
Abstract
Introduction
Among the factors that influence the long-term outcome of schizophrenia, medication adherence is particularly important as it is potentially open to intervention [1–3]. However, despite the large number of studies that have been done in this area, much remains inconclusive about the determinants of adherence behaviour [4]. In the context of real-life clinical practice, adherence behaviour is likely to be the result of complex interactions between clinicians and patients [5, 6]. This interaction is influenced by patients' perceptions of the illness and its treatment, as well as by clinicians' evaluations of the patients' pro?les. In particular, a clinician's perception of the risk of nonadherence behaviour will determine whether the clinician will initiate more speci?c interventions, such as intensive psycho-education, family work, or depot medication.
Past studies of adherence behaviour have mostly focused on samples of mixed or chronic patients. These studies found that non-adherence rates for patients who were discharged from inpatient care were high (at least 50% after 1 year and 75% at 2 years) [7]. The most common patient-reported barriers to adherence were the stigma of taking medication, side-effects, forgetfulness and lack of social support [8]. Kampman et al. found that determinants of non-adherence included side-effects, male gender, younger age, lack of social activities, and high total score of Positive and Negative Syndrome Scale (PANSS) but with a low score on PANSS positive symptoms [9]. Agarwal et al. also found that non-adherent patients were generally younger, had a shorter duration of illness and had an episodic course of illness. In addition, they made more incorrect attributions to current positive symptoms and had a more negative subjective view of medication [10]. These ?ndings suggest that non-adherent behaviour may be more prominent among patients in the early phase of illness.
More recently, there has been an increasing awareness of a phase-speci?c approach to the management of schizophrenia [11]. By studying patients in a similar phase of the illness, such as within the ?rst few years of onset, it is more likely that patterns of behaviour and attitude related to speci?c issues pertinent to that stage are identi?ed. This approach is particularly relevant to the study of adherence behaviour as it is probable that patients' behaviour and attitude towards medication change over time. Only a few studies have been conducted on the adherence behaviour of patients who are in the early phase of schizophrenia. Coldham et al. found that in patients with ?rst-episode schizophrenia, 39% were estimated to be non-adherent and 20% were estimated to be inadequately adherent [3]. Non-adherent patients demonstrated more positive symptoms, more relapses, more alcohol and cannabis use, reduced insight and poorer quality of life. They also con?rmed that nonadherent patients were younger, had an earlier age of onset and were less likely to have a family member involved in their treatment [3]. In another study of 101 patients with ?rst-episode schizophrenia, attitudes toward medication and insight were found to contribute to medication adherence [12].
Despite its clinical signi?cance, few of the previous studies addressed the relationship between the evaluation of non-adherence by clinicians and patients' own accounts. We hypothesize that there is only a modest correspondence between clinicians' evaluations and patients' accounts. In this study, we aim to examine the relationship in a group of early patients with schizophrenia and to compare them with a group of chronic patients.
Method
Participants
A total of 484 patients were recruited from four outpatient clinics in Hong Kong (Queen Mary Hospital, Pamela Youde Nethersole Eastern Hospital, Castle Peak Hospital and Kowloon Hospital). Two of the clinics provided an Early Assessment Service for Young People with Psychotic Disorders that targeted patients with early psychosis [13]. Patients in the other two general adult psychiatry clinics had longer illness durations. All participants attended the outpatient clinics as voluntary patients (i.e. not under treatment order). Seventy-seven per cent of the patients were receiving oral antipsychotic medications, 6% were receiving depot alone, and 17% were receiving both depot and oral medications. Patients were aged between 18 and 65 years of age, and clinically diagnosed with schizophrenia, schizoaffective disorder or schizophreniform disorder. The study was approved by each hospi-tal's Institutional Review Board and all participants gave written informed consent.
Procedure and measures
Patients completed an abridged version of the Medication Adherence Rating Scale [14]. The abridged version consisted of six dichotomous items that pertained to the adherence of patients to medication behaviour and their attitudes. The ?rst two items addressed adherence behaviour (forgetting to take medication and deciding to stop medication), and the remaining items addressed adherence attitudes. We translated the questionnaire into Cantonese and carried out back-translation procedures to ensure accuracy (the Cantonese version of the questionnaire is available upon request). At the same time, the patients' clinicians completed a questionnaire on their evaluation of their patients' adherence behaviour. This 10-item questionnaire contained items that corresponded to the items of the Medication Adherence Rating Scale in the patients' questionnaire and also included questions on factors that may affect medication adherence. Other relevant information that was collected included the Clinical Global Impression (CGI) scale, duration of illness and the class of medication prescribed (i.e. either conventional or atypical).
Data analysis
Statistical analyses were carried out using the SPSS version 12.0 (SPSS Inc., Chicago, IL, US). Using illness duration of 5 years as the cut-off, the sample was divided into two groups: the ‘early group’ and the ‘chronic group’. The cut-off of 5 years was chosen because this corresponded to the ‘critical period’ after the ?rst presentation of the psychotic illness [15]. Descriptive statistics for gender, medication type (either atypical or conventional), age and CGI scores were reported in each group. Forms of adherence behaviour and attitudes of the early and the chronic groups were compared using the chi-squared test. Separate analyses were carried out for the two types of non-adherent behaviour (forgetting to take medication and deciding to stop medication). The agreement between the clinicians' evaluations and the patients' reported adherence behaviour was evaluated. We reported the sensitivity and speci?city of the clinicians' detection of the patients' non-adherence behaviour. Bayes' theorem enabled us to consider the effect of speci?c information on the probability of a particular hypothesis being correct. With the unfolding of the information, the probability of the hypothesis being correct shifts from the prior probability (before information) to the posterior probability (after information). By comparing the prior probability with the posterior probability, the impact of the information can be evaluated. Using Bayes' theorem, we considered the effectiveness of clinicians' identi?cation of non-adherence.
Results
Descriptive pro?le of the early and chronic groups
The early group (i.e. illness duration of less than 5 years) consisted of 229 patients (114 male and 115 female). The chronic group consisted of 255 patients (132 male and 123 female). The early group had a mean age of 26.21 years (SD = 8.42) and the chronic group had a mean age of 45.1 years (SD = 10.57). The mean CGI score for the early group was 2.33 (SD = 1.17), while the chronic group had a mean CGI score of 2.98 (SD = 1.23). In the early group, 47% were taking conventional antipsychotics and 53% were taking atypical antipsychotics. In the chronic group, 75% were taking conventional antipsychotics and 25% were taking atypical antipsychotics. The two groups were matched for gender (χ2 = 0.19, p = 0.663) but, as expected, differed in age (t = −21.849, p < 0.001), CGI score (t = −6.011, p < 0.001) and medication type (χ2 = 39.286, p < 0.001).
Comparisons between early and chronic patients
The patients' reports on adherence behaviour and their attitudes differed between the early and the chronic groups (Table 1). More of the early patients with schizophrenia reported that they had forgotten to take their medication or had decided on their own to stop taking medication. The two types of non-adherent behaviour (forgetting to take medication and deciding to stop medication) were relatively independent of one another in early patients (χ2 = 0.39, NS), but they tended to co-occur for chronic patients (χ2 = 8.24, p = 0.007). Signi?cantly, 38% of the early group felt embarrassed about taking medication (compared with only 22% of chronic patients, χ2 = 14.9, p < 0.001). However, most patients, and in particular the chronic patients (85%), believed that medication was bene?cial (compared with 76% of early patients, χ2 = 7.1, p = 0.008). In addition, more chronic patients (44%) felt worse without medication (compared with 34% of early patients, 2 = 4.5, p = 0.033).
