
Abstract
Bulimia nervosa (BN) during pregnancy can have serious consequences for both mother and child [1–3]. Although the relationship between psychosocial characteristics and BN has been investigated extensively in non-pregnant women [4] little is known about the relationship between such factors and BN during pregnancy. In particular, the association between psychosocial variables and patterns of continuation, incidence and remission of BN in pregnancy has not been investigated.
The Norwegian Mother and Child Cohort Study (MoBa) is a prospective birth cohort study designed to recruit a sample of 100 000 pregnant women. Information on eating disorders during and prior to pregnancy is collected. Using data from the first 41 157 mothers enrolled, we investigated the association between psychosocial characteristics and continuation, incidence and remission of broadly defined BN during pregnancy.
Methods
Participants
The data collection was conducted as a part of the MoBa study, directed by the Norwegian Institute of Public Health [5]. The study was approved by the appropriate regional ethics committees for medical research and the Norwegian National Data Inspectorate.
In brief, MoBa is a prospective pregnancy cohort that started in 1999 and it is estimated that the goal of 100 000 pregnancies will be reached by the end of 2008 [5]. Pregnant women are recruited through a postal invitation after registering for a routine prenatal ultrasound examination in their local hospital at approximately 17 weeks’ gestation. Participating women sign informed consent to take part in a longitudinal study, donate blood and urine samples, and receive a questionnaire. The present study is based on the first questionnaire (Q1). Overall, from 1999 to 2006, approximately 42% of invited mothers agreed to participate in MoBa.
The MoBa cohort is linked to Norwegian health registries, particularly the Medical Birth Registry of Norway (MBRN) to capture pregnancy outcome variables. Since MBRN was established in 1967 all stillbirths and live births in Norway after 12 weeks of pregnancy have been reported through mandatory notification [6]. Data from the MBRN have been used for prior biomedical research [6–9].
The analysis population for this report included MoBa participants who (i) had identification information from both the MBRN and Q1; (ii) did not complete an early pilot version of the Q1 (n = 2599); (iii) had valid values for self-reported age, weight, and height; (iv) returned Q1 before delivery; and (v) had a singleton birth. If a woman enrolled in MoBa more than once (due to additional pregnancies), only the first pregnancy was included. Of the initial 54 714 pregnancies enrolled in MoBa, 41 157 (75%) met the five criteria and were included in this report. Respondents completed Q1 at a median of 18.1 weeks gestation (interquartile range = 16.7–20.1 weeks, range = 5.3–41.9 weeks).
Measures
Data for the present study came primarily from Q1, which includes assessment of a range of exposures and health outcome variables. Demographic data were obtained both from Q1 and MBRN.
Eating disorders
Q1 includes a number of items on eating disorders that were designed in accordance with the criteria for BN in DSM-IV [10], and have previously been used for studies of eating disorders in the Norwegian Institute of Public Health Twin Panel [11–13]. The binge eating item was designed to capture the two key features of binge eating: eating an unusually large amount of food and experiencing a sense of loss of control. Diagnostic algorithms were constructed from the questionnaire items to define the presence of broadly defined BN with a frequency of binge eating and compensatory behaviours of minimum once per week. Broadly defined BN was assessed both 6 months prior to pregnancy (retrospective assessment) and at the time of survey completion (i.e. first trimester of pregnancy) [14]. Lifetime BN was not assessed. The BN diagnosis was classified as missing if at least one of the diagnostic criteria were missing and if there were no affirmative responses to any of the other criteria.
Continuation of BN was defined as fulfilling criteria for BN both in the period 6 months prior to pregnancy and during the first trimester of pregnancy. Incidence refers to new cases of BN during early pregnancy in mothers who reported no BN in the 6 month period prior to pregnancy. Because lifetime BN was not assessed, incidence in this paper refers to onset of symptoms during pregnancy that were not reported to exist in the 6 months prior to pregnancy, but not necessarily first lifetime onset. Remission was defined as BN before pregnancy and the absence of both binge eating and compensatory behaviour during pregnancy, whereas partial remission refers to BN prior to pregnancy, continued presence of binge eating during pregnancy, but absence of compensatory behaviours.
Psychological variables
A five-item version of the Hopkins Symptom Checklist–25 was used to measure symptoms of anxiety and depression [15]. The short form has been shown to correlate highly with the total score of the original scale and have good psychometric properties [15], [16]. Self-report symptom scales such as the Hopkins Symptom Checklist have considerable temporal stability and seem to approximate the trait-like aspects of psychological functioning [17]. Items are scored according to a scale ranging from 1 to 4.
The cognitive component of subjective well-being was measured using the Satisfaction With Life Scale [18], [19]. This widely-used five-item scale has been shown to be a valid and reliable measure of life satisfaction, suited for use in a wide range of ages and applications [20]. Each item is scored 1–7.
Self-esteem was measured by a short version of the Rosenberg Self-Esteem Scale [21], widely used in eating disorder research [22–25]. It consist of four items and correlates well (r = 0.95) with the original 10 item scale [26]. Answers on each item were scored 1–4.
