
Abstract
Heavy users of psychiatric services comprise 10–30% of psychiatric patients, and tend to have psychotic illnesses often with comorbid personality disorders and drug and alcohol misuse. These patients use between 50% and 80% of service resources [1], [2] and have high levels of need [3]. More effective management of this group would reduce their use of services and free up resources for other health-care users [4].
Self-management is increasingly recognized as important in both mental and physical illnesses. Patients must learn to manage their medication and self-care activities, such as alcohol intake, sleep, diet and exercise, as well as access appropriate social support or medical care when necessary [5]. This is particularly the case with the current strategy of patient empowerment and the recovery model for mental disorders, where patients are encouraged to cope with their illness [6]. But a number of patients have difficulty managing their own conditions, leading to frequent use of services, and health professionals need to find strategies to improve self-care in these individuals.
The first step in improving patient self-care is to understand why patients may not be coping well. It has been suggested that applying social cognitive models from psychology may help to understand how beliefs contribute to variation in health-related behaviours in mental illness [7]. Furthermore, applying a theoretical framework to the assessment of beliefs in mental illness may help to provide theoretically based targets for intervention.
The common sense model of illness is a social cognitive model that proposes that patients are active problem solvers in managing their illness [8]. According to this model patients form their own cognitive representations of the illness (illness perceptions), and have emotional responses to the illness, both of which shape their coping behaviours. This self-regulatory model has been extensively researched in physical illnesses and found to predict coping behaviours such as adherence to medication, as well as health outcomes such as glucose control in diabetes and speed of return to work following illness [9]. The model has recently been found to be useful in mental disorders, such as schizophrenia [10], depression [11] and anorexia [12].
The structure of illness perceptions has been found to be similar in mental illness to that in physical illnesses, consisting of ideas about the identity of the illness (the name the patient gives the illness and the symptoms they associate with it), consequences (the perceived effects of the illness on their life), perceived causes of the illness, perceived personal control over the illness (the ability of the self to exert influence over the illness), perceived treatment control (the ability of medical treatment to exert control over the illness), and the perceived timeline (expectation about the duration of the illness) [11]. Patients’ emotional representations (the patient's emotional responses generated by the illness) and sense of coherence (how well the patient believes they understand their illness) are also measured as part of the common sense model of how people make sense of illness, and have been found to be applicable to mental illness [13]. Illness perceptions have been associated with quality of life and coping in schizophrenia, in that worse consequences scores have been found to have the strongest associations with poor functioning and quality of life [10], [13]. Together with previous research this suggests that illness perceptions may be important in determining coping responses and functioning in high users of mental health services.
Previous research has not investigated the role of illness perceptions in patients with severe mental illnesses who are high users of services and there has been no previous attempt to relate illness perceptions to needs. The assessment of needs in this group of patients has been used as a measure of outcome [14] and unmet needs are correlated with a lower quality of life [15], [16].
The aim of the present study was to assess illness perceptions in patients with severe mental illness who were also high users of services and to investigate their association with functioning, attitude to medication, visits to the general practitioner (GP), and needs. We hypothesized that patients with more negative illness perceptions would have lower functioning, a poorer attitude towards medication, more GP visits, and greater needs.
Methods
Participants
Patients were randomly selected from the database of a large survey of needs of high users of mental health services in the northern region of New Zealand [17]. Inclusion criteria were age 17–65 years, a current diagnosis of psychotic disorder (schizophrenia, schizoaffective disorder, bipolar disorder, depressive disorder with psychotic features, delusional disorder, alcohol or substance induced psychotic disorder) or personality disorder, and high service use. High service use was defined as >2 years continuous use of mental health services and/or current use of inpatient rehabilitation, inpatient forensic services, residential rehabilitation, the community intensive care team, community support work or intensive support work services; or having >28 days use or more than two admissions to acute inpatient services in 1 year.
For the present study a subsample of 1000 patients (500 Maori and 500 non-Maori) was randomly selected from the total database of 4500 patients using computer-generated random numbers. Patients’ key-workers asked patients if they were willing to take part in the study and, if they consented, an interviewer arranged an interview with the patient, usually in their own residence or local community centre. The interviewers were users of mental health services who went through 2 days training that included the Camberwell Assessment of Need (CAN) manual, interviewer skills and safety.
A total of 260 patients were interviewed, but 57 data sets were excluded because they did not have information from clinicians. Confidentiality was ensured by using only National Health Index numbers rather than names on the forms. The Auckland Ethics Committee approved the study.
Measures
As part of the large survey, background information on patient age, gender, and ethnicity were collected. District Health Board (DHB) clinical staff (trained in assessment procedures) completed the Global Assessment of Functioning (GAF), a rating of functioning developed as part of the multi-axial diagnostic system of the American Psychiatric Association in DSM-IV, for each patient. These staff also completed the CAN, a tool designed to assess the needs of people with severe mental illness across 22 domains, for each patient [18]. For each area of need a rating is given: 0 = no need; 1 = patient has a need but it is being met; 2 = patient has an unmet need; or 9 = unknown. The numbers of met, unmet and total needs are then summed for each individual.
During the patient interviews for this substudy, patients completed the CAN to assess their own ratings of need, separately from the clinic staff. Patients also completed the 10-item Drug Attitude Inventory (DAI-10), in which a positive score indicates a positive attitude towards medication [19]. Positive scores have been associated with greater adherence. To assess GP visits, patients were asked how many visits they had made to a GP in the last year (recorded as 0, 1, 2, or 3 or more).
Illness perceptions were assessed using the Brief Illness Perception Questionnaire [20]. This includes nine self-report items assessing the dimensions of the common sense model of illness. Perceptions are measured on scales from 0 to 10 and include illness identity (the extent to which the patient reports experiencing symptoms associated with the illness); timeline (how long the patient thinks the illness will last); consequences (how much the patient thinks the illness affects their life); personal control (how much control the patient feels they have over their illness); treatment control (how much the patient thinks their treatment can help them); as well as illness coherence (how well the patient feels they understand their illness); concern about the illness (how concerned the patient is about their illness); and emotional representation (how much the patient reports being emotionally affected by their illness). Causal beliefs are assessed by an open-ended response item asking patients to list in rank order the three most important factors they believe caused their illness. The questionnaire has shown good validity and reliability in a number of illnesses [20].
Statistical analysis
Data were analysed using SPSS (SPSS, Chicago, IL, USA). Data were checked for normality using the Kolmogorov–Smirnov statistic, and non-parametric tests were used when data did not meet the requirements for normality. The association of illness perceptions with attitude to medication, total needs and functioning was assessed using Spearman's rho correlation coefficients. Kruskal–Wallis tests were performed to see whether illness perceptions differed between groups based on the number of visits to the GP. Causal beliefs were assessed by coding all of the patients’ responses to the causal item into categories formed from a bottom-up assessment of the data. The frequency of responses in each category was calculated. χ2 tests were performed to analyse whether there were any differences in the number of GP visits between groups with different causal attributions. In these analyses there were no expected cell counts <5.
Results
The mean age of the sample was 40.86 years (SD = 10.59). A total of 109 of the participants were female (54%). In terms of ethnicity, 85 participants were European; 93, Maori; 11, Pacific Islander; two, Asian; and six, other ethnicities. A total of 122 patients were diagnosed with schizophrenia; 35, bipolar disorder; 30, depression; 15, substance use disorder; seven, anxiety disorder; five, other psychosis; one, organic diagnosis; 24, personality disorder; one, mental retardation; and seven, with other axis II disorders. Sixty-four patients had axis III diagnoses, indicating the presence of a general medical condition. Forty-four participants had more than one diagnosis, most commonly this was personality disorder with an Axis I diagnosis (n = 19) or schizophrenia with substance misuse (n = 9). The mean total GAF was 64.73 (SD = 14.39). Average patient-rated unmet needs were 1.98 (SD = 2.32), met needs 4.98 (SD = 2.76) and total needs 6.96 (SD = 3.55). Average DHB staff ratings for unmet needs were 1.39 (SD = 2.12), met needs 4.41 (SD = 3.66) and total needs 5.80 (SD = 4.44). Compared to the larger survey group the sample included more female subjects, more Maori, a lower proportion aged 18–35, and more living in rental accommodation, although the sample did not differ from the larger group on GAF scores or patterns of diagnosis.
The relationships between patient-rated and clinician-rated needs were analysed using Spearman correlations. The results show no association between the number of met needs rated by clinician and patient (r = 0.11, NS), a small–medium correlation between unmet needs ratings (r = 0.22, p < 0.01), and a small–medium correlation between total needs ratings (r = 0.15, p < 0.05). Clinicians’ need ratings (but not patients’ need ratings) were associated with GAF scores (met, r = − 0.38, p < 0.01; unmet, r = − 0.48, p < 0.001; total, r = − 0.55, p < 0.001). Patient DAI scores were associated with their own ratings of their unmet needs (r = − 0.17, p < 0.05), such that a more positive attitude was associated with fewer unmet needs, but DAI scores were not associated with other needs ratings.
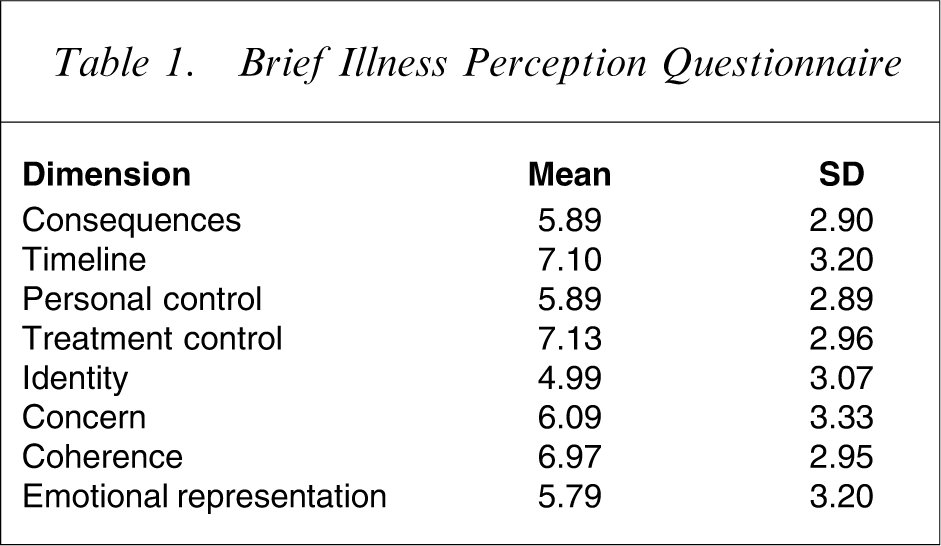
The average patient DAI score was 4.82 (SD = 4.22), which indicates a fairly positive attitude towards drugs on average. Mean scores on the dimensions of the Brief Illness Perception Questionnaire are given in Table 1. These show that on average, patients report moderate identity, consequences, emotional representation and personal control scores and high treatment control scores. They report high coherence and long timeline perceptions. Put another way, the results suggest that the average high user of mental health services experiences a moderate number of symptoms, is moderately concerned about the effect of the condition and believes that their mental health problem is likely to continue for some time. They experience some emotional distress but feel that they have a good understanding of the problem, that medication and other treatment will help to some extent and that they can exert some control over the disorder.
Brief Illness Perception Questionnaire
The associations between illness perceptions and outcomes are shown in Table 2. Patients who were rated by DHB staff to have better functioning on the GAF had higher personal control perceptions and reported lower identity scores. Consistent with this, patients who were rated by DHB staff to have greater unmet needs had higher consequences scores, lower personal control scores and higher concern. Patients with a more positive attitude to medication measured on the DAI had longer timeline perceptions, higher personal control and treatment control scores, lower concern and higher coherence. Patient ratings of their total needs and unmet needs were associated with higher consequences scores, longer timeline perceptions, lower personal control scores, lower treatment control scores, higher identity scores, higher concern and higher emotional representations.
Associations between illness perceptions, functioning, drug attitudes and needs in severe mental illness
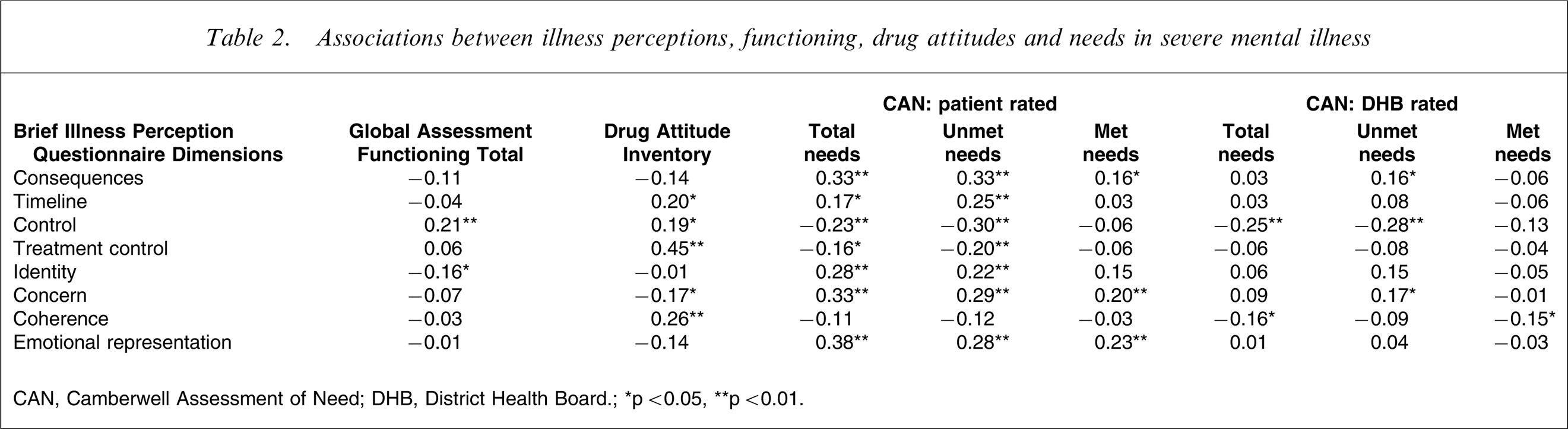
CAN, Camberwell Assessment of Need; DHB, District Health Board.
∗p < 0.05, ∗∗p < 0.01.
Mann–Whitney U-tests were conducted to test whether there were any differences in the number of visits to the GP between those who had a general medical condition (axis III diagnosis) and those who did not; results showed no significant difference (U = 3649, p > 0.05). To assess whether perceptions about mental illness were associated with the number of visits made to the GP, patients were divided into groups based on the number of GP visits they made the previous year, (no visits, n = 37; once, n = 17; twice, n = 35; three or more, n = 83), and Kruskal–Wallis tests were performed to assess whether there were any differences in illness perceptions between groups. There were significant differences between groups based on patient perceptions of symptoms (λ2(3) = 12.47, p = 0.006), concern (λ2(3) = 12.83, p = 0.005), and emotional representation (λ2(3) = 11.56, p = 0.009). Follow-up Mann–Whitney tests using the Bonferroni procedure to control for type 1 error indicated significant differences between patients who visited not at all and those who visited once on identity (Z = − 3.06, p < 0.002), concern (Z = − 2.96, p = 0.003) and emotional representation (Z = − 2.71, p = 0.007). There were also significant differences between those who visited three or more times and those who visited once on identity (Z = − 3.09, p = 0.002) and concern (Z = − 3.29, p < 0.001). Patients who reported the highest identity perceptions, concern and emotional representations, tended to either not visit their GP at all or to visit many times, while patients with more moderate perceptions visited their GP once a year (Figure 1).
Mean (SE) illness perception scores in patient groups based on the number of visits to the general practitioner (GP) made in the last year.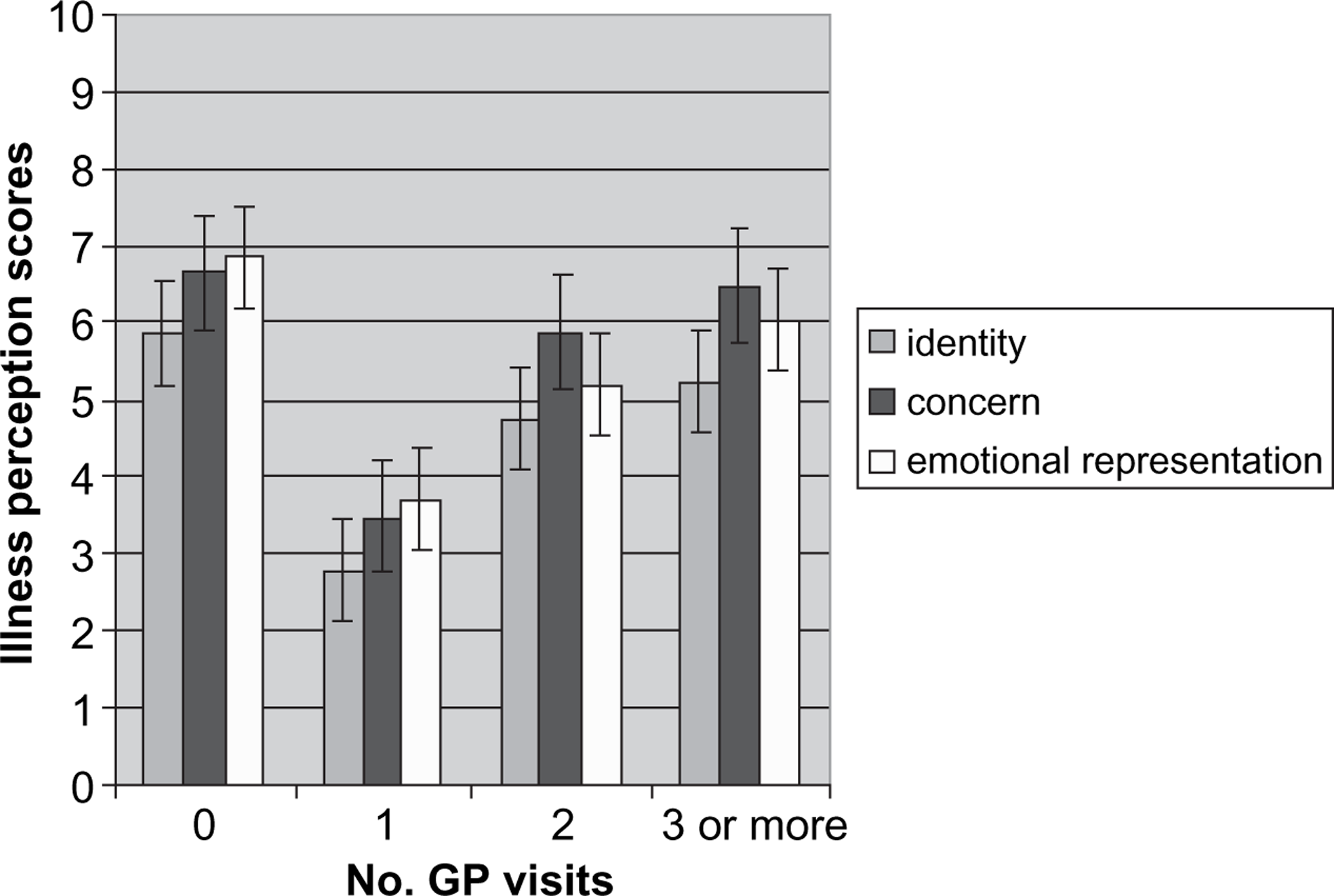
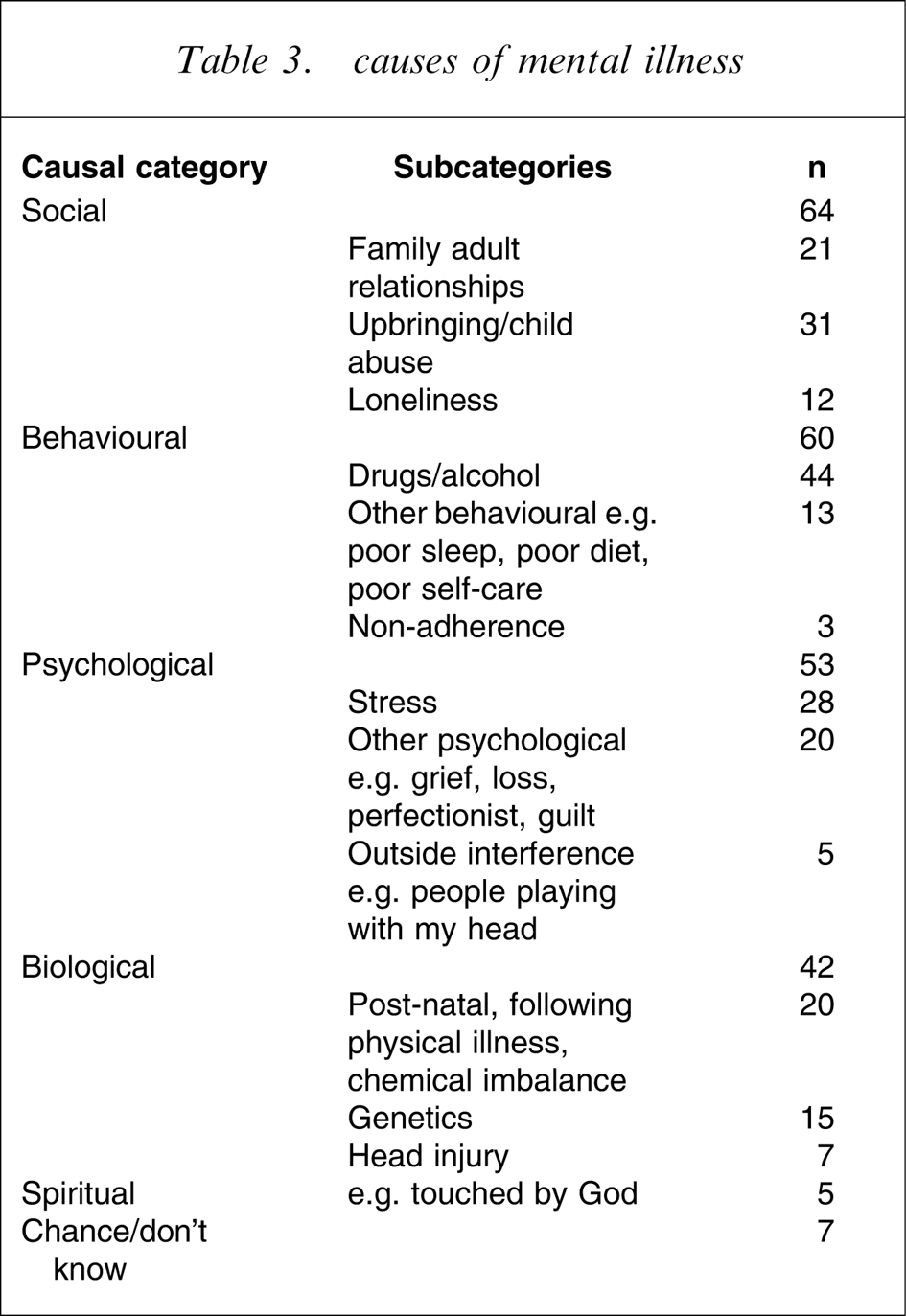
Ninety-eight patients answered the open-ended causal question. Of these, 25 patients provided one factor, 13 provided two factors and 60 provided three factors. The categories of the causal beliefs and their frequencies are shown in Table 3. Several broad themes emerged including social, psychological, biological and behavioural causes. The most common specific causes that patients attributed their illness to were drug abuse, childhood upbringing/abuse, and stress. χ2 tests were conducted to see whether the type of attribution patients had for their illness was related to the number of visits to the GP by categorizing patients’ primary causal attributions into biological (n = 23), psychosocial (combining psychological and social categories; n = 36), or behavioural (n = 27). The result was statistically significant (χ2(4) = 16.34, p = 0.003), and follow-up pairwise tests using the Bonferroni method to control for type 1 error showed that there was a significant difference between groups who made behavioural attributions (37% did not visit, 41% visited once or twice, 22% visited three or more times) and those who made psychosocial attributions (11% did not visit, 17% visited once or twice, 72% visited 3 or more times; χ2(2) = 15.57, p = 0.000). Kruskal–Wallis tests were conducted to assess whether there were any differences