Comparisons between the early and chronic groups in patients' self-reports and clinicians' evaluation of medication adherence behaviour
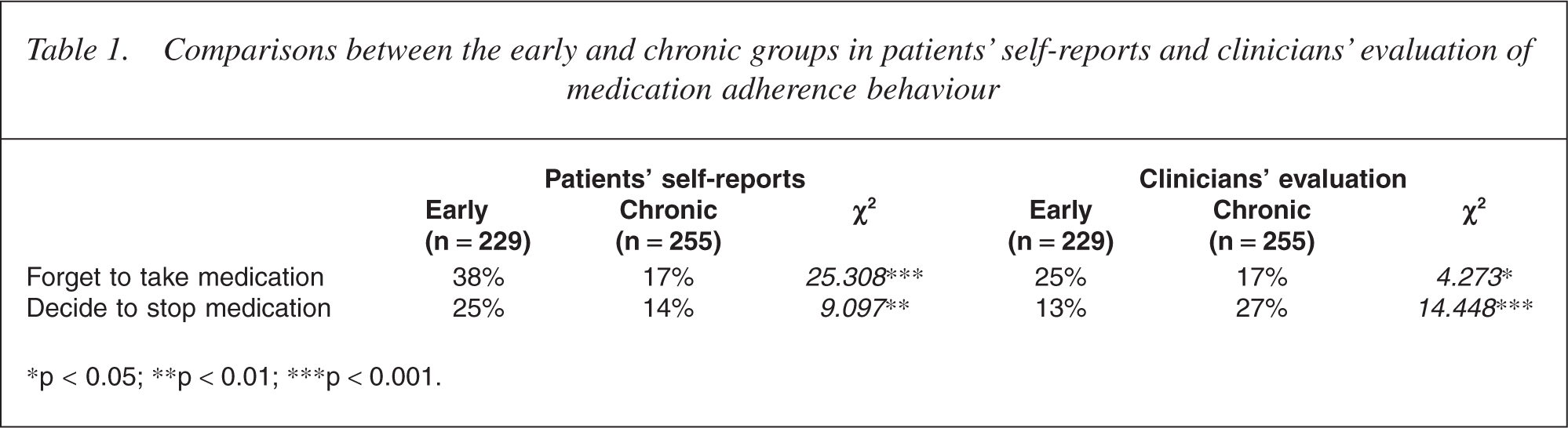
∗p < 0.05; ∗∗p <0.01; ∗∗∗p <0.001.
The clinicians' evaluations of the adherence behaviour of patients in the early and the chronic groups are compared in Table 1. More patients from the early group were considered by their clinicians to have forgotten to take medication, while more patients from the chronic group were considered by their clinicians to have decided to stop medication. Clinicians were more likely than not to consider their patients as being incapable of noticing deterioration, and this was particularly the case with chronic patients (80% compared with 65% of the early patients, 2 = 4.25, p = 0.039). A similar proportion of early and chronic patients were considered by their clinicians to have problems with irregular daily routine (χ2 = 0.39, NS), substance abuse (χ2 = 0.48, NS), the need for a reminder (χ2 = 0.17, NS), unawareness of illness (χ2 = 0.07, NS), cognitive deterioration (χ2 = 0.56, NS) and with feeling embarrassed about their medication (χ2 = 2.26, NS). Clinicians considered that more of the chronic patients would stop taking their medication as soon as they felt better (37% compared with 23% of the early patients, 2 = 11.32, p = 0.001).
Relationship between patients' attitudes towards medication and their adherence behaviour
The relationship between patients' attitudes toward treatment and their reported adherence behaviour were explored using cross-tabulations. The two adherence behaviour items (forgetting to take medication and deciding to stop medication) were analysed separately. Each adherence attitude item was cross-tabulated with the behaviour items.
Chronic schizophrenia group
‘Taking medication only when feeling unwell’ was not unsurprisingly related to both deciding to stop medication (χ2 = 28.408, p < 0.001) and forgetting to take medication (χ2 = 10.692, p = 0.001). ‘Feeling embarrassed about medication’ was related to deciding to stop medication (χ2 = 8.147, p = 0.004), but was not related to forgetting to take medication. Likewise, ‘feeling medication is bene?cial’ was related to deciding to stop medication (χ2 = 9.361, p = 0.002) but not to forgetting to take medication. However, ‘feeling worse without medication’ was not signi?cantly related to either forgetting to take medication or deciding to stop medication.
Early schizophrenia group
Notably, ‘feeling embarrassed about medication’ was signi?cantly related to both forgetting to take medication (χ2 = 6.014, p = 0.014) and deciding to stop medication (χ2 = 10.018, p = 0.002). ‘Taking medication only when feeling unwell’ was, as expected, related to deciding to stop medication (χ2 = 32.981, p < 0.001) but not to forgetting to take medication. ‘Feeling worse without medication’ was signi?cantly related to forgetting to take medication (χ2 = 6.28, p = 0.012) but not to deciding to stop taking medication. ‘Feeling medication is bene?cial’ was not related to either forgetting to take medication or deciding to stop medication.
Feelings of embarrassment and non-adherence
As many as 38% of early patients with schizophrenia reported feeling embarrassed about medication, although clinicians signi?cantly under-recognized embarrassment (21%, McNemar test, χ2 = 15.6, p < 0.001). Likewise, 22% of chronic patients admitted feeling embarrassed about medication, but clinicians felt that only 16% of those patients were embarrassed about medication (McNemar test, χ2 = 2.35, NS). We hypothesized that embarrassment was related to the decision to stop taking medication. To explore this, separate chi-squared tests were carried out on data from the early and chronic patient groups. It was con?rmed that patients who felt embarrassed about medication were more likely to stop medication, both in the early (36% vs 17%, 2 = 10.02, p = 0.002) and in the chronic groups (25% vs 11%, 2 = 8.15, p = 0.007).
Clinicians' detection of reported non-adherence
The sensitivity and speci?city of the clinicians' evaluations of patients' non-adherence behaviour (forgetting to take medication and deciding to stop medication) were further compared with patients' selfreports. If forgetting to take medication was considered, then the sensitivity rate of the early group was 0.35, which meant that clinicians were only able to identify one-third of the patients who themselves reported forgetting to take medication. The speci?city rate was 0.82: that is, clinicians correctly identi?ed 82% of patients who remembered to take medication. Similarly, the chronic group had a sensitivity of 0.3 and a speci?city of 0.86. If deciding to stop medication was considered, then for the early group the sensitivity was 0.32 and the speci?city was 0.93, and for the chronic group the sensitivity was 0.29 and the speci?city was 0.73.
Bayes' theorem on prediction of non-adherence
Using the base rate from self-reported non-adherence behaviour as the prior probability, we further explored the probability of detecting non-adherence (as reported by patients) given a piece of new information. Bayes' theorem was applied, starting with the prior probability of non-adherence behaviour (forgetting to take medication and deciding to stop medication) and arriving at the posterior probability using the additional information (patients' attitudes toward medication, clinicians' evaluation, or both).
We summated the patients' attitude item scores into a composite score and then dichotomized the score (using 2.5 as the cut-off) into positive and negative attitudes. The posterior probabilities with the additional information of the patients' attitudes towards medication were calculated using Bayes' theorem. Likewise, the posterior probabilities of non-adherence behaviour, given the additional information of clinicians' evaluation, were calculated. When patients' attitudes were revealed, the increase in posterior probability was only minimal. In contrast, when clinicians' evaluations were known, a substantial increase in posterior probabilities was achieved. This was particularly notable for detecting early patients with schizophrenia stopping their medication, with a prior probability of 0.24 increased to a posterior probability of 0.60. When both patients' attitudes and clinicians' evaluations were known, the posterior probability was further increased to 0.68. In contrast, for chronic patients, the prior probability was 0.14. Clinicians' evaluations only increase the posterior probability of detection slightly to 0.15, whereas information regarding patients' attitudes would substantially increase the posterior probability to 0.31.
