
Abstract
The interest in the topics of compliance, adherence and concordance in mental health disorders, and especially in schizophrenia, has increased substantially during the last few years [1–10]. Focusing on these issues is overdue because non-compliance is a major problem in schizophrenia [11]. Patients who did not take antipsychotic medication for relapse prevention were shown to have much higher relapse rates compared to patients who took antipsychotics [12], [13]. In patients with a first episode of schizophrenia, relapse rates were fivefold higher for those who did not take antipsychotic medication [14].
The terms ‘compliance’, ‘adherence’ and ‘concordance’ are not used consistently in the literature; some authors use them synonymously whereas others define compliance as the extent to which a person complies with medication and adherence or concordance as a wider concept, including habits and attitudes towards therapeutic strategies [15], [16]. The use of the term ‘compliance’ has been criticized by some authors as inferring an authoritarian and paternalistic attitude, whereas the concept of concordance explicitly involves mutual respect and understanding between a patient and their treating physician as well as shared decision-making in order to achieve a cooperative therapeutic alliance [17]. But the term ‘compliance’ is still common and in use. Medication compliance has often been regarded as an all-or-nothing behaviour and until a few years ago patients were either viewed as compliant or non-compliant [18]. More recently the concept of ‘partial compliance’ has emerged, acknowledging the actual, frequent situation in which a person takes some, but not all of the prescribed medication [18], [19]. Weiden et al. therefore favour the term ‘partial compliance’ over non-compliance [18]. Compliance with medication is difficult to measure and is often defined differently [16], [20]. In a recent review of the literature Velligan et al. found that compliance is often assessed by subjective or indirect methods such as patient self-report, provider report, significant other report and chart view, whereas direct or objective methods such as pill count, blood or urine analysis, electronic monitoring and electronic refill records are used infrequently [16]. For a consensus development Velligan et al. suggested the term ‘medication refusers’, those who do not accept medication; and ‘medication acceptors’, divided by degrees of adherence (those who take medication but might have adherence problems in the future). The authors stress that this is very important because ‘complete refusal may begin as a function of missed or skipped doses, either intentional or accidental’. Patients who are partially compliant or adherent according to these concepts have an increased risk of hospitalization and higher costs than those who are compliant: partially compliant patients with schizophrenia or bipolar disorder were 49% more likely to be hospitalized and incurred 55% higher inpatient charges than compliant patients [19].
The aim of the present study was therefore to provide data on the frequency of partial compliance in patients with schizophrenia using the concept of Weiden et al. [18] and to identify patient-related factors contributing to partial compliance by using a large sample size.
Methods
During a 10 day period in June 2004, psychiatrists working in hospitals or in private practices in Germany were asked to participate in a compliance survey. The participating physicians were requested to anonymously evaluate the compliance in 10 consecutive patients with schizophrenia using a questionnaire consisting of 10 questions (questions A–J, possible answers were ‘yes’ or ‘no’; Table 1) and return it by fax. The term ‘compliance’ in the present study was defined as the extent to which a person complies with the prescribed medication.
