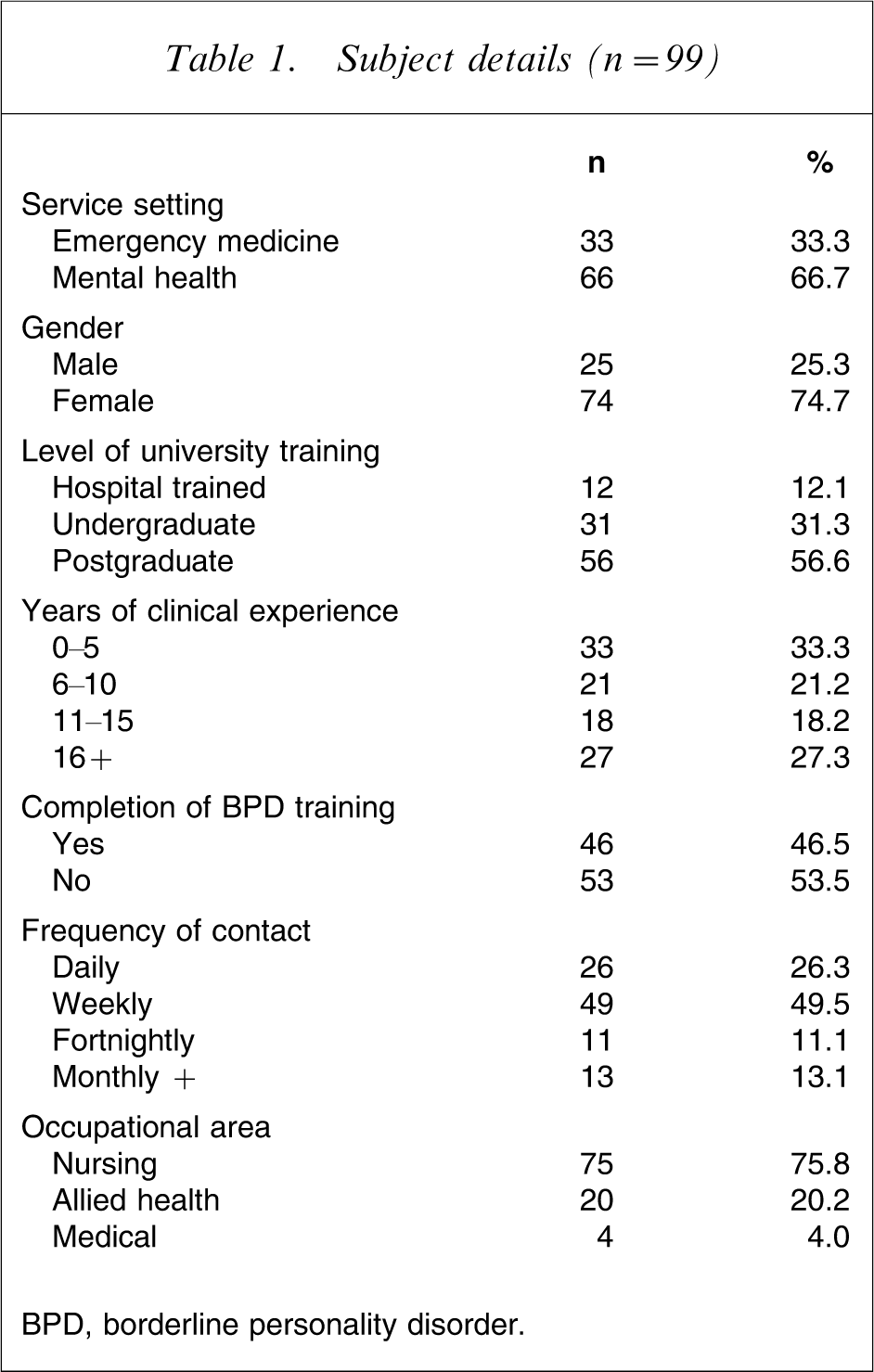
BPD, borderline personality disorder.
The mean pre- and post-education scores and standard deviations on the ADSHQ for the participant group are presented in Table 2. Overall comparison of the ADSHQ scores obtained before and after attendance at the education programs showed that there was a significant improvement in attitude ratings towards working with DSH behaviours in BPD patients, with a small to medium effect size (t(98) = − 6.127, p = 0.000, d = 0.40).
ADSHQ scores
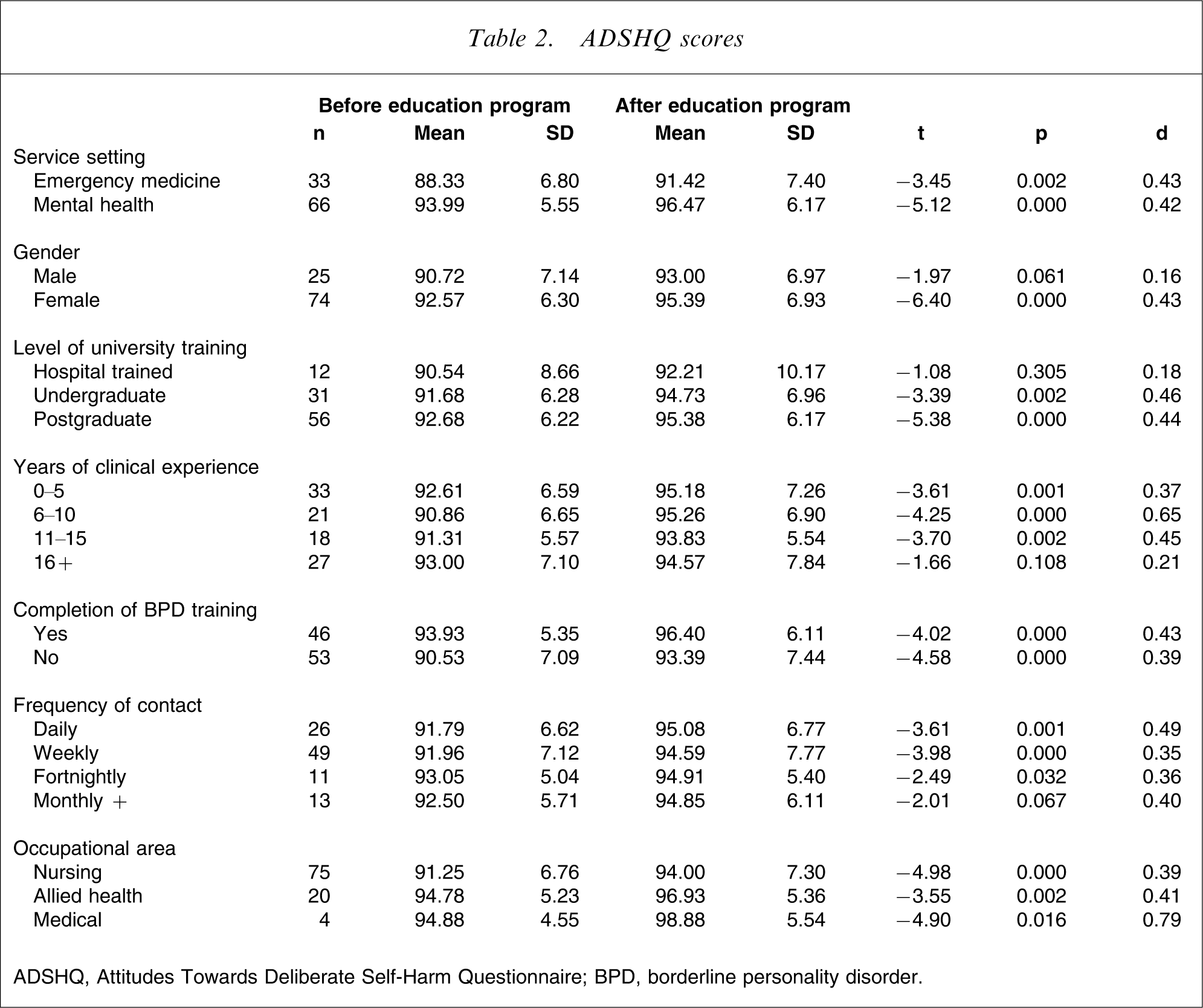
ADSHQ, Attitudes Towards Deliberate Self-Harm Questionnaire; BPD, borderline personality disorder.
Analysis of subscales within the attitude measure showed that the strongest impact of the educational package was obtained on the confidence in assessment and referral (d = 0.43), and improved ability to deal effectively with patients with BPD (d = 0.30). Impacts on the use of an empathetic approach and knowledge of hospital regulations were minimal (d = 0.10 and d = 0.12, respectively). The distribution of rates of change is presented in Figure 1.
Frequency distribution of changes in attitudes scores following educational intervention, comparing emergency medicine and mental health clinicians (N = 99).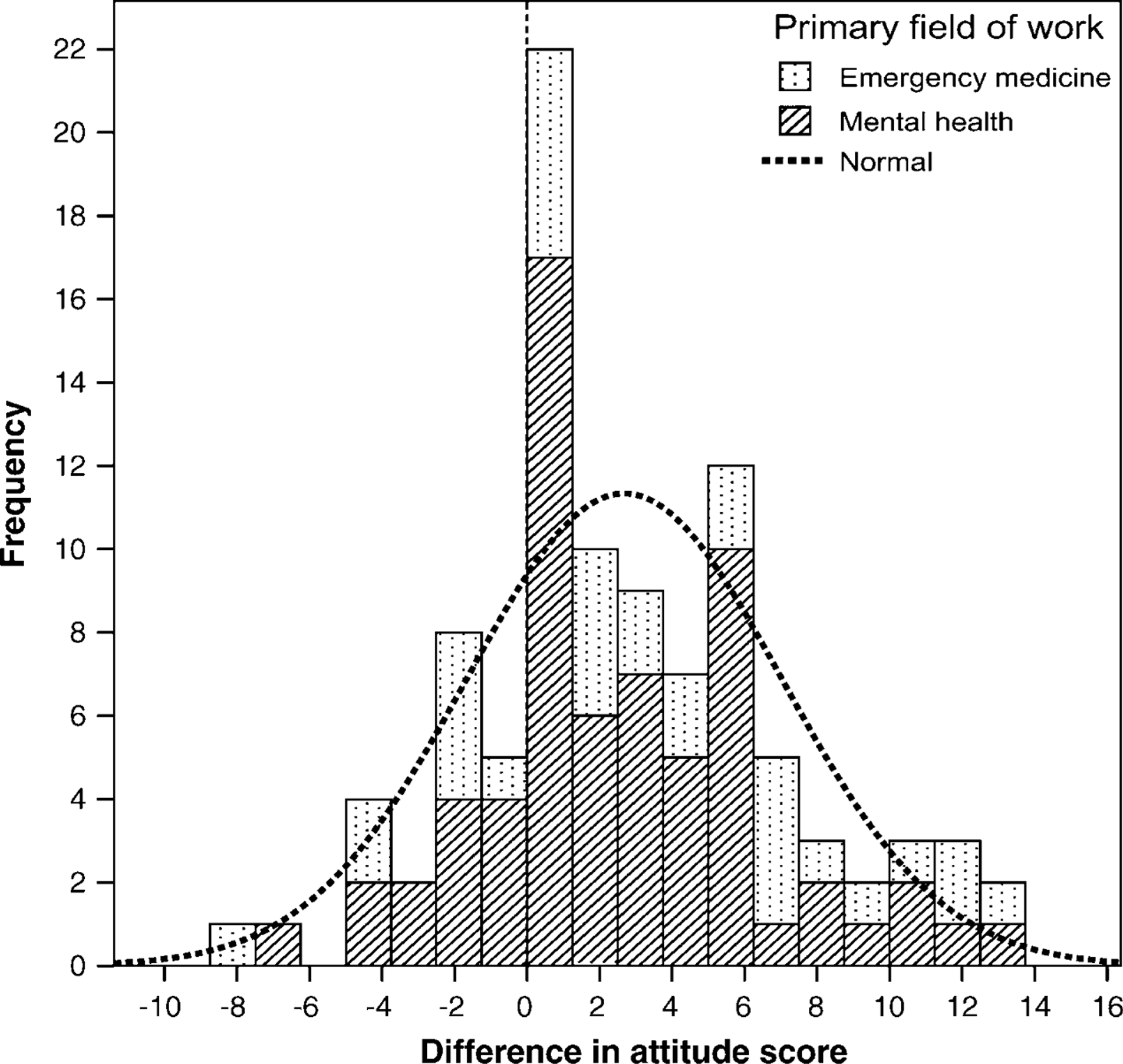
In terms of service setting comparisons, both emergency medicine and mental health clinicians demonstrated statistically significant improvement in the attitude ratings to DSH behaviours in BPD following their attendance at the education programs with a medium effect size (t(32) = − 3.45, p = 0.002, d = 0.43, and t(65) = − 5.12, p = 0.000, d = 0.42, respectively).
Upon comparison of gender groups, it is apparent that only female clinicians demonstrated a statistically significant improvement in their attitude ratings after education program attendance (t(73) = − 6.40, p = 0.000, d = 0.43), as compared with male clinicians, who showed a small and not statistically significant improvement in the ADSHQ ratings (t(24) = − 1.97, p = 0.061, d = 0.16). Participants who had completed undergraduate and postgraduate university training demonstrated significant and medium-sized improvements in attitude ratings following attendance at the education programs (t(30) = − 3.39, p = 0.002, d = 0.46, and t(55) = − 5.38, p = 0.000, d = 0.44, respectively). Interestingly, hospital-trained health professionals did not show a statistically significant improvement in their attitudes towards working with DSH behaviours exhibited in BPD following their attendance at the education programs (t(11) = − 1.08, p = 0.305, d = 0.18).
All clinicians reporting 0–15 years of clinical experience had significant improvement in attitude ratings, but the small number of clinicians with ≥16 years of clinical experience did not demonstrate a statistically significant improvement in attitude scores, after education attendance (t(26) = − 1.66, p = 0.108, d = 0.21). For participants who had completed prior training in BPD, a higher attitude rating was recorded after education program attendance of medium effect size (t(45) = − 4.02, p = 0.000, d = 0.43). The same significant level of attitudinal improvement was also observed for those participants who had not attended prior training in BPD (t(52) = − 4.58, p = 0.000, d = 0.39)
Examination of clinician ratings according to demographic groups showed that all clinicians reporting daily to fortnightly contact with patients with BPD had significant improvement in attitude ratings following their attendance at training with small to medium effect sizes; clinicians who recorded monthly or longer time interval between contacts with patients diagnosed with BPD also improved in their attitude ratings, but they failed to show a statistically significant improvement in their attitudes towards working with DSH behaviours exhibited in BPD following their attendance at the education programs (t(12) = − 2.01, p = 0.067, d = 0.40). These ratings did, however, demonstrate a medium effect size and were approaching statistical significance.
The attitude ratings before and after education attendance for nursing clinicians, allied health clinicians and medical clinicians showed that all clinicians across these three occupational areas had statistically significant improvement in their attitude ratings towards working with DSH behaviours in BPD, with medium to large effect sizes (t(73) = − 4.98, p = 0.000, d = 0.39; t(19) = − 3.55, p = 0.002, d = 0.41; and t(3) = − 4.90, p = 0.016, d = 0.79, respectively; Table 2).
Further examination of these attitude ratings, using a series of one-way between-groups analysis of covariance (ANCOVAs), was then completed to compare the demographic comparison groups to determine whether, after adjusting for the differing pre-measure ADSHQ scores, there were any significant differences in the improved ADSHQ ratings observed, after attendance at the education program (Table 3). There were no violations of assumptions of normality, linearity, homogeneity of variances or regression slopes, and reliable measurement of the covariate. After adjusting for pre-education ADHSQ scores, there were no significant differences found in the level of improvements observed in ADSHQ scores following attendance at the education programs across participants in the different service settings, those who had and had not completed prior training in BPD, and across the three occupational areas of nursing, allied health and medical fields. All clinicians across the emergency medicine and mental health service settings, and occupational fields had equivalent improvements in their attitude ratings to working with DSH behaviours in BPD, after controlling for their pre-measure ADSHQ scores. Similarly, completion of prior training in BPD was not a prerequisite to greater attitudinal change; those participants who had not completed prior training in this disorder demonstrated the same level of improvement in ADSHQ score after attendance at the education programs (Table 3).
ANCOVA for clinician comparison groups, with pre-measure ADSHQ ratings as covariate (n = 99)
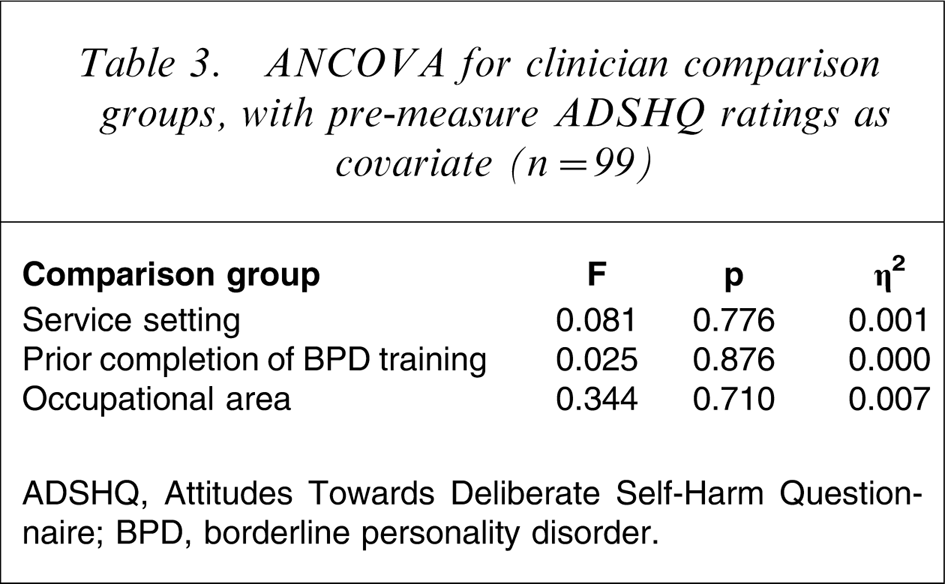
ADSHQ, Attitudes Towards Deliberate Self-Harm Questionnaire; BPD, borderline personality disorder.
Discussion
In this cohort of participants the completion of targeted clinical education on BPD resulted in statistically significant improvement in clinician attitude ratings towards working with DSH behaviours in patients with BPD. Such findings are consistent with previous research [14], [15]. More positive attitudes expressed towards working with DSH in patients diagnosed with BPD were reported by participants once they obtained knowledge relating to research findings on attitudes to BPD, prevalence rates, DSM-IV diagnostic criteria, aetiological factors, definitions and rates of self-harm and suicide, therapeutic responses to BPD, clinical guidelines to working with BPD, and some form of theoretical framework to understanding the behavioural presentation of DSH in patients with BPD. Given that the education intervention consisted of a combination of specific knowledge, time devoted to discussing and reflecting upon the issues, and active attendance and involvement in professional development, it is difficult to discern precisely the main factors responsible for this improvement in attitudes.
It was shown that clinicians from both the emergency medicine and mental health settings were able to demonstrate statistically significant improvement in their attitude ratings towards this patient group with access to targeted clinical education, and the medium effect sizes found suggest that these may be of clinical significance. This is important given that emergency medicine clinicians are typically negative in their responses to patients diagnosed with BPD, or those who present to the emergency department for treatment of DSH injuries [5], [7], [16], [19], [20]. Similarly, mental health clinicians can also demonstrate derogatory attitudes towards working with DSH behaviours, and the BPD patient group collectively [3], [6], [21]. As evidenced by the current research program, improved attitudes towards this patient group, or working with their difficult behavioural presentations of DSH, can be achieved through providing access to targeted clinical education on this complex disorder.
Interestingly, male clinicians did not exhibit the same level of improvement in attitude ratings following their attendance at the target clinical education program as the female clinicians, who demonstrated statistically significant change with a large effect size. Male clinicians also rated their attitudes more negatively than female clinicians before the intervention. This may be a function of the ability of female clinicians to be more able to empathize with the patients with significant emotional difficulties [22], [23], and may be related to the higher presentation of female patients being diagnosed with BPD [24]. It also suggests that different educational strategies may be required to improve the attitudes of male clinicians than those used in the current intervention (i.e. such as presenting case examples using male BPD patients).
Although clinicians who had completed university training (undergraduate and postgraduate studies) had significant improvement in their attitude ratings after education program attendance, hospital-trained clinicians failed to demonstrate similar levels of statistical improvement. This pattern was also demonstrated for clinicians across different years of clinical experience; only clinicians who held ≥16 years of clinical experience failed to show statistically significant improvement in their ADSHQ score after education attendance. Upon review of these two groups, an overlap was found: 91.67% (n = 11) of the hospital-trained clinicians reported holding ≥16 years of clinical experience, and 40.74% (n = 11) of the clinicians with ≥16 years of clinical experience were those who had received hospital training only.
There are several possible explanations for this finding. It may suggest that the education package was implicitly targeted towards participants with university level education, who tend to be more responsive to a seminar and discussion format. Such an interpretation is supported by the fact that intervention effects increase along with the level of university education, with postgraduate-educated participants improving the most in their attitudes. The finding may also reflect a generation of clinicians who are resistant to attitude change. This may be related to strongly entrenched and traditional attitudes and practices in health and psychiatry, where the biomedical model may have been more dominant during this generation's training. Such a group tends to be sceptical of the responsiveness of patients with BPD to mental health interventions. It could be argued that the basic hospital training of these clinicians may not have allowed for an in-depth appreciation of the aetiological constellations of personality disorder, and the use of psychotherapeutic theoretical frameworks and treatment models, which may be provided to other health clinicians during university training. Altering clinical practice obviously becomes difficult after a sustained period of interaction with the BPD patient group.
When comparing the clinician groups in terms of completion of prior training in BPD, those who had not received previous training in the area had statistically significant improvement in ADSHQ scores after access to such training; those clinicians who had received targeted education on BPD prior to their completion of the current research program, also had a significantly more positive response to DSH behaviours in BPD. This was also found across the different occupational fields of the participant group: nursing, allied health, and medical practitioners. These findings support the need for access to regular training opportunities in the area of BPD for all health clinicians, across the different service settings and occupational fields, to facilitate empathetic responses to BPD patients. Ongoing clinical education opportunities can assist in the improvement and maintenance of positive clinician attitudes to working with patients with this disorder.
Across the clinician groups that reported varying frequency of contact with patients diagnosed with BPD, all showed some improvement in their attitude ratings towards BPD. Clinicians that had contact with this patient group on a monthly or longer time interval, however, did not record statistically significant improvement in ADSHQ scores after education program attendance. This may be attributed to the difficulty in applying the educational material to the clinical practice with this patient group, which is not all that familiar to them. In this cohort of participants, those clinicians who had at least fortnightly contact with BPD patients demonstrated that the education program was useful in the consideration of the disorder, which in turn could enable an improved response to working with this patient group.
When controlling for the different pre-education scores on the ADSHQ, all clinicians across the service settings of emergency medicine and mental health had an equivalent improvement in their attitude ratings following attendance at the education program. This type of response was also found across the three different occupational areas of nursing, allied health and medical fields, as well as among clinicians who had and had not received prior targeted clinical education in BPD. It is evident that through providing targeted clinical education and training in BPD, the derogatory attitudes typically found in clinicians in direct response to contact with patients diagnosed with BPD may be able to be improved, even when the clinicians have completed prior training in this disorder.
The present results suggest that access to clinical education on BPD can improve the attitude ratings of both emergency medicine and mental health clinicians to patients with this disorder, and suggest that regular access to such education may assist with the maintenance of positive attitudes and empathetic responses. The usefulness of the shift in attitude ratings, averaging 2–6 points on the ADSHQ for clinicians, in terms of true attitude change and clinical practice, does remain uncertain. The composition of the ADSHQ as an assessment tool, with participants requiring to respond with a clear indication of agree or disagree (and no neutral response being allocated), does suggest however, that there were some functional improvements in attitude ratings across the participant sample. Further limitations of the current study relate to the small sample size and a lack of more long-term follow up of attitude ratings after education. Assessing the direct impact of clinician attitude change on clinical practice and the longevity of improved attitude rates was beyond the scope of the current study and remains a suggestion for future research.
It is evident from the literature that DSH behaviours and the diagnostic categorization of patients as having BPD can often shape staff attitudes and therapeutic responses, and attempts to develop a more nuanced and empathetic understanding of self-harm within the context of personality disorder is clinically important in today's health system. It becomes imperative to ensure that all clinicians, across emergency medicine and mental health services settings, as well as across different occupational fields that are to come into clinical contact with BPD patients, receive regular access to training in this complex mental disorder.
Footnotes
Acknowledgements
Thank you to all participants across the three health services who gave their time to complete the necessary questionnaire and attend the education program, and Dr Leonardo Rodriguez for his guidance and main supervision of the research area. This work was undertaken in part fulfilment of a Doctor of Philosophy in Psychological Medicine by Amanda Commons Treloar at Monash University, Melbourne, Australia.