
Abstract
The term ‘mental health literacy’ conceived by Jorm and colleagues describes a field of research that examines knowledge and beliefs held about mental health [1]. One area of interest to researchers in this field is social distance. Social distance is the degree of proximity an individual is comfortable with in relation to a mentally ill target and it is recognized as a proxy measure of psychiatric stigma. A range of factors is believed to influence social distance including the perceived dangerousness and unpredictability of a target. Research that examines social distance can therefore provide insight into factors that may influence the stigmatization of the mentally ill.
Although improvements in public knowledge about psychiatric disorders have been reported, mentally ill persons continue to invoke strong affective reactions commonly described in terms of fear and rejection [2]. According to Angermeyer and Matschinger there is a strong relationship between familiarity with mental illness and social distance [2]. They suggest that the more familiar an individual is with mental illness the less likely they are to express negative reactions toward that individual or desire extensive distance from them. In an earlier work Link and Cullen came to the same conclusion [3]. They argued that increased contact between the mentally ill and laypersons effectively combats stigma. As a potential mitigating factor of psychiatric stigma, enhancing familiarity has therefore become a key design feature of many destigmatization campaigns [4].
A proposition forwarded by Phelan et al., however, suggests that as a result of improvements in public knowledge, laypersons now make more sophisticated distinctions between mental disorders [5]. From this view, laypersons may now distinguish symptoms associated with different diagnostic categories, which leads them to respond to such categories differently relative to social distance. Their findings indicate that lay individuals do not necessarily hold an indelible impression of the social category ‘mentally ill’. To the contrary, they suggest that the quality of attributions made by lay individuals differs in terms of whether targets exhibit symptoms consistent with neurosis or psychosis, which in tandem comes to be reflected in lay social distance judgements. Specifically, they suggest that symptoms linked to the psychiatric subcategory ‘neuroses’ will attract less social distance while symptoms linked to ‘psychoses’ will attract more social distance.
Using a vignette methodology, we investigated whether social distance evaluations correspond to the categorical delineation between psychoses and neuroses, and whether behavioural addictions attract similar or dissimilar attributions to either diagnostic subgrouping. In addition, we examined whether familiarity influences social distance appraisals across four mental disorders, namely, schizophrenia, depression, alcohol abuse, and substance dependence.
Study 1
Method
Participants
Six hundred individuals were randomly selected from the New Zealand Maori and General Electoral Rolls, and sent a detailed participant information sheet, a questionnaire (including a protocol for its completion), a consent form, and a postage paid return envelope. Of these, 435 usable questionnaires were returned, a response rate of 72.5%. The sample consisted of 276 female respondents, ranging in age from 20 years to 88 years (median = 43 years), and 159 male respondents, ranging from 18 years to 85 years (median = 47 years). Upon return of a completed questionnaire, participants were sent a $5.00 voucher for their involvement in the research and on completion of the study, participants were sent a lay summary of results.
Vignette development
Four vignettes were constructed. Each vignette described an unlabelled psychiatric case history of a hypothetical character that met the minimum DSM IV-R diagnostic criteria for schizophrenia, a major depressive disorder, alcohol abuse, or substance dependence. Indirect references were included in each vignette regarding the onset, duration, frequency, course, and severity of the specific behaviours exhibited by the respective target characters. Each character's age and sex were determined by and corresponded to the mean demographic profile for their respective disorder as reported in the available New Zealand psychiatric morbidity data [6]. To enable easy comprehension of the materials by participants the language used in the vignettes was intentionally lay-oriented and free of technical jargon.
Questionnaire development
Questions were drawn from the mental health literacy literature and included the following items: problem identification, recognition of contributing factors, quality of life, treatment preferences, likely prognosis, social burden, social distance, and familiarity. Only the social distance and familiarity items are reported here. The reason that problem identification data are not included in the reporting of this study is that it is participants’ responses to behavioural cues that is of interest and not their ability to correctly identify diagnostic labels.
The social distance measures were adapted from a scale used by Angermeyer and Matschinger [2] and required participants to rate their willingness to engage in 11 types of relationship with someone who behaved like the target character described in the vignette. Relationship types ranged from sitting next to someone on a bus to having a long-term romantic relationship. Ratings were made on a 7-point Likert scale ranging from 1, very unwilling; to 7, very willing.
Participants were also asked if they knew anyone who had experienced a mental illness and, if so, to specify the type of relationship they had with that person or persons. The scale used by Arkar and Eker [7] was adapted and used to identify 14 types of relationship covering various degrees of familiarity. The option was also made available for participants to include a relationship that was not specified in the scale. Responses were divided into three levels of familiarity. The first level consisted of relationships that had the greatest level of intimacy (e.g. family member, spouse), the second level constituted a moderate level of intimacy (e.g. acquaintance, work mate), and the third level related to a low level of intimacy (e.g. not personally knowing anyone with a mental illness).
Each participant received one of the four vignettes and an accompanying questionnaire along with a participant information sheet and consent form. Ethical approval for this study was obtained from the Canterbury Ethics Committee.
Results
Table 1 shows the mean social distance ratings for each of the four vignettes. A 2 (participant: male/female)×4 (disorder: schizophrenia/depression/alcohol abuse/substance dependence) analysis of variance (ANOVA) indicated a significant main effect for disorder, F(3,427) = 54.60, p < 0.001. Post-hoc analysis (Tukey, p < 0.05) showed that participants were more willing to engage in a relationship with someone like the character in the depression vignette than with someone like the characters in the schizophrenia, alcohol abuse, and substance dependence vignettes. No significant differences were found between the schizophrenia, alcohol abuse, and substance dependence vignettes. No main effect for sex was identified, although there was a significant interaction between sex and disorder, F(3,427) = 4.86, p < 0.005, with women more willing than men to engage in a relationship with someone like the character in the depression vignette.
Mean social distance ratings for study 1
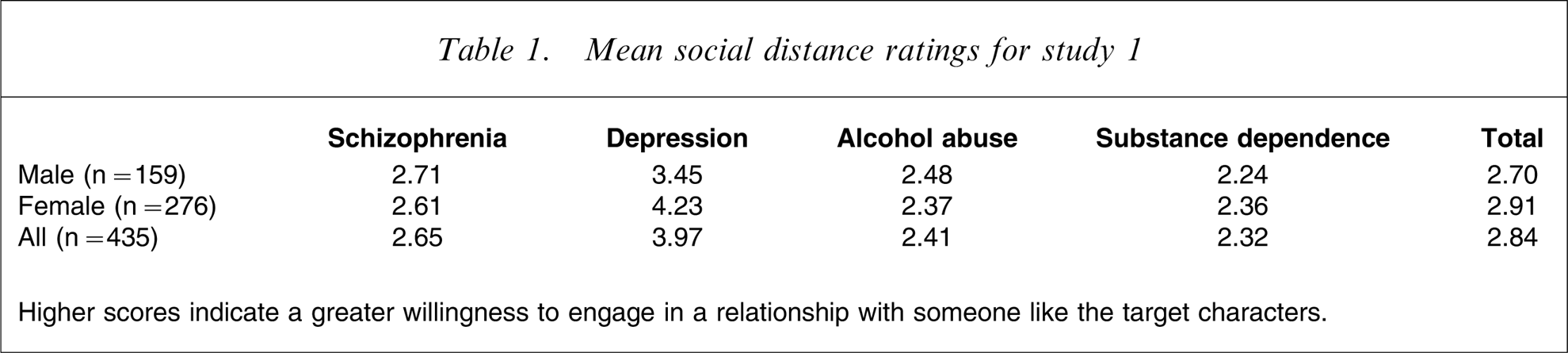
Higher scores indicate a greater willingness to engage in a relationship with someone like the target characters.
Regarding familiarity with mental illness, 52% of participants fell into the high familiarity category, 35% into the moderate familiarity category, and 13% into the low familiarity category. ANOVA indicated an effect of familiarity on social distance F(2,432) = 4.23, p < 0.02, with post-hoc analysis (Tukey, p < 0.05) indicating that participants in the high familiarity group (mean = 2.98, SD = 1.15) were more willing to engage in relationships with the target characters than participants in the moderate familiarity group (mean = 2.63, SD = 1.10). However, there was no significant difference between the high familiarity group and the low familiarity group (mean = 2.88, SD = 1.36), or between the moderate familiarity group and the low familiarity group.
Discussion
Prompted by the supposition that laypersons may now distinguish between psychiatric subgroupings and respond to them differently [5], the present study sought to examine the relationship between disorder type and social distance evaluations. The results suggest a general reluctance on the part of participants to engage in a range of relationships with any of the target characters. However, this finding was less pronounced for the target experiencing a major depressive disorder. Therefore, the tentative conclusion drawn is that laypersons do make fine-grained discriminations relative to disorder type. There are a number of viable interpretations that could account for this result.
First, depression may be viewed as a more behaviourally benign disorder due to it having stronger associations with social withdrawal and sadness. Seldom are these same characteristics linked to schizophrenia, alcohol abuse, or substance dependence. Second, participants may have had more positive exposure to depression when compared with the other disorders included in the present study. Depression is the disorder most often experienced and has received much public attention due to its increasing incidence and prevalence rates in the developed world. A third possible interpretation is that the present participants may have responded differently to the vignettes on the basis of the characters’ sex. The depressed character, for example, was female while the remaining three vignette characters were male. Although we cannot comment directly on possible effects related to the sex of our targets, evidence from a US study found that participants were more willing to interact with a female character than a male character exhibiting the same disordered behaviour [8]. To account for this result, the author concluded that either people are more accepting of individuals when their disordered behaviour conforms to their gender role, or that women are simply regarded as less dangerous and more approachable regardless of whether or not they exhibit disordered behaviour. We found that female participants exposed to the depressed fictional target were more likely to indicate a willingness to have a relationship with the character than were the male participants. Therefore, it is plausible that female subjects may not only be considered as more approachable, but may also be more inclined to approach an individual expressing symptoms of depressive illness when compared with male individuals. Of interest is that the results show no clear pattern of familiarity directly influencing social distance evaluations.
There are three main limitations of the present study. First, because of the study's design the research was restricted to undertaking a between-subjects analysis across the disorders. Second, the sample size for each group numbered around 100 participants respectively and larger samples may have produced different results. In addition, the interpretations we provide for the data are constrained by the lack of an identifiable outcome measure. Therefore, in the following study we explore one possible explanation to account for our findings, namely the influence of perceived dangerousness.
Study 2
Psychiatric stigma is widely recognized as a major impediment to individuals who experience a mental health condition. However, the term ‘psychiatric stigma’ implies that all psychological disorders are viewed similarly by laypersons. In brief, it is commonly assumed that it is mental illness generically that invokes stigmatizing attitudes toward those experiencing psychological difficulties. Results obtained from study 1 suggest that laypersons may now make more fine-grained distinctions between disorders and by doing so also respond to them differently relative to social distance judgements. This result compares to that obtained by Crisp et al. who found that in a UK sample, stigmatizing opinions varied in nature and frequency for different mental disorders [9].
It has been suggested that psychiatric stigma is influenced by a range of attributional dimensions [10–13]. Prominent among these dimensions are the attributions that laypersons make about the perceived dangerousness of a mentally ill target [9]. In the present study we investigate whether lay perceptions of dangerousness impact on social distance appraisals and correspondingly, whether these perceptions differ across diagnostic categories. As in study 1, the disorders of interest included in this research were depression, schizophrenia, alcohol abuse, and substance dependence. In addition, we report on the claim that enhanced familiarity with mental illness will lead to less social distance being desired by laypersons relative to a mentally ill target.
Method
Participants
One hundred and four individuals were recruited from the University of Canterbury campus. Three participants were omitted due to improper completion of the questionnaire, giving a final sample of 54 men, ranging in age from 17 years to 45 years (median = 20 years), and 47 women, ranging from 17 years to 45 years (median = 20 years). Participants received $5.00 in return for their involvement in the research.
Vignette
The vignettes pertaining to schizophrenia, major depressive disorder, alcohol abuse, and substance dependence that were constructed and used in study 1 were also used in this study. All participants viewed each of the four vignettes with the order of presentation counterbalanced across participants.
Questionnaire
The questionnaire administered in study 1 was again used in this study. In addition, a measure of perceived dangerousness was also included. The dangerousness measure was modified from a scale used by Penn et al. [14]. Beliefs about the perceived dangerousness of the vignette characters were assessed by asking participants to rate, on a 7-point Likert scale (1 = strongly disagree; 7 = strongly agree), to what extent they agreed with the following statements: ‘X should not be allowed to obtain a gun licence’; ‘I would think more about my personal safety if X lived nearby’; and, ‘I would be concerned if X owned a sword collection’.
Results
The mean social distance ratings for each vignette are shown in Table 2. To examine for significant differences a 2 (participant: male/female)×4 (disorder: schizophrenia/depression/alcohol abuse/substance dependence) ANOVA with repeated measures on the second factor was conducted. This indicated a significant main effect for disorder F(3, 396) = 31.69, p < 0.001. Post-hoc analysis (Tukey, p < 0.05) showed that participants were significantly more willing to engage in a relationship with someone like the character in the depression vignette than with someone like the characters in the alcohol abuse, schizophrenia, and substance dependence vignettes. Participants were also more willing to engage with someone like the character in the substance dependence vignette than with someone like the character in the schizophrenia vignette. The analysis also indicated a significant main effect for sex (F(1,396) = 4.97, p < 0.05), with men reporting more willingness to engage in relationships with someone like the target characters than women. No significant interaction effect between sex and disorder was found.
Mean social distance ratings for study 2
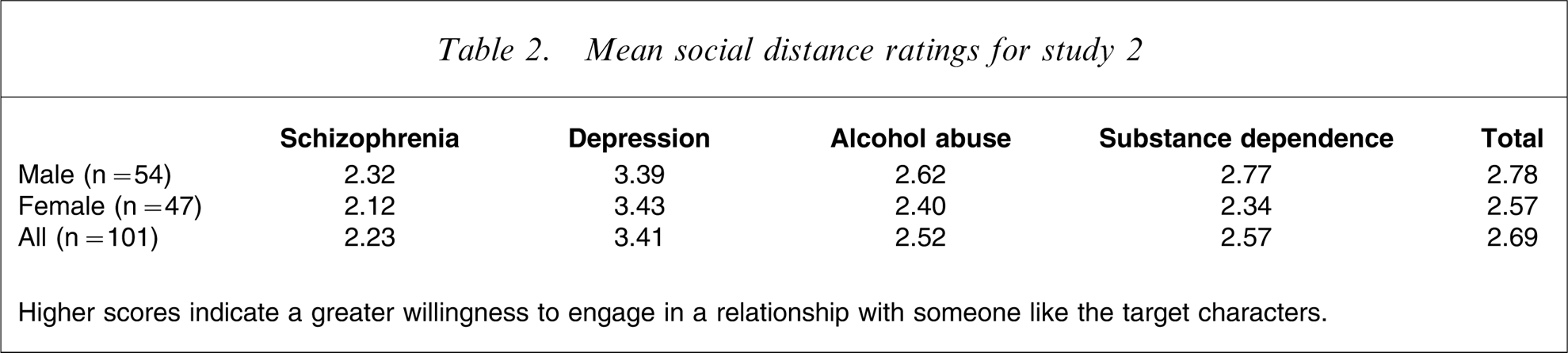
Higher scores indicate a greater willingness to engage in a relationship with someone like the target characters.
The perceived dangerousness ratings were submitted to a 2 (participant: male/female)×4 (disorder: schizophrenia/depression/alcohol abuse/substance dependence) ANOVA with repeated measures on the second factor. A significant main effect for disorder was found (F(3,396) = 24.99, p < 0.001). Post-hoc analysis (Tukey, p < 0.05) showed that the character described in the schizophrenia vignette (mean = 5.64, SD = 1.46) was perceived as significantly more dangerous than the other three characters and that the character in the alcohol abuse vignette (mean = 4.71, SD = 1.37) was perceived as more dangerous than the character in the depression vignette (mean = 4.00, SD = 1.26). No significant differences in perceived dangerousness were found between the alcohol abuse character and substance dependence character (mean = 4.49, SD = 1.51), nor between the depression character and the substance dependence character. A significant main effect for sex was found, F(1, 396) = 18.24, p < 0.001, with women (mean = 5.02, SD = 1.34) rating the characters as more dangerous than men (mean = 4.44, SD = 1.61). No significant interaction effect between sex and disorder was found.
