
Abstract
Keywords
The patient was a young Palestinian man with a strong family history of schizophrenia, who was admitted in 1993 with his first psychotic episode at the age of 19. At that time he demonstrated bizarre behaviour for around 3 months, for example defecating into ice cream containers. He also believed that he was possessed by the devil, and attempted to burn down the family house with petrol. During his first admission, several typical antipsychotics all caused severe extrapyramidal side-effects. Electroconvulsive therapy (ECT) was ineffective. He eventually responded incompletely to a high dose of risperidone and was discharged after 6 months while still psychotic.
He was readmitted in 1996, after a stormy course in the community punctuated by further bizarre behaviour, non-compliance with medication and violence towards his family. After failing to respond to risperidone he was eventually given clozapine 450 mg, to which he had an excellent response, and was discharged well. For the next 2 years he was free of delusions and hallucinations, non-violent, and compliant with clozapine.
His haematology results in 1996 before starting clozapine were as follows: white cell count (WCC) 4.8×109 L−1 (normal range = 4 − 11×109 L−1) and neutrophils 2.2×109 L−1 (normal range = 2 − 8×109 L−1). During the next 2 years, on clozapine, his neutrophil count frequently fluctuated in and out of the amber range (1.5 − 2.0×109 L−1). In 1998 one neutrophil reading reached the red zone at 1.4×109 L−1 (WCC = 3.8×109 L−1), and the clozapine 450 mg was ceased. At this time his only other medication was sertraline 50 mg. His neutrophil count was again within the normal range (at 2.4×109 L−1) at the next test 3 days later.
Since 1998 the patient has spent most of his time in and out of hospital. At each hospital stay before the current 3 year admission he was either discharged while still psychotic, or absconded from a low-security ward. He has never been free of psychosis and has frequently assaulted others both inside and outside hospital.
He was readmitted in November 2004 and remained in the high-security ward for 30 months. He was continually psychotic, hearing the voices of Allah and the devil, which commanded him to punch or rape other patients and staff. He frequently asked for euthanasia, saying that no treatment worked for him, that he was constantly in fear, and wished to die. His affect was tormented. He made several serious self-harm attempts while in the high-security ward. On one occasion he jumped from a low railing onto his head and fractured his spine, his leg, some ribs and sustained a closed head injury. At another time, while unobserved in a toilet for a few minutes, he managed to fracture his tibia and fibula. He swallowed a plastic table knife, which had to be endoscopically removed.
Every few days the patient attempted to or succeeded in seriously assaulting another person. Several nurses sustained injuries, as well as significant psychological trauma. He also several times attempted to rape other patients. As a result he was placed in seclusion, where he remained continuously for more than 4 months.
His care was passed from one medical team to another every few months, due to staff burnout. The desperation of his treating teams is reflected in the medication regimens used in the 3 years of this admission. These included (i) risperidone 9 mg + lithium 1000 mg + valproate 2000 mg; (ii) olanzapine up to 70 mg + diazepam 70 mg; (iii) chlorpromazine 1000 mg; (iv) amisulpride up to 2400 mg + lithium + cyproterone acetate; and (v) bilateral ECT three times per week for 50 treatments.
Blood tests, where applicable, confirmed compliance. All of these treatments were totally ineffective for both antipsychosis and sedation.
Two attempts were made by a previous treating psychiatrist to have clozapine reinstated. One application was made to the Novartis Clozaril Patient Monitoring System (CPMS), and was refused in early 2006. A further application to the Special Access Scheme of the Therapeutic Goods Administration was also refused. The response to this application stated that ‘Overall, I consider that the haematological risks associated with re-introduction of the drug in your patient outweigh its potential benefits’. Further application was discouraged.
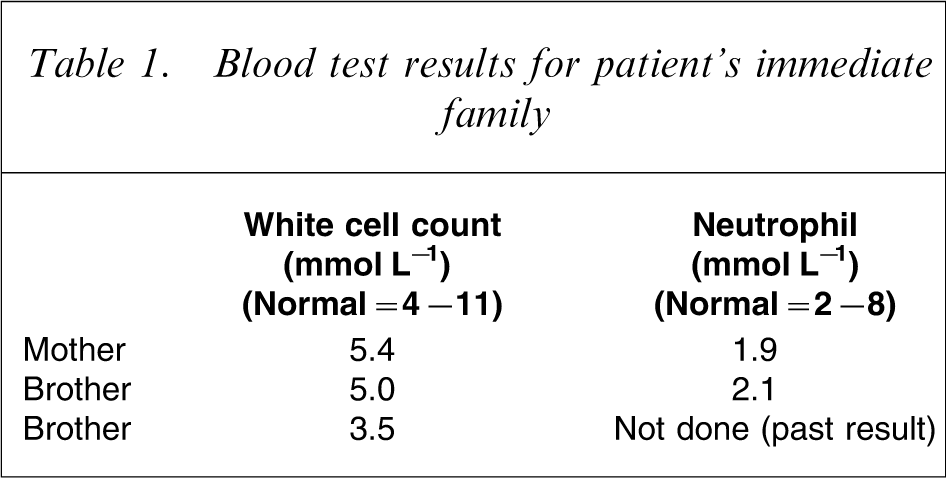
In late 2006 another change of treating team occurred, and a review of the patient's notes showed that his pre-clozapine WCC and neutrophil counts had been towards the bottom of the normal range. With that in mind, blood results were obtained from his three living family members (none taking clozapine). These results too were near or below the bottom of the normal ranges (Table 1).