Physician responses for 5729 patients
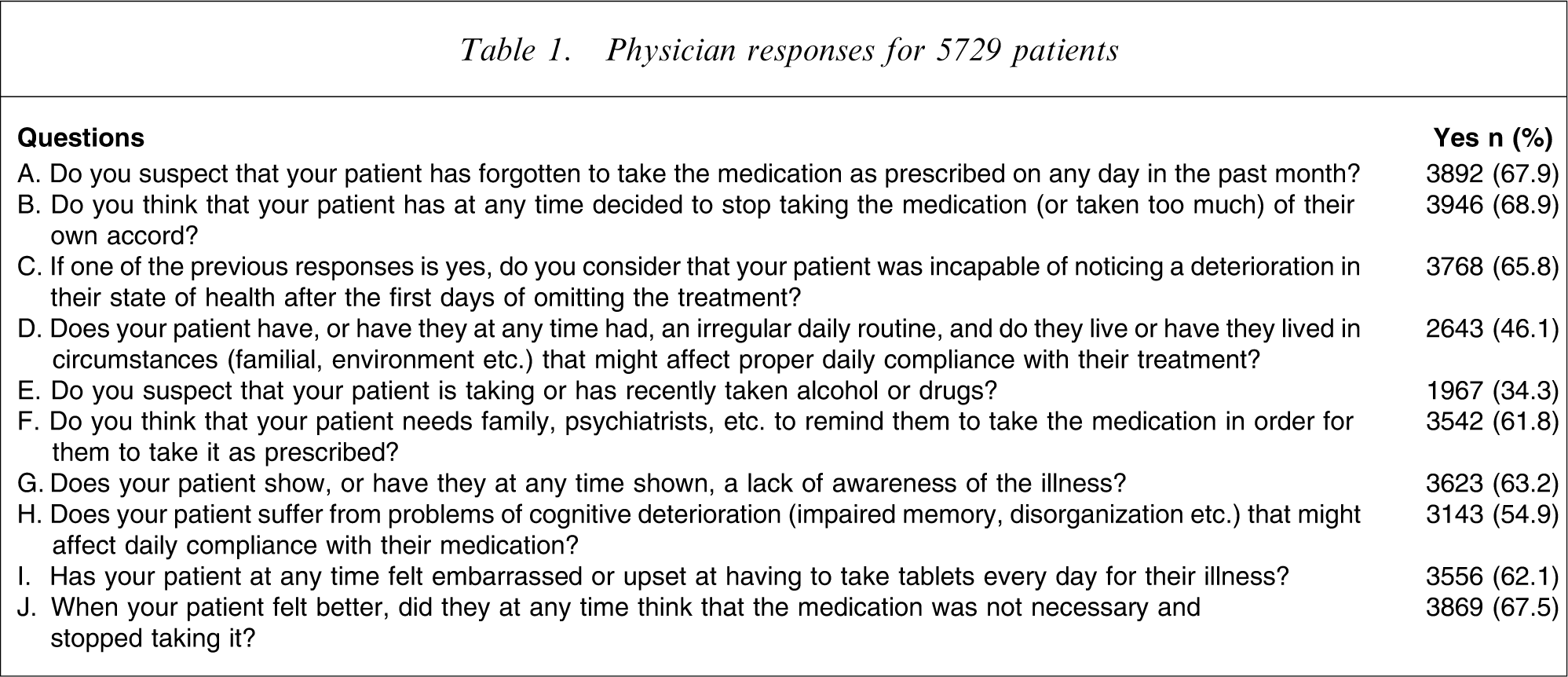
Question A assessed the frequency of partial compliance, defined as the lack of drug intake on any day during the past month; the physician was asked whether they suspected that the patient had unintentionally forgotten to take the prescribed medication on any day during the past month. Question B asked about the lifetime partial compliance and the intentional discontinuation of prescribed medication. Questions C–J were designed to evaluate the patient-related factors possibly contributing to the partial compliance: questions C and G related to lack of insight/denial of illness. Question J covered the insight into a need for prophylactic medication for relapse prevention. Problems with cognition and memory were measured with questions F and H. Question E asked about substance abuse; questions D and I covered living conditions and stigma.
Statistical analysis
Demographic data of the participating physicians were collected and responses were analysed using descriptive statistics, using SPSS for Windows, version 15.0 (SPSS, Chicago, IL, USA). Generalized estimation equation (GEE) models were used to estimate the proportion of ‘yes’ answers in the physician groups (hospital vs private practice psychiatrists). The GEE approach properly reflects the structure of repeated data and takes the correlation among patients with the same physician into consideration. The statistical software R version 2.4.1 (R Foundation for Statistical Computing, Vienna, Austria) with the GEE package was used, assuming an exchangeable correlation structure between subjects. Statistical comparisons were made at an overall level of significance of 0.05, applying Bonferroni adjustment of p for multiple comparisons.
Results
Demographic data of participating physicians
A total of 1300 psychiatrists had been asked to participate, 703 participated, and data for 699 psychiatrists were included in the analysis (participation rate 54%). A total of 396 (57%) worked in a psychiatric hospital, and 303 (43%) in private practice. Four hundred and thirty-three (62%) of the responding physicians were psychiatrists, 119 (17%) were at least in their third year of residency for psychiatry, 28 (4%) were first or second year Psychiatry residents and 119 (17%) did not specify their training.
Two hundred and seven participants did not complete the compliance assessment for 10 patients; data on the assessment of compliance are therefore available for 5729 patients with schizophrenia (Table 1).
Quantification of unintentional and intentional partial compliance
The physicians assessed that 68% of the patients had unintentional partial compliance during the last month (question A). Sixty-nine per cent of the patients were reported to have had an intentional lifetime partial compliance problem (question B).
Factors contributing to partial compliance
Of the patient-related factors possibly contributing to partial compliance, a lack of insight into the need for prophylactic medication (question J) was the most important problem (68%), followed by a lack of insight/denial of illness (66% question C, 63% question G). The psychiatrists reported that 62% of patients felt embarrassed at taking medication every day (question I) and 46% had living conditions inappropriate for compliance (question D). A total of 62% of patients needed someone to remind them to take their medication (question F). Cognitive problems were observed in 55% of the patients (question H). Substance abuse was assumed in 34% of the patients (question E).
Patients who were considered to be unintentionally partially compliant (question A) or intentionally partially compliant (question B) were statistically significantly more likely to fall in the ‘yes’ category of questions C–I than those who were considered to be compliant in questions A and B.
Differences in the assessments of hospital-based versus office-based psychiatrists
A GEE model was used to estimate the proportion of ‘yes’ answers in the two physician groups (hospital vs private practice psychiatrists) to examine whether the working situation of the physicians influenced the assessments. Psychiatrists working in a hospital chose the partially compliant/negative answers statistically significant more often in all questions except for question I, where no statistically significant difference was found (Figure 1; Table 2).
Proportions of yes answers according to question and physician group with 95% confidence intervals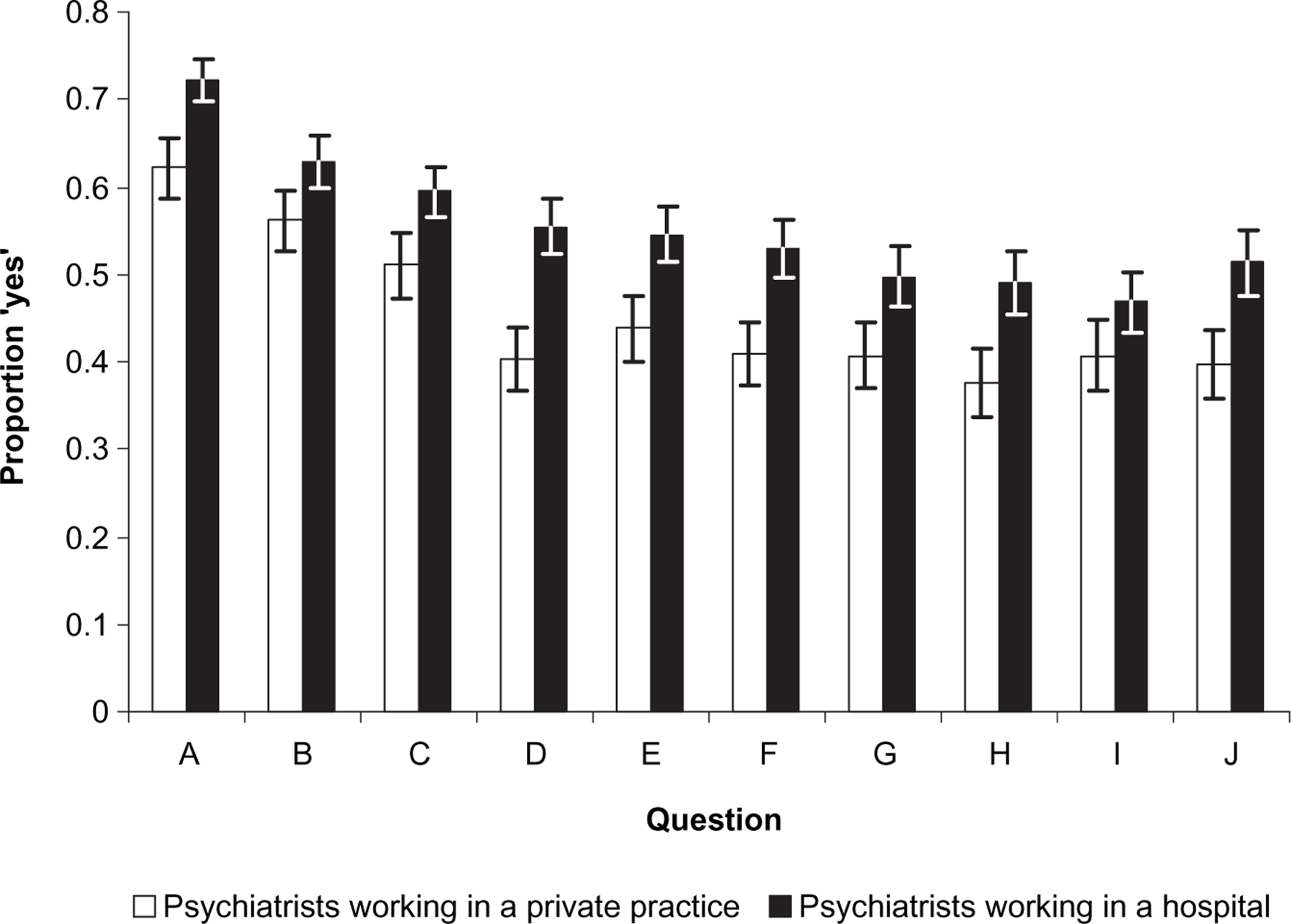
Patient assessment according to physician group
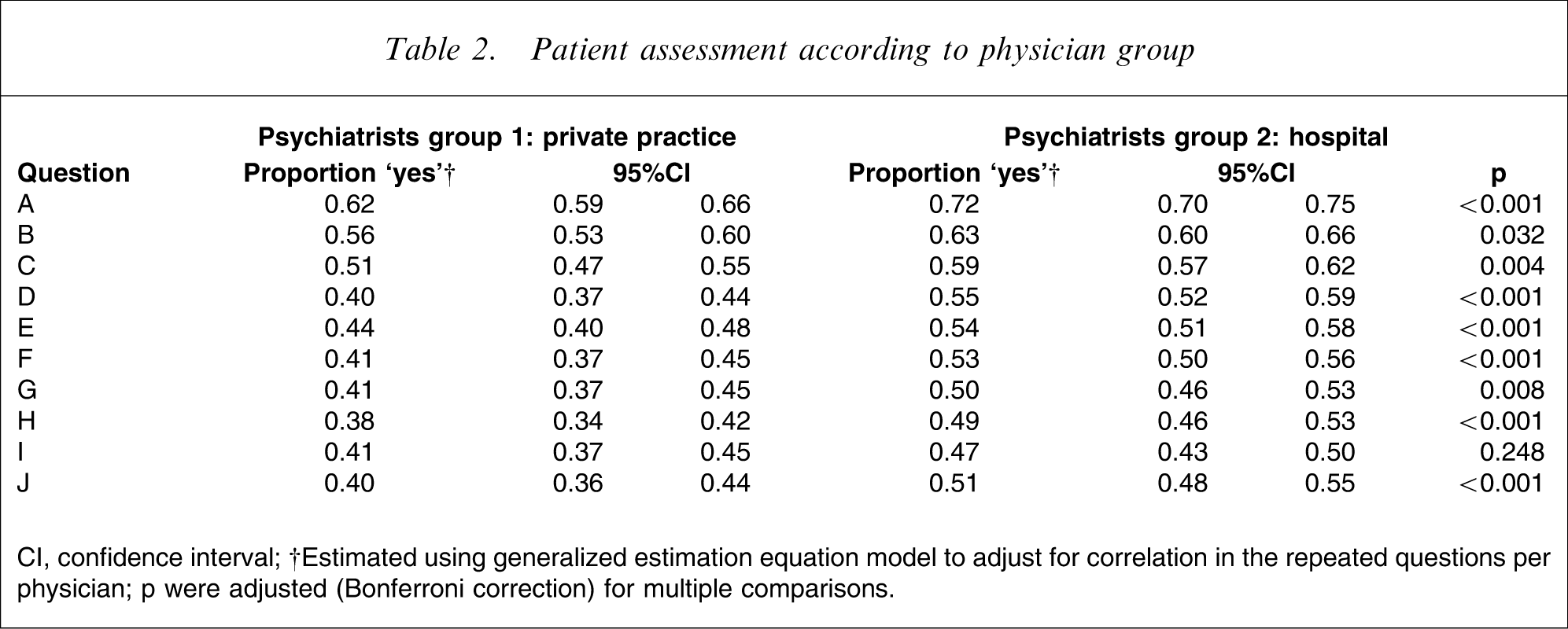
CI, confidence interval; †Estimated using generalized estimation equation model to adjust for correlation in the repeated questions per physician; p were adjusted (Bonferroni correction) for multiple comparisons.
Discussion
To our knowledge this is one of the largest surveys among psychiatrists to assess the partial medication compliance of their patients with schizophrenia [15], [21]: almost 700 psychiatrists assessed the compliance of >5700 patients with schizophrenia. According to their treating physicians, 68% of patients had had unintentional partial compliance problems in the last month and 69% had intentional partial compliance problems with their antipsychotic medication in the past. These large figures – more than two out of three patients had compliance problems – might appear high but they do not seem to represent an overestimation because physicians tend to overestimate the compliance of their own patients. A study comparing electronic monitoring and clinician rating showed that physicians dramatically underestimated non-compliance with antipsychotics [22]. Difficulties with medication compliance are considered to be one of the most important risk factors for relapse and rehospitalization among patients with schizophrenia and to cause approximately 40–50% of relapse [23–26]. Weiden et al. found a direct correlation between estimated partial compliance and hospitalization risk among patients with schizophrenia: medication gaps of only 1–10 contiguous days in a 1 year period were associated with a twofold increase in hospitalization risk, larger gaps (≥30 days) increased the likelihood of hospitalization by approximately fourfold [18]. In the present survey 69% of patients were considered to have unintentionally forgotten to take their medication as prescribed on any day during the previous month, thus showing partial compliance. When these results were extrapolated to a period of 1 year (as per the time frame in the Weiden et al. study), this 69% of patients were found to be associated with at least a twofold risk of hospitalization.
Interestingly, psychiatrists working in a hospital assessed their patients as having more compliance problems in all questions compared to the patients of psychiatrists working in private practice. These differences were statistically significant on all questions except for question I. Question I dealt with feeling embarrassed at taking medication every day, which would obviously affect inpatients and outpatients without a significant difference. A possible reason for the differences in the assessments of the patients in the other questions might be that the hospital physicians are confronted with readmissions due to relapses more often than psychiatrists in private practice. A further reason might be that patients who need to be hospitalized are generally more severely ill than outpatients in private practice.
What could be done to reduce the rehospitalization risk? Several strategies that consider the factors derived from questions C–I and possibly contribute to the partial compliance, appear promising to improve compliance.
First, telephone interventions, for example telephone reminders by case managers or families, can be helpful in assisting patients with mental disorders to regularly take their medication [27], given that the present survey showed that 62% of patients needed someone to remind them to take their medication. Second, ensuring that patients have adequate support in their environment, for example home-based cognitive adaptation training, and help for adequate living conditions, would be useful because 46% of the patients in the present survey had living conditions considered inappropriate for being compliant; therefore this intervention may contribute to improve medication adherence in schizophrenia [28]. Third, rationalizing drug regimens is a very important issue: once-daily dosage or monotherapy, whenever possible, and the use of so-called ‘dosette boxes’, where medication can be kept in daily order for 7 days so that the patient knows that they are taking the right amount at the right time, can counter several factors contributing to partial compliance that were found in the survey (environmental circumstances/living situation/cognitive problems) [29]. Another option for compliance improvement is the antipsychotic depot medication, which can also influence some of the patient factors that were found to possibly contribute to partial compliance: the need for someone to remind them to take the medication regularly, feeling embarrassed at taking medication every day, and cognitive problems [30]. Normally, long-acting agents must be administered approximately one to two times per month, thus making it unnecessary to think or be reminded of the medication every day [31], which can be helpful for those feeling embarrassed at taking medication every day – an issue markedly under-recognized by clinicians [32]. Long-acting agents allow the treating physician to identify immediately when a patient has missed a dose and can thus easily differentiate a compliance problem from an efficacy problem [29], [33], but psychiatrists are often reluctant to prescribe long-acting agents [33].
Heres et al. showed in a large survey among psychiatrists that fewer than 36% of the participants’ patients had ever been offered antipsychotic depot treatment [34]. A study by Patel et al. published in 2003 showed that the participating psychiatrists believed long-acting agents to be ‘less acceptable to patients’ (69%), ‘stigmatizing’ (48%) and ‘old fashioned’ (40%) [35]. Patients themselves, however, often do accept long-acting medication when offered by the treating physician [36] and show high satisfaction with such a treatment [37].
Fourth, psychosocial interventions, such as psychoeducation, were shown to reduce rehospitalizations. The lack of insight into the illness and into the need for prophylactic medication for relapse prevention, the factors most frequently reported in this survey as contributing to the partial medication compliance, can be positively influenced by psychoeducation [38–42]. The 7 year follow up of the Munich Psychosis-Information Study showed that patients who participated in psychoeducation had a mean number of hospital days spent in a psychiatric hospital of 75 compared to 225 days in the control group [43]. Because psychoeducation for schizophrenia is still not available in all hospitals [44], new strategies such as peer-to-peer psychoeducation [45–48] and integrating the entire treatment team into psychoeducation [42] are urgently needed.
There were three main limitations to the present survey. First, the questions focused on partial compliance rather than compliance, which might have increased the number of patients being considered partially compliant. However, as discussed, physicians tend to overestimate the compliance of their patients [22], [49]. We thus believe that our findings provide valuable real-life data on the frequency of partial compliance; the compliance studies by Giner et al. and Kim et al. found comparable, but somewhat lower, partial compliance figures of 61% and 57%, respectively [15], [21]. Second, the definition of partial compliance is very strict, namely: having forgotten the medication on any day within the last month. But, as the study by Weiden et al. showed, even short medication gaps of 1–10 continuous days in a 1 year period were associated with a twofold increase in hospitalization risk [18] and, given that Velligan et al. stressed that the complete refusal of medication may begin as a function of missed or skipped doses [16], it appears reasonable to define partial compliance in such a way. Third, not all participating psychiatrists assessed the compliance of 10 patients; therefore data are available on only 5729 patients, that is, 82% of all potentially possible patients. In order to include all available data we adjusted the calculations where necessary as mentioned in the methods section. Unfortunately missing or incomplete data are a common problem in most clinical studies, but in the present study there were no significant differences in incomplete data between the working situations of the psychiatrists.
In conclusion, the data suggest that more than two-thirds of patients with schizophrenia are partially compliant with their antipsychotic medication. Strategies to improve compliance are urgently needed.
Footnotes
Acknowledgements
This study was funded by Janssen-Cilag.