A significant negative correlation between perceived dangerousness and willingness to engage in relationships was shown, r = − 0.41, p < 0.001. Table 3 shows the coefficients obtained from a series of regression analyses predicting social distance from participants’ perceived dangerousness ratings that were carried out to further examine this finding. As can be seen, for the schizophrenia, alcohol abuse, and substance dependence vignettes, perceived dangerousness negatively predicts social distance appraisals. That is, with the exclusion of the character in the depression vignette, participants’ perceptions of dangerousness were found to be associated with their desire for greater social distance from the target characters.
Regression coefficients predicting social distance from perceptions of dangerousness
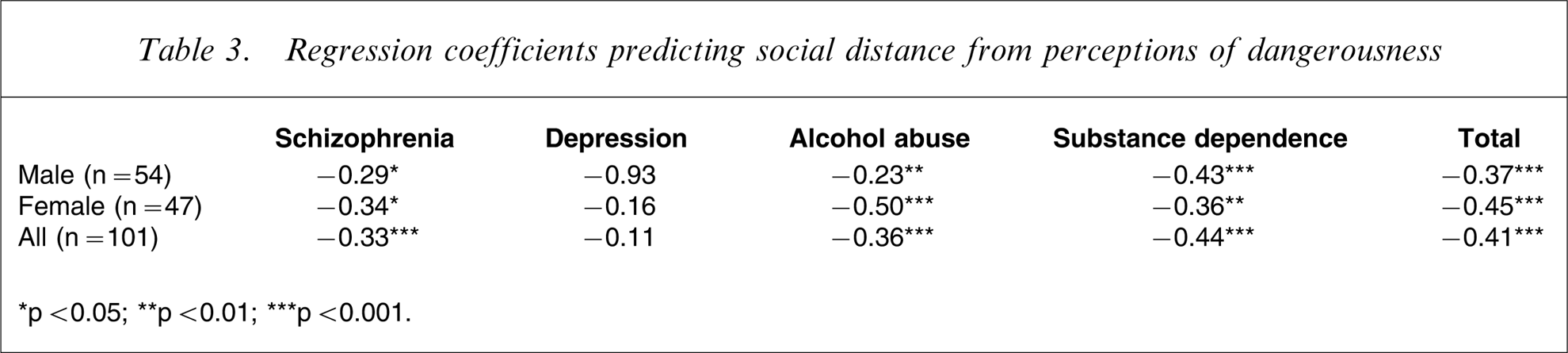
∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Given these findings, it is possible that perceived dangerousness may mediate the relationship between disorder and social distance. That is, the effect of disorder type on social distance evaluations may operate indirectly via the influence of perceived dangerousness. Figure 1 illustrates and informally examines this possibility using the logic of Baron and Kenny [15]. A more formal assessment involves estimating the indirect effect of disorder type on social distance through perceived dangerousness. Following the procedures outlined in Preacher and Hayes [16], a Sobel test found a significant indirect effect (Sobel z score = 4.17, p < 0.001) of disorder on social distance, with perceived dangerousness reducing the total effect of disorder. That is, perceived dangerousness appears to partially mediate the relationship between disorder and social distance.
Mediating effect of perceived dangerousness on the relationship between disorder and social distance. Following Baron and Kenny [15], partial mediation is held to occur when the introduction of perceived dangerousness (the mediator) reduces the direct effect of disorder type (the predictor) on social distance (the outcome). ∗p < 0.001.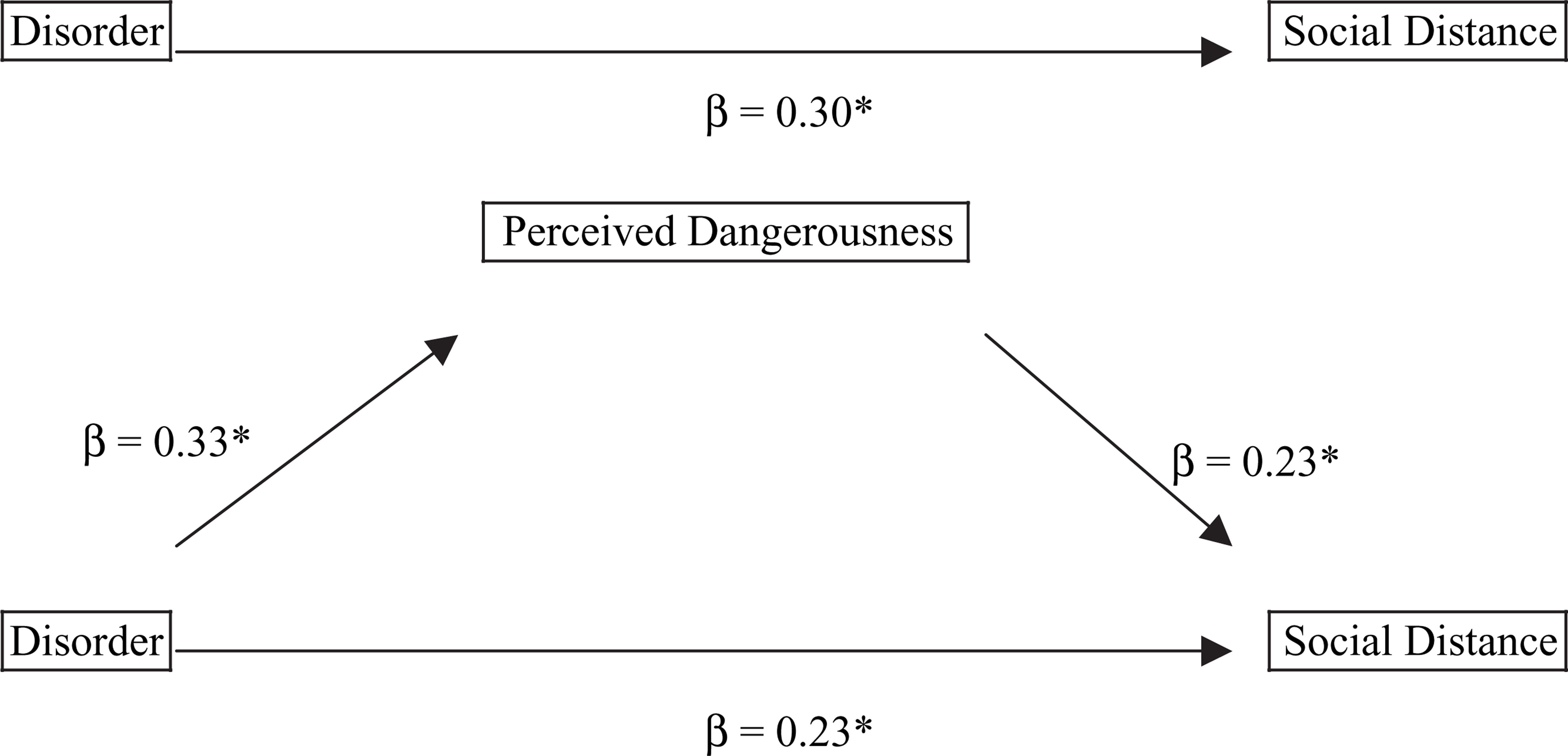
With regards to familiarity with mental illness, 39% of participants reported high familiarity, 34% reported moderate familiarity, and 27% reported low familiarity. ANOVA indicated no statistically significant relationship between level of familiarity and desire for social distance, or between level of familiarity and perceived dangerousness.
Discussion
The present findings largely confirm and extend upon those obtained from study 1. Participants were largely unwilling to engage in a range of relationships with any of the fictional characters. However, this finding was less pronounced for the depressed target and most pronounced for the schizophrenia target. We suggest that this finding provides provisional support for the Phelan et al. view that due to enhanced familiarity with mental illness lay individuals now distinguish between psychiatric subgroupings and respond to them differently [5].
To investigate this claim further, we examined whether perceived dangerousness mediates the relationship between disorder type and social distance. Analyses indicated that this is indeed the case. A relationship was shown in which higher ratings of perceived dangerousness for each of the targets corresponded to a desire for higher social distance. Of the four disorders included in this research, the schizophrenia target was judged as being significantly more dangerous than the other three targets. In turn, participants expressed less willingness to engage in a relationship with this fictional character. It would appear that laypersons are sensitive to detecting symptoms associated with psychosis and that they respond to such symptoms qualitatively differently in comparison to symptoms linked with other serious, yet non-psychotic disorders. A strong desire to avoid individuals exhibiting symptoms of psychosis and to view them as more dangerous than individuals with other serious mental health conditions appears to characterize what could be regarded as psychosis-specific stigma.
It has been well documented that the public has stronger negative views about schizophrenia than other mental disorders. However, much of this research has been limited to comparing attitudes about schizophrenia and depression [17], [18]. In the present study we have also examined stigma towards people with alcohol abuse and substance use, and have found that schizophrenia is viewed more negatively than either, in spite of the fact that these two disorders are often associated with violent behaviours [19], [20]. We now discuss this finding in more detail.
In the first instance, it is likely that laypersons have had a higher degree of exposure to depressive illness and behavioural addictions. Compared with schizophrenia, these psychological problems are reasonably common and frequently displayed within the social spectrum [21]. Because of heightened exposure, it is possible that laypersons now consider depression, alcohol abuse, and substance dependence as being within the rubric of normalcy. Conversely, schizophrenia may be perceived as being outside of the range of normalcy because it is relatively rare and therefore laypersons would have had limited exposure to the behavioural cues associated with this disorder.
Closely aligned to heightened exposure is the related factor of predictability. It is plausible that non-psychotic conditions are judged as being less dangerous than schizophrenia because they are thought of as being more behaviourally predictable. Depression, for example, is commonly characterized as a unipolar disorder involving withdrawn, passive behavioural symptoms [22], while alcohol abuse and substance dependence are more often depicted as leading to self-harm, in particular, to an individual's physical health and quality of life [19], [23].
In contrast, schizophrenia is more frequently represented as involving volatile behaviours that are unpredictable in terms of expression and outcome [17]. Therefore, schizophrenia may induce more negative reactions from laypersons because they consider individuals with this disorder as being more likely to cause harm to others. Nowhere is this characterization of psychosis more evident than in media reporting. Within the media, strong associations between psychotic conditions and acts of violence are frequently emphasized in the absence of reporting on similar acts involving alcohol or illicit substances [24], [25]. We suggest that media reporting, which highlights a relationship between psychosis and violence, may be complicit in perpetuating the message that a disproportionate number of violent acts are committed by individuals with schizophrenia. By failing to report corresponding rates of violence undertaken by individuals under the influence of alcohol or illicit drugs, the media may unwittingly reinforce psychosis-specific stigma. As a result, they may also be providing an unwarranted justification as to why in the social domain individuals with schizophrenia ought to be kept at a distance. Of interest is that contrary to the view that enhanced familiarity moderates social distance, the present results provide no evidence in support of this supposition.
Conclusion
Traditionally, much of the research reporting on psychiatric stigma has tended to treat mental illness as a generic category. Even with the advent of labelling theory, psychiatric stigma was commonly theorized as arising through adverse reactions to diagnostic labels as opposed to symptoms associated with distinct disorders [26]. The research presented investigated whether four psychological disorders were evaluated differently by laypersons with respect to social distance. The results from study 1 suggest that this was the case, and from study 2 we provided evidence that some of the variance reported in social distance judgements was mediated by perceived dangerousness.
According to Corrigan et al., the belief that individuals with mental illness are dangerous could very well be the most harmful of all stigmatizing attitudes [27]. However, this view may need to be refined. Although individuals may now be more inclined to normalize depression and behavioural addictions, concomitantly, they may also draw stronger links between schizophrenia and risk of perpetrating violence, than is warranted. A better informed public would recognize that depression is strongly associated with self-harm and suicide, the latter of which may be regarded as one of the more unpredictable human acts. Moreover, individuals experiencing addiction problems with either alcohol or illicit substances are at increased risk of being either a victim or perpetrator of violence [20].
In a seminal work, Haghighat provides an extensive critique of current interventions used to reduce stigmatization of the mentally ill [28]. Among these interventions are educational, affective, legislative, political, linguistic, intellectual, and cultural initiatives. Significantly, Haghighat cautions against the expectation that enhancing familiarity alone will moderate public perceptions of the mentally ill. The rationale provided is that stigma may present as one of humanity's basic tendencies, and given this propensity, the interventions need to be creative and continuous. This positioning we believe provides an erudite view of stigma because it helps to explain the pervasiveness of stigmatizing attitudes and also advocates an ongoing, multi-level guide to intervention.
Footnotes
Acknowledgements
This research was funded by a project grant from the Health Research Council of New Zealand. We thank Mary-Anne Mace for her contribution to this research.