Relationship satisfaction was assessed using the Relationship Satisfaction Scale. This 10-item scale is partially based on the Marital Satisfaction Scale [27], and has been shown to correlate highly with the Quality Marriage Index [28] and have good psychometric properties [Røysamb E: personal communication]. Each item was scored 1–6.
The variables for each of the scales were constructed by adding the scores on all items and dividing this sum by the number of items in the respective scales.
Lifetime history of major depression was assessed using six questions designed to reflect the diagnostic criteria for the disorder in the DSM [29]. This method has previously been used for self-report purposes [30].
Sexual and physical abuse
Physical abuse was assessed at three different time points (during the pregnancy, last 6 months before pregnancy, and earlier). The various response categories were collapsed into a dichotomous yes/no variable reflecting lifetime abuse, with women reporting physical abuse at any time point in the yes category.
Sexual abuse was assessed using a question with four alternative answers, reflecting severity (from ‘no, never’ to ‘yes, have been raped’), at three different time points (during the pregnancy, last 6 months before pregnancy and earlier). A dichotomous variable reflecting lifetime sexual abuse was created. Women responding yes to any of the questions at any time point were included in the yes category.
Health behaviours
Q1 included one item assessing lifetime smoking (yes/no) and one item assessing smoking during pregnancy. The latter item had three response categories: ‘no’, ‘sometimes’, or ‘daily’. The last two categories were collapsed, and a dichotomous yes/no variable was created.
Frequency of alcohol consumption in the 3 month period prior to pregnancy was assessed using a question with several response categories. In order to capture potential problematic drinking behaviour rather than simply alcohol use, the categories were collapsed into a dichotomous variable. ‘Yes’ included drinking alcohol two or more times a week (approximately 7%) and ‘no’ included drinking alcohol once a week or less.
Statistical analysis
For this report we had three analytic goals: first, to compare psychosocial characteristics in women with BN in early pregnancy (continuation and incidence) and in women without eating disorders in the 6 months prior to pregnancy. Second, to investigate psychosocial characteristics associated with the presence of BN during the first trimester of pregnancy. Third, to investigate psychosocial characteristics associated with continuation, incidence and remission of BN during early pregnancy.
A Poisson regression model is considered suitable for the analysis of rates, both required for the second and third analytic goals, because it produces estimates of discrete counts, which can be divided by units of exposure [31]. What is called an ‘offset’ in these models enables the division of events by units of exposure. The Poisson regressions specified in this paper use generalized estimating equations for variance estimation and a description and justification of its usage in this context have been discussed before [14].
In the present paper events represent the discrete counts, and the number of mothers before pregnancy at risk for the event represents the units of exposure. The association between these estimated rates and psychosocial characteristics occurs with a psychosocial variable included as a covariate in the Poisson regression. Age and education (age only for incident cases) were also included as covariates to correct for any possible confounding.
We estimated the rate ratio of prevalence, incidence, remission and partial remission of BN during pregnancy. The rate ratio can be defined as the ratio of the rate (i.e. prevalence, incidence, remission or partial remission rate during pregnancy) in the exposed group versus the non-exposed group. There were at least nine psychosocial characteristics, thus there were at least nine models for each of the prevalence, incidence, remission and partial remission estimates.
The small number of BN reports during pregnancy required a separate model for each psychosocial characteristic to avoid over-fitting the models. Multiple tests were controlled for by the false discovery rate (FDR) [32].
Some of the psychological variables, symptoms of anxiety and depression, life satisfaction, self-esteem, and relationship satisfaction, had >3% of responses missing. Consequently, multiple imputation was an approach used in any model evaluating the psychological scale variables. This approach is appropriate for data that are missing at random [33] and this is the assumption we make regarding these data. The process of multiple imputation involved three steps: first, generation of five separate data sets with imputation of missing score responses through the SAS MI procedure using the Markov Monte Carlo method [33]; second, analysis of each of the five data sets using the methods as previously stated; and finally, compiling of the output from the second step using SAS MIANALYZE to create parameter estimates with their corresponding p and standard errors.
All analyses were done using SAS/STATA version 9.1.3 software (SAS Institute, Cary, NC, USA) for Windows and Solaris.
Results
Factors associated with BN during pregnancy
Ninety-six (0.2%) of the women in the sample fulfilled the criteria for broadly defined BN in the first trimester of pregnancy. Of these, 67 also reported having BN during the last 6 months prior to pregnancy, 26 had new cases of BN developed after pregnancy and three did not report BN status prior to pregnancy, and were classified as missing.
Table 1 presents descriptive statistics of psychosocial characteristics for women with BN in the first trimester of pregnancy and women with no eating disorder. We include two subgroups: women who had BN prior to pregnancy and continued to fulfil the diagnostic criteria during pregnancy, and new cases of BN in early pregnancy.
Subject psychosocial characteristics in the first trimester of pregnancy
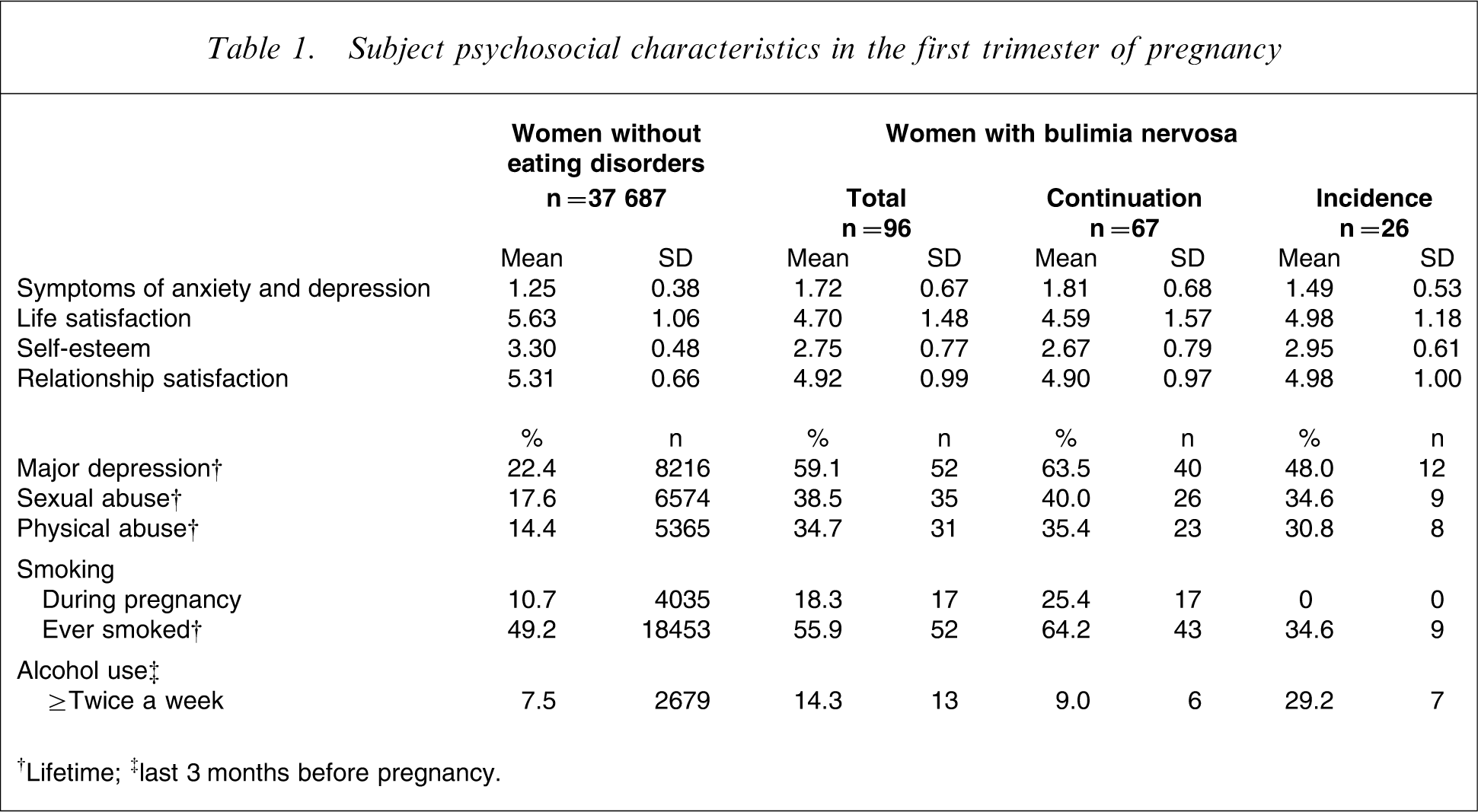
†Lifetime; ‡last 3 months before pregnancy.
Compared to women without eating disorders, women with BN scored on average >1SD higher on symptoms of anxiety and depression, >1SD lower on life satisfaction, self-esteem and relationship satisfaction, and reported nearly a threefold prevalence of lifetime major depression. Women with BN also reported double the frequency of lifetime sexual abuse and physical abuse, and higher rates of smoking both during pregnancy and lifetime, and higher rates of alcohol use before pregnancy. The greatest differences were observed in women who had BN both before and during pregnancy versus women without eating disorders.
All the psychosocial characteristics tested were significantly associated with BN in early pregnancy, except smoking and alcohol use (Table 2).
Prevalence rate ratio for bulimia nervosa during pregnancy †
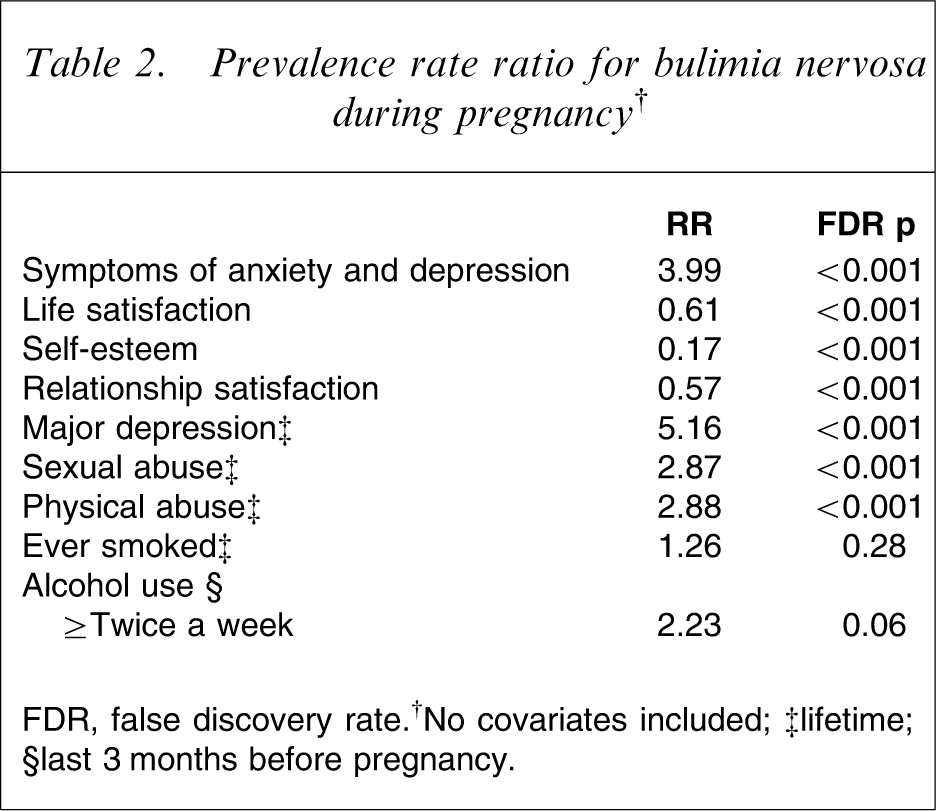
FDR, false discovery rate. †No covariates included; ‡lifetime; §last 3 months before pregnancy.
Factors associated with continuation of BN during pregnancy
Continuation of BN from the last 6 months prior to pregnancy to the first trimester of pregnancy was not significantly associated with any of the psychosocial characteristics studied (Figure 1).
Associations between continuation of bulimia nervosa during pregnancy and psychosocial characteristics (adjusted for age and education of mother). †Lifetime; ‡last 3 months before pregnancy. CI, confidence interval; FDR, false discovery rate.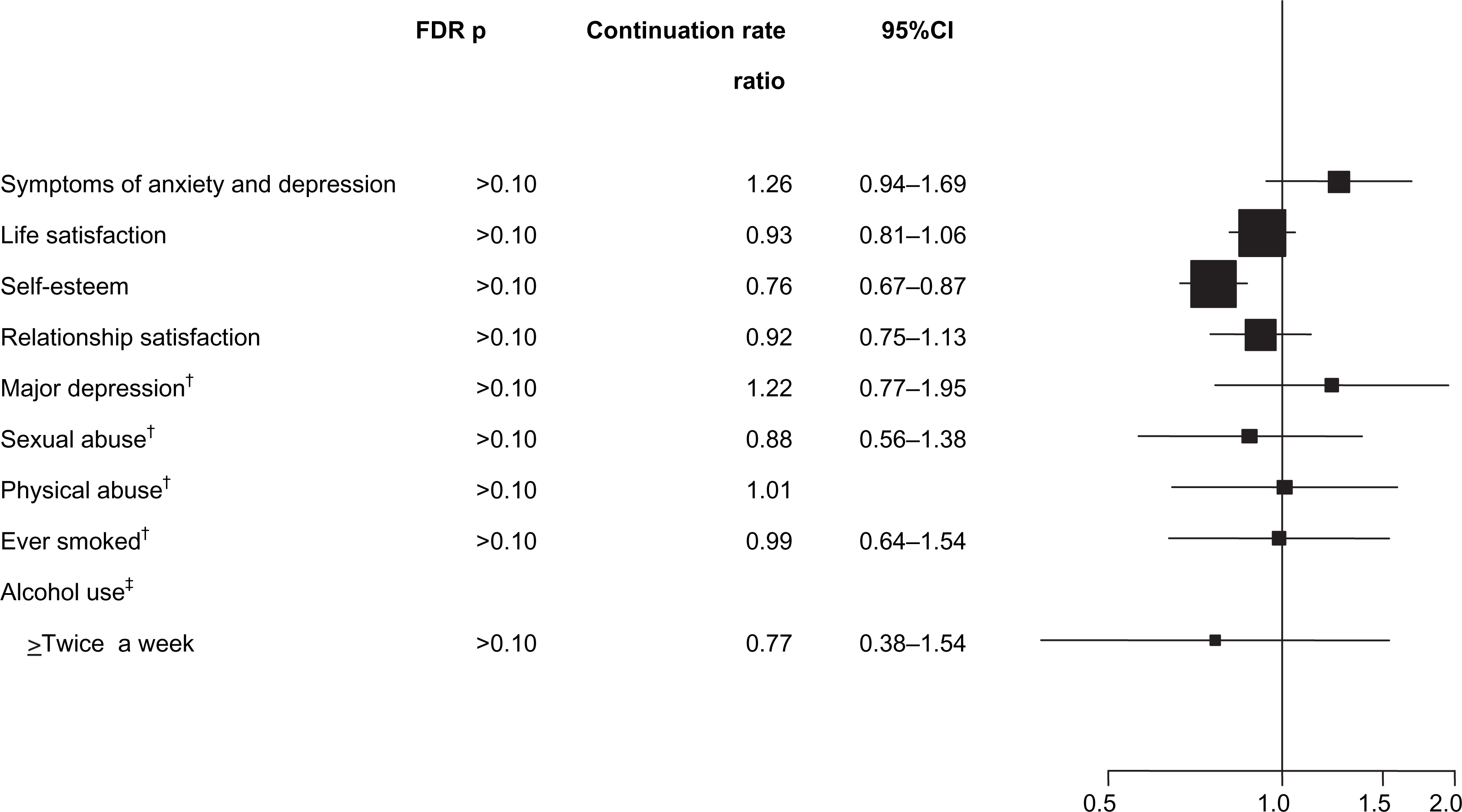
Factors associated with incident BN during pregnancy
Figure 2 shows the associations between the psychosocial characteristics and incidence of BN during pregnancy adjusted for mother's age. High scores on symptoms of anxiety and depression, and low scores on life satisfaction, and self-esteem were significantly associated with incidence of BN (FDR p = 0.003, FDR p = 0.003 and FDR p = 0.007, respectively). Lifetime major depression, alcohol consumption before pregnancy and relationship satisfaction were significantly associated with incidence before but not after correcting for multiple testing.
Associations between incidence of bulimia nervosa during pregnancy and psychosocial characteristics (adjusted for mother's age). †Lifetime; ‡last 3 months before pregnancy. CI, confidence interval; FDR, false discovery rate.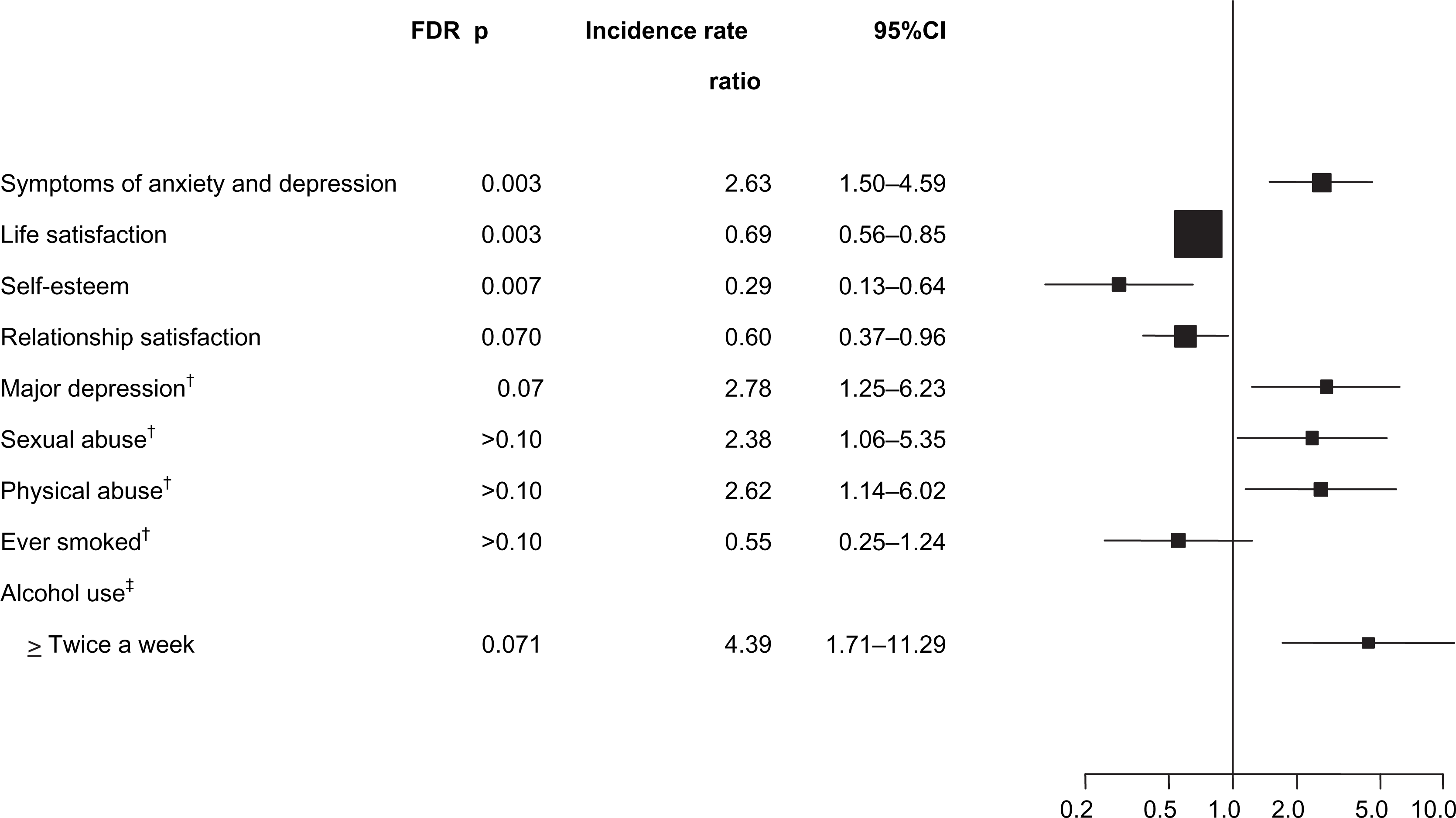
Factors associated with remission and partial remission of BN during pregnancy
Of the 290 women who fulfilled the criteria for BN in the 6 months prior to pregnancy, 77 went into remission (i.e. discontinued both binge eating and compensatory behaviours) and 73 had partial remission (i.e. continued binge eating but discontinued compensatory behaviours) in the first trimester of pregnancy.
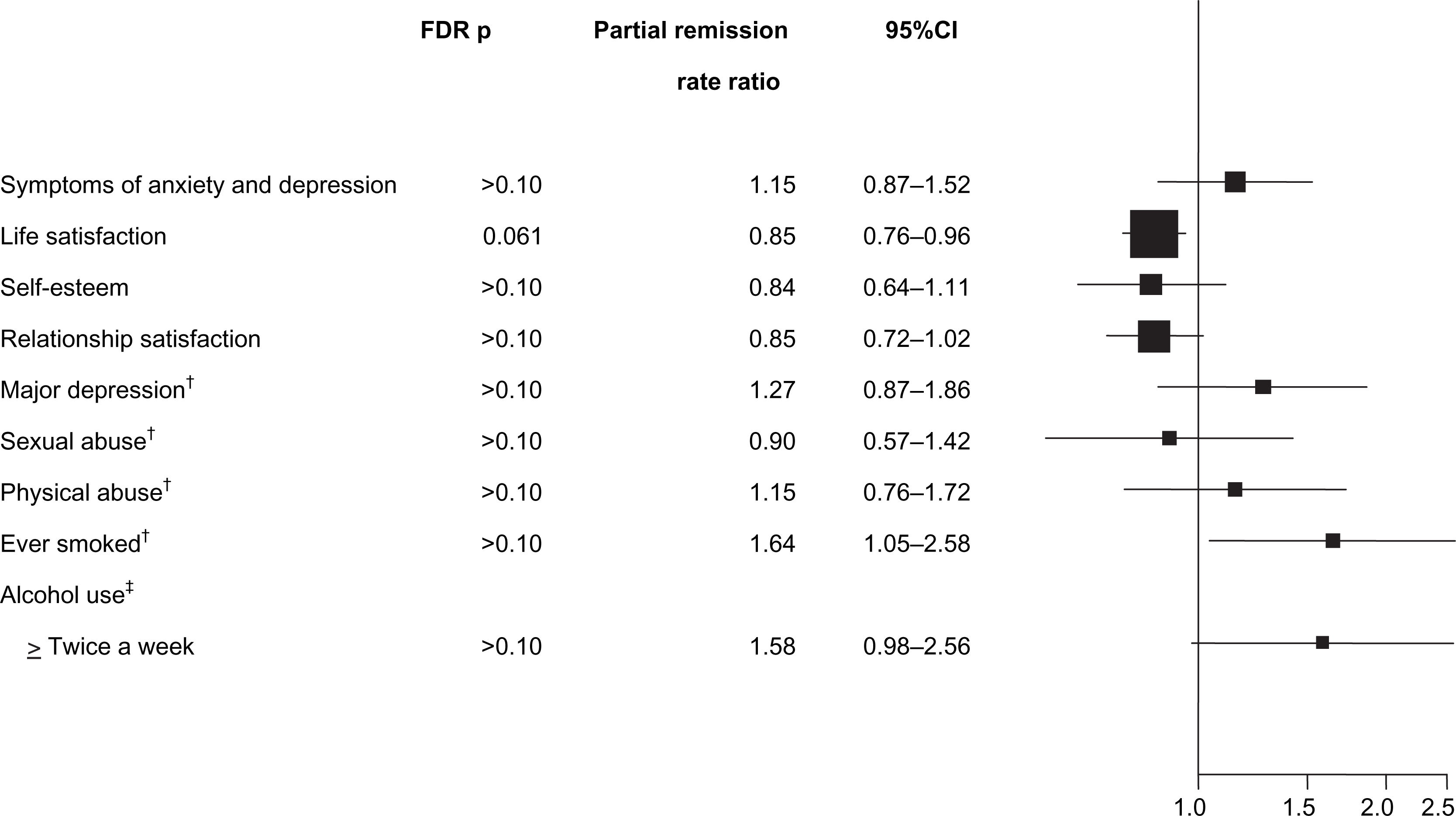
As shown in Figure 3, only life satisfaction and self-esteem were significantly associated with remission of BN when controlling for mother's age and education and correcting for multiple testing (FDR p = 0.02 and FDR p = 0.02, respectively), and none of the psychosocial characteristics was significantly associated with partial remission (Figure 4).
Associations between psychosocial characteristics and remission during pregnancy for women with BN before pregnancy (adjusted for age and education of mother).
†
Lifetime;
‡
last 3 months before pregnancy. CI, confidence interval; FDR, false discovery rate. Associations between psychosocial characteristics and partial remission during pregnancy for women with BN before pregnancy (Adjusted for age and education of mother). †Lifetime; ‡last 3 months before pregnancy. CI, confidence interval; FDR, false discovery rate.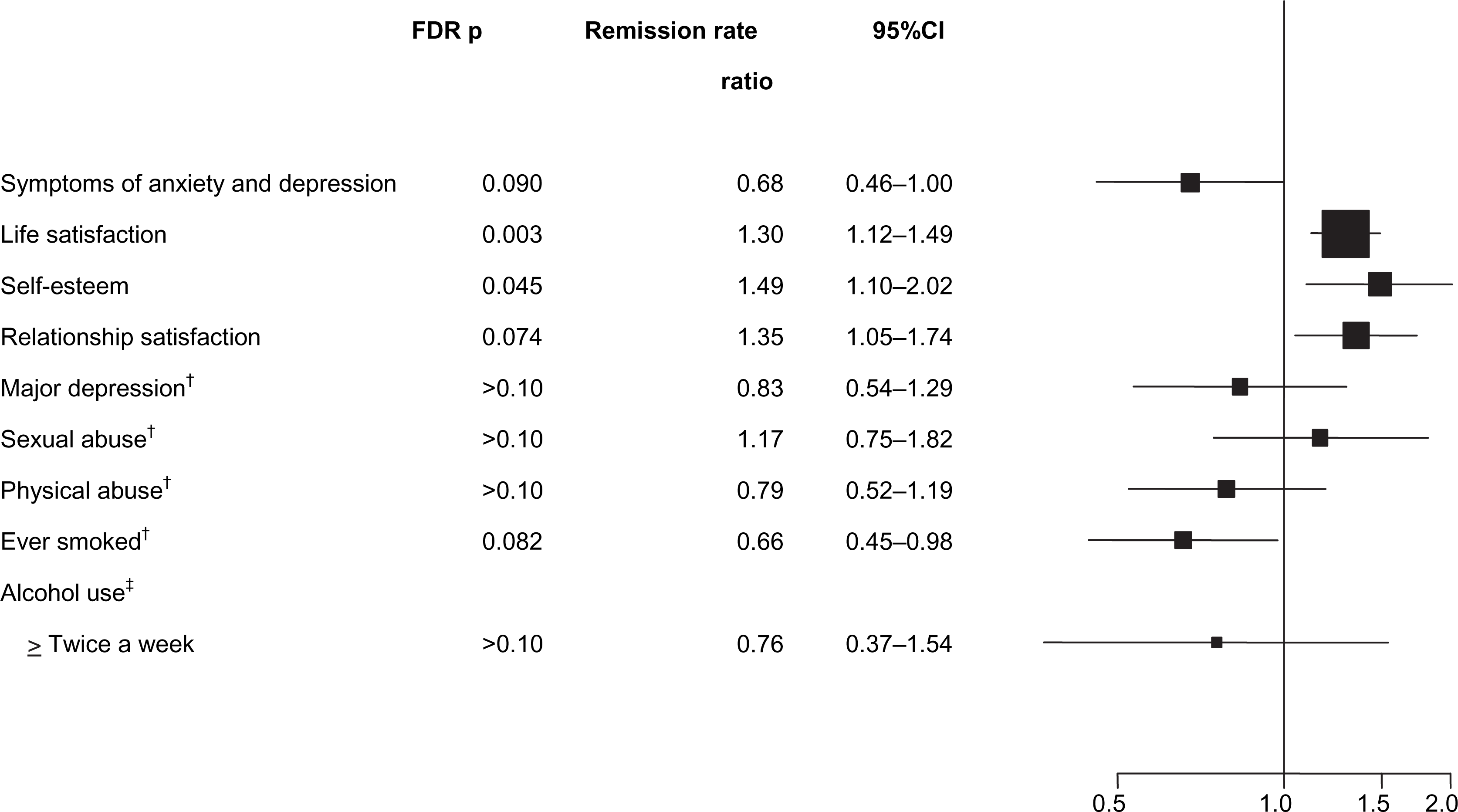
Discussion
Psychosocial characteristics associated with BN during pregnancy
To our knowledge this is the first study exploring psychosocial correlates of BN during pregnancy in a large-scale population-based sample. Compared to women without eating disorders, women who fulfilled the criteria for broadly defined BN during the first trimester of pregnancy had significantly higher rates of lifetime physical abuse, sexual abuse and major depression, and current symptoms of anxiety and depression. They also had lower scores on measures of life satisfaction, self-esteem and relationship satisfaction. These results reflect all cases of BN during pregnancy, whether continuing or incident cases.
There are no previous studies with which the present results can be directly compared. A few studies of eating disorder symptoms in pregnant women have, however, been published. In a study of 359 Chinese pregnant women, poor spousal support was associated with drive for thinness, but neither instrumental spousal support (e.g. assistance in household chores, child care and problem solving) nor emotional spousal support (e.g. nurturance and positive affect sharing) was significantly associated with disordered eating [34]. In a sample of 530 pregnant women attending an antenatal clinic, eating disorder symptomatology was associated with younger age, previous eating disorder symptoms, lower educational attainment, poorer housing, employment status, and previous miscarriage [35]. In another study based on a community sample of 10 641 pregnant women, antenatal eating disorder symptoms were associated with having been sexually abused before the age of 16 [36].
The present observations during pregnancy parallel observations of general risk factors and psychosocial correlates for BN in non-pregnant women. Significant associations have been reported between BN and lifetime physical and sexual abuse [37–39], major depression [40], low self-esteem [41], and psychological distress [42], suggesting that similar mechanisms are associated with the presence of BN both in general and during pregnancy. It is possible that women with BN who do get pregnant are less severely ill than women with BN who do not get pregnant [43].
Psychosocial characteristics associated with continuation and incidence
In a previous study of the same sample used in the present report we did not identify demographic variables associated with either continuation or incidence of BN during pregnancy [14]. Within the present report, although we identified no factors associated with continuation, incident cases of BN during pregnancy were associated with significantly higher scores on symptoms of anxiety and depression and lower scores on self-esteemd life satisfaction. This suggests that pregnant women with a psychological profile with these features may be at increased risk for BN, and professionals should be alert to this possibility. Future studies with larges samples are needed to further explore this relationship.
Psychosocial characteristics associated with remission and partial remission
In contrast, high scores on life satisfaction and self-esteem were significantly associated with remission of BN during pregnancy. Low self-esteem has previously been shown to be related to BN both in cross-sectional [44] and longitudinal studies [23], [41]. Although some researchers have found that women with low self-esteem respond more poorly to treatment [22], others have not found this association [45], [46]. Moreover, women who recovered from BN reported an increase in self-esteem [47]. Although trait-like characteristics such as life satisfaction show long-term stability, short-term fluctuation can occur [48]. The design of the present study did not enable inferences about causal mechanisms, for example whether higher self-esteem and life satisfaction increase the probability of remission from BN when pregnant, or emerge secondary to remission, or if some other common factor influences self-esteem, life satisfaction, and BN.
Limitations
The present findings must be considered within the context of several limitations. First, although the diagnostic questions used to create the BN diagnosis have been used in previous epidemiologic studies in Norway, they did rely on self-report of symptoms and targeted broadly defined BN. Face-to-face interviews are impractical in samples as large as the MoBa, although they may yield more reliable diagnostic information. Although the reliability of self-report of binge eating has been questioned [49], when assessed within the context of salient behavioural markers such as vomiting and laxative misuse (as was the case in the present study), the reliability of self-reported diagnosis of BN is equivalent to that of major depression [50].
Second, although the frequency criteria for binge eating differed from DSM criteria, neither the DSM nor our revised criteria have been extensively empirically validated [51]. Third, we have information about BN symptoms only in the first trimester of pregnancy. BN behaviours have been shown to gradually decline throughout the course of pregnancy [52], [53]. Fourth, 42% of women invited agreed to participate in MoBa. Although this response rate is low, it is typical of large epidemiologic studies and does not necessarily imply a biased sample [54]. Bias could occur if individuals who chose not to participate in MoBa differed markedly from those who did participate on the variables of interest. A comparison of MoBa to the Norwegian population suggests lower rates of preterm birth and low birthweight (<2500 g), possibly reflecting a socioeconomic gradient associated with participation [5]. MoBa participants are more educated than the general Norwegian population, with 58% attending some form of college in comparison to 46% of women aged 25–29 years and 43% of women aged 30–39 years reported to have higher education in 2005 by Statistics Norway (http://www.ssb.no/utniv_en/). Fifth, the BN status prior to pregnancy is reported retrospectively but, given the limited time delay until assessment, the impact of retrospective recall should be minimal.
Implications
Continuing and incident BN symptoms during pregnancy are of clinical concern. Given that women who have eating disorders are unlikely to report this to their obstetricians [55], detection efforts are critical. Moreover, those with BN in pregnancy may require assistance not only with BN but also with depression and anxiety – all of which have known adverse consequences for both mother and child [1], [2], [56].
In future waves of the MoBa we will investigate the role that psychosocial factors play in the course of BN after birth of the child. Most [53], [55], [57–59] but not all [52], [60] studies suggest that symptom improvement in many women with BN may be limited to the pregnancy period, and that a significant portion of these women return to eating-disorder behaviour after giving birth. Therefore it is important to be able to identify characteristics associated with increased risk of BN during the postpartum period in order to implement therapeutic measures to prevent relapse.
Footnotes
Acknowledgements
This research was supported by the National Institutes of Health Grants (HD047186) to CMB and the MoBa study is supported by the Norwegian Ministry of Health, NIH/NIEHS (grant no. N01-ES-85433), NIH/NINDS (grant no. 1 UO1 NS 047537-01) and Norwegian Research Council/FUGE (grant no. 151918/S10). The donations of questionnaire data and biological material from MoBa participants are gratefully acknowledged.