Blood test results for patient's immediate family
Benign ethnic neutropenia
Benign ethnic neutropenia is a familial condition involving a retention of mature granulocytes in the bone marrow storage pool. There is no actual deficit of neutrophils overall, and immune function is unimpaired [1]. The condition has been well described in Afro-Caribbean families, for example Karayalcin et al. found that >30% of healthy black African hospital employees had low neutrophil counts [2]. A review of the literature also produced two small studies of Middle Eastern families demonstrating a similar phenomenon [3], [4].
The normal values for WCC and neutrophil counts were established in white populations, and do not reflect commonly occurring values in other racial groups [1]. Neutrophil counts in a large group of black African workmen, for example, averaged 2.3×109 L−1, compared to 4.6×109 L−1 in white workers [5]. When the ‘amber zone’ for clozapine neutropenia monitoring starts at 2.0×109 L−1, one can see how having such a low average count would place many haematologically healthy clozapine patients in this ethnic group at a disadvantage.
It then becomes very important to distinguish between clozapine-induced neutropenia, which could potentially be fatal, and benign ethnic neutropenia, which may have no deleterious effect at all except that of causing the patient to lose access to a badly needed medication.
The Maudsley Hospital Prescribing Guidelines note that the reduction in white cells seen in benign ethnic neutropenia may occur late in the clozapine treatment course (later than 6 months after commencing the drug), to fluctuate in and out of the normal range over time, and to correct itself within a few days. This can help to distinguish it from clozapine-induced neutropenia, which demonstrates an early and more decisive drop, with a slower recovery [6]. The present patient's neutropenia clearly followed the former course.
Lithium is sometimes used to increase the neutrophil count so that clozapine treatment can continue in those immunologically normal individuals who are constitutionally prone to lower WCCs. The mechanism by which lithium raises the WCC is thought to be through de-margination of existing white cells from the peripheral circulation. A serum lithium level of 0.4 mmol L−1 may be required to achieve a useful rise in neutrophils. Lithium does not protect patients from clozapine-induced agranulocytosis, and there are suggestions that it may mask a pathological, moderately low WCC. Extra vigilance with regard to infections is therefore advised. There are also case reports of neurotoxicity of even low-dose lithium, when added to clozapine [7].
Further patient management
This information was presented to the CPMS, and permission to recommence clozapine was at last given in March 2007. The dose was titrated upwards over 3 weeks to a total of 750 mg day−1. The patient remains on a low dose of lithium, chiefly for its effect in raising the neutrophil count. Certainly, the WCC results since starting lithium have all been within the normal range, including after the recommencement of clozapine. The patient's average neutrophil count is now 4.2×109 L−1, with an average WCC of 7.0×109 L−1.
The patient's violent attacks and self-harm ceased completely within 2 weeks of restarting clozapine, and he was released from seclusion. He was moved into a low-security locked ward within 1 month, and into the hospital's open rehabilitation facility after 6 months. He still sporadically reports auditory hallucinations, but his overall mental state has improved markedly, with a fall in Brief Psychiatric Rating Scale score from 97 in March 2007 to 53 in September 2007. The patient now participates in the hospital's living skills programme, and visits his family home, where his behaviour is appropriate.
Discussion
Around 30% of people of African descent have a neutrophil count below the normal range as established in white populations [2], and this is also the case for an unknown number of people from Middle Eastern races. People from these racial groups receive clozapine based on the same restrictions in terms of neutrophil counts as do white patients. Those whose normal neutrophil levels routinely fall below 1.5×109 L−1 without occasioning any increase in morbidity would thus be deprived of access to clozapine, based on racially inappropriate normative data. The present patient was eventually permitted to resume clozapine use, but the long intervening period of untreated psychosis has most likely resulted in a more treatment-resistant course and a poorer long-term outcome [8].
The Maudsley Guidelines suggest the use of lithium in these cases to provide artificial support to the patient's neutrophil count [6]. This is done, as in the present case, not to support the immune function, which is acknowledged to be normal, but to let the patient continue to meet the criteria for clozapine prescription according to the current requirements. It is anticipated that the present patient will remain on lithium for the foreseeable future because the consequences of ceasing clozapine in this patient are so serious. Thus, he must remain on a potentially toxic medication, not for his own benefit, but to satisfy a bureaucratic standard.
The immigrant population in Australia contains an increasing number of people of African and Middle Eastern descent. A total of 200 000 people from these areas have migrated to Australia since 1995 [9]. Those patients with treatment-resistant schizophrenia who, due to their race, either lose access to clozapine or are compelled to take long-term lithium to retain it, could be forgiven for viewing the current clozapine monitoring system as racist.