in needs based on patients’ primary causal beliefs. While there were no differences in patient-rated needs, there was a significant difference in clinician-rated unmet needs (χ2(2) = 6.315, p = 0.04). Follow-up Mann–Whitney tests showed that patients with behavioural causal beliefs were rated by clinicians to have greater unmet needs (mean = 2.67, SD = 3.45) than patients with biological causal beliefs (mean = 1.04, SD = 2.11; Z = −2.45, p = 0.01).
causes of mental illness
Discussion
This study provides evidence that illness perceptions can provide a framework to understand how patients who are high users of mental health services think about their mental illness. Illness perceptions were shown to be associated with patients’ needs, functioning, attitude to medication, and GP visits. More negative illness perceptions on all dimensions except illness coherence were associated with greater patient ratings of unmet needs. That is, perceptions of the mental health problem as causing more symptoms, greater emotional distress and concern, having more negative consequences, lasting for a longer time and being less able to be controlled were associated with having more unmet needs. This suggests that patients with a more threatening and less controllable view of their illness may not be managing their illness well. This interpretation is supported by the finding that higher identity scores and lower personal control scores were associated with poorer functioning ratings by clinicians as measured by the GAF. Personal control perceptions appear to be key for better coping, because they were associated with better functioning, a more positive attitude to medication, and fewer unmet needs.
The cross-sectional nature of the study does not allow the direction of causality to be directly inferred. But a prospective study by Lobban et al. found that perceptions of mental illness are significant predictors of outcome in schizophrenia [10] and those findings are similar to the present ones.
Recent research has recommended further investigation into the possible link between perceptions of treatment and adherence to medication in schizophrenia [21]. In the present study a more positive attitude towards drugs, implying greater adherence [19], was associated not only with higher treatment control scores and higher coherence, which corroborates previous work [13], but also with longer timeline perceptions, lower concern, and higher personal control scores. This suggests that to help encourage adherence, clinicians should ensure that patients understand that their illness has a long timeline, and understand that there are things that they can do personally to help control their condition. The clinician needs to check patients’ perceptions about whether medications can help control their illness, and explore patient concerns.
Understanding the pattern of health service use in New Zealand is important, both in terms of GP and specialist care [22]. In the present study visits to the GP were associated with identity perceptions, concern, emotional representations, and causal beliefs. Patients with high identity scores, high concern and high emotional representations of their mental illness either did not visit their GP at all or were frequent attendees. This suggests that these perceptions are associated with poor coping, either in terms of not taking proper steps to receive treatment when necessary, or in terms of seeking medical care too often. Previous work has also shown that high identity perceptions are associated with a high number of doctor visits in neurology, gastroenterology and cardiology outpatients [23]. Patients who had psychosocial reasons, such as childhood abuse or stress, as the primary cause of their illness were more likely to attend their GP frequently than those who attributed their illness to their own behaviour, such as drug abuse. In line with this, clinicians rated those with behavioural causal beliefs to have the greatest unmet needs. Together, this suggests that patients with behavioural attributions do not seek sufficient help for their needs.
Previous assessment of causal beliefs in mental illness has tended to ask patients to endorse the causes they agree with, using a checklist of items proposed by the investigator [13], which may not contain all patients’ ideas about the causes of their illness. In contrast, the present study used an open-ended response item in which patients could come up with their own ideas. Results showed that patient causal beliefs about mental illness could be categorized as biological, social, psychological or behavioural. This corresponds to the model of mental illness that clinicians commonly use, and the biopsychosocial model of disease. The most common causal beliefs were drugs and alcohol, childhood upbringing/abuse, and stress, which are known risk factors for mental illness. The causal beliefs that patients reported in the present study inform researchers about patients’ attributions for mental illness and should be included in any causal checklists in future studies about mental illness.
Assessing patients’ perceptions about their mental illness and discussing their beliefs may provide an opportunity to identify and alter maladaptive beliefs to improve functioning. Qualitative research has found that assessing illness perceptions in bipolar patients can be therapeutic in allowing patients to tell their story, consider new issues and clarify aspects of their illness [24]. Discussing illness perceptions with psychosis patients and their carers has also been proposed as a way to improve family relations [25]. Previous research has demonstrated that an intervention to change patients’ illness perceptions following myocardial infarction resulted in quicker return to work and fewer symptoms of chest pain [26]. The present results suggest that improving illness perceptions in patients with severe mental illness, particularly by increasing patients’ personal and treatment control perceptions, reducing consequences perceptions, and reducing emotional representations, may help to improve adherence and functioning, reduce needs and help to moderate service use.
The study has a number of limitations. While it was intended to survey 1000 patients, only 203 were included in the final sample and the sample differed from the larger survey group, which indicates a potential selection bias. The sample included more female subjects, more Maori, a lower proportion aged 18–35, and more living in rental accommodation than the larger survey group, although the sample did not differ from the larger group on GAF scores or patterns of diagnosis [17]. Another limitation was that visits to GPs were assessed by self-report rather than by medical records. The study was also limited by a low response rate to the causal question, which may be because interviewers were insufficiently trained to administer the scale. As a cross-sectional study the directionality of associations cannot be established. Future research could investigate how perceptions predict outcomes in a longitudinal study, and whether an intervention to change perceptions results in improved functioning and self-management in mental health disorders.
Footnotes
Acknowledgements
This study was funded by the Northern District Health Board Support Agency Limited.