Discussion
This study investigated reported non-adherent forms of behaviour and their detection by clinicians in early and chronic patients with schizophrenia. The results in the ?rst instance supported previous ?ndings of a high rate of non-adherence in early psychosis patients. Our ?nding of a nearly 40% rate of non-adherent behaviour is similar to that reported by Coldham et al. [3]. In addition, our study divided non-adherent behaviour into two types, one related to forgetting to take medication, and the other related to patients' attempts to stop medication without the clinician's knowledge. These two types of nonadherence were relatively independent of one another in early patients with schizophrenia, but tended to converge for chronic patients. Our study demonstrated that these two aspects of non-adherence had contrasting pro?les in the chronic and the early groups. These two types of nonadherence behaviour can be considered from the perspective of being organization errors and it could be argued that this perspective shifts blame away from patients and offers new possibilities for intervention [16]. According to this framework, non-adherence could be divided into intended actions and unintended actions. In our study, patients' deciding to stop medication unilaterally is considered as an intended action. Further consideration of causes for intended non-adherence should include knowledge and reasoning. Patients' forgetting to take medication is considered as an unintended action, and remedies for this should address factors such as delivery methods [16]. Nearly a quarter of the early psychosis patients in this study unilaterally decided to stop medication and more than 38% report having forgotten to take their medication. A high level of non-adherence in patients with early schizophrenia is notable, as the majority of these patients would have received extensive information about their illness and its treatment [13]. This high level of non-adherence supports the notion that adherence behaviour may not be the sole product of rational, informed, behavioural choice, but that other heuristic, social, psychological and service-related factors may interact to impact on adherence behaviour [4]. An extensive review of potential factors that took into consideration organization, service delivery and psychosocial factors would be desirable. For instance, we found that feeling embarrassed about medication was an important correlate of non-adherence. Embarrassment about medication was markedly under-recognized by clinicians particularly in early schizophrenia. This ?nding would suggest that clinicians should aim to understand more about patients' concerns about having to take medication in front of others and the practical dif?culties of being able to take their medication in private.
The true non-adherence rate was dif?cult to measure and there is no agreement regarding the gold standard for this measurement [5, 17]. While a range of electronic devices have been used in previous studies, they have been found to be effective only in measuring unintentional non-adherence. Studies of adherence have emphasized the need to take patients' perspective into consideration [6]. In this study, we have chosen to investigate patients' self-reported non-adherent behaviour. We recognize that using this method probably results in an underestimation of true non-adherence, but it is a lowburden measure that can be applied to a large sample of patients. By using a self-administered questionnaire, patients are put under less pressure to give socially desirable responses. The study results show that sensitivity was low for clinicians' detection of non-adherence behaviour, while the speci?city was high. Using Bayes' theorem, we demonstrated that the information inherent in clinicians' evaluation was more informative for early patients than for chronic patients. In addition, supplementing clinicians' evaluations with attitude measures can only modestly increase the posterior probability. Medication attitude measures are commonly used to predict adherence behaviour [18, 19]. Our ?ndings suggest that in addition to medication attitude information, clinicians' evaluations can help to inform non-adherence behaviour. In early stages of schizophrenia, non-adherence behaviour is a signi?cant clinical problem which could have profound implications for long-term outcome. Our study demonstrated that clinicians' evaluations are important in the detection of non-adherence behaviour. With effective detection, intervention to address nonadherence could be implemented [20].
Footnotes
Acknowledgements
We acknowledge partial support for this study from an unrestricted education grant from Janssen Pharmaceuticals. Thanks to the patients and staff of Queen Mary Hospital, Pamela Youde Nethersole Eastern Hospital, Castle Peak Hospital and Kowloon Hospital for their support and participation in this study.