
Abstract
Anxiety disorders are the most common psychological conditions affecting children and adolescents in the general community [1]. Untreated anxiety disorders constitute a significant burden to the health-care system [2–4] and estimates from the Burden of Disease Project suggest that anxiety disorders represent one of the most significant health problems in terms of global burden of disease, exceeding the vast majority of physical health problems [5].
If left untreated, anxiety disorders are likely to persist, and may span a chronic course into adulthood [2, 6]. Anxiety disorders can lead to a range of associated complications including severe impairment in social functioning [7, 8] and academic achievement [9], and failure to meet specific developmental tasks necessary for adult functioning such as completing school, achieving financial independence, separating from the family of origin, and becoming gainfully employed [10]. Long-term morbidity can include substance abuse [11], depression [12, 13], suicidal ideation and suicide attempts [14].
Cognitive–behaviour therapy (CBT) is currently recommended as the treatment of choice for anxiety disorders in children and adolescents [15], with demonstrated improvements on the target symptoms and sequelae [6, 16]. An essential question in this field is whether involving parents in treatment significantly improves outcomes for all anxious children. Barrett etal. demonstrated that 84% of anxiety-disordered children in their study were diagnosis free at post-treatment assessment in comparison to 57% of children who had received only received child-focused CBT [17]. At 1 year follow up 95% of the children in the family-oriented condition had no diagnosis as compared to 70% of children in the child-focused condition. Cobham etal. compared two treatment modalities: (i) child-focused CBT; and (ii) CBT for the child, plus parental anxiety management training (PAM) [18]. In addition, parental anxiety was investigated as a predictor of treatment outcome. Post-treatment and follow-up results indicated that (i) parental anxiety represented a significant risk to the successful outcome of child-focused CBT of anxious children; and (ii) the addition of the PAM component to a standard CBT programme appeared, to a certain extent, to counteract the risk factor of parental anxiety. At long-term follow up (average of 4.26 years following treatment), 69.6% of children in the CBT condition were anxiety diagnosis free versus 88.5% of children in the CBT + PAM condition (Cobham VE, Dadds MR, Spence SH: unpublished data, 2007). These results indicated that, at long-term follow up, parental anxiety (at time of treatment) no longer seemed to represent a significant risk to the successful outcome of treatment. Instead, the difference lay in whether or not the families of anxious children had been involved in treatment. Although the studies reviewed would seem to highlight the importance of involving the families of anxious children in treatment, some studies have not demonstrated significantly superior outcomes as a function of parental involvement [19, 20]. However, many of these studies did not have samples that were sufficiently large to detect differences between active treatment conditions. In addition, some studies have targeted specific types of childhood anxiety [20]. Finally, not all treatment studies have targeted parenting behaviours identified in the aetiological literature as being significant for child anxiety, and neither have outcomes always been assessed in terms of changes in parenting behaviours. In summary then, although not all studies have demonstrated significantly better effects for interventions involving parents, evidence is mounting that specific family and parenting behaviours influence levels of anxiety symptoms in children.
The cost-effectiveness of treating large numbers of young people simultaneously has generated increasing interest in the delivery of CBT in a group format (GCBT). Group treatment also presents several theoretical advantages over individual treatment including normalization, modelling, prompting, reinforcement, heightened mastery, and increased opportunities for social experience [21–23]. In contrast, parental scepticism about group treatment and fewer opportunities for therapists to tailor the treatment to young people's needs are potential disadvantages.
Recent research indicates that GCBT is efficacious in the treatment of childhood anxiety disorders [24–26]. However, only two studies have directly compared the same intervention administered individually and in a group format [26, 27]. Flannery-Schroeder and Kendall studied 37 anxious children (8–14 years) allocated to one of three child-focused conditions: ICBT, GCBT, or a waitlist control (WLC) group [26]. At post-treatment assessment 64% of children in the ICBT, and 50% of children in the GCBT groups no longer met criteria for any anxiety disorder, and children in the WLC group failed to demonstrate change. Results indicated that the ICBT and GCBT groups were superior to the WLC group. The post-treatment, 3 month, and 12 month difference in remission rates between the ICBT and GCBT conditions was not statistically significant. Manassis etal. compared ICBT and GCBT (both with parental involvement) with a sample of 78 anxious children (aged 8–12 years) [27]. Results at post-treatment and at 1 year follow up showed significant reductions in anxiety on parent, and child report measures and significantly improved global functioning. Group and individual delivery of CBT produced improvements and no significant differences were detected between conditions. That study supports the efficacy of GCBT, despite being limited by the lack of diagnostic data at post-treatment and subsequent follow-up points.
The aim of the present study was to compare the relative effectiveness of individual and group formats of the Cobham family-focused, Facing your fears and Do as I do treatment programmes for children with an anxiety disorder [28, 29]. It was hypothesized that group therapy would be as effective as individual therapy in the treatment of child and adolescent anxiety as measured by children's self-report and parental reports of their children's anxiety. It was further hypothesized that the intervention would result in diagnostic outcomes comparable to those obtained in previous studies comparing the efficacy of individual versus group CBT for childhood anxiety disorders.
Methods
Participants
Participants were 29 children (10 girls and 19 boys), ranging in age from 7 to12 years, with a principal diagnosis of an anxiety disorder. The mean age of children was 8.86 years. Study participants were recruited from referrals by parents, teachers and other mental health professionals to the Child and Adolescent Anxiety Project at the University of Queensland, Australia. The inclusion criterion was an anxiety diagnosis of clinical significance. Children with comorbid depression were included, given the high level of overlap between these disorders, providing that their primary diagnosis was an anxiety disorder. Three children met criteria for a comorbid diagnosis of dysthymia, but at mild levels of severity. Children were excluded from the study if they had significant medical problems; severe learning difficulties; if they were under treatment elsewhere (including medication), or if they met diagnostic criteria for a clinically significant non-anxiety diagnosis.
The ICBT condition consisted of 14 children (five girls and nine boys) with a mean age of 8.79 years (SD = 1.37), while the GCBT condition consisted of 15 children (five girls and 10 boys) with a mean age of 8.93 years (SD = 1.67).
Procedure
Pre-assessment telephone screening identified potential study participants. Following informed consent procedures, diagnostic assessment sessions were conducted by postgraduate clinical psychology students. Twenty per cent of all diagnostic interviews were videotaped and judged independently in order to determine interrater reliability for pre-treatment diagnoses. Two reliability interviewers were used in the present study. The diagnoses reached by the independent interviewers were compared with the original diagnoses given, and interrater reliability estimates were calculated. No disagreements occurred for any of the primary diagnoses, and thus kappa was 1.00. No disagreements among raters occurred for severity ratings assigned to primary diagnoses (where agreement is defined as interviewers being within 1 severity point of each other).
Following assessment, children were randomly allocated to the ICBT or GCBT condition. A questionnaire package containing details of which condition the family had been allocated to and parent and child self-report measures was then mailed to the family. Parents were asked to return the measures either at their first session or by post prior to the commencement of therapy.
Families in the ICBT and GCBT conditions were assessed at pre- and post-treatment, 3 month and 6 month follow-up. Assessment consisted of completion of the parent and self-report measures outlined in the following section. To assess diagnostic status at post-treatment and subsequent follow-up points, the telephone version of the Anxiety Disorders Interview Schedule for Children, 4th edition–Parent Version (ADIS-IV-C/P) was used. These interviews were conducted by a trained clinical psychologist blind to subjects’ treatment condition. As with the face-to-face interviews, interrater reliability was calculated. A total of 20% of the telephone interview transcripts from each of the three follow-up points were reviewed by a research assistant who was blind to participants’ treatment condition in order to calculate interrater reliability estimates. Across the three follow-up points the kappa for primary diagnosis was 1.00. The kappa for severity rating (where agreement is defined as interviewers being within 1 severity point of each other) was 0.95.
Measures
Structured Diagnostic Interview
The ADIS-IV-C/P is a semi-structured interview designed to determine the presence or absence of anxiety disorder categories [30]. It assesses the symptomatology and severity of anxiety disorders, mood disorders, and externalizing disorders in children and adolescents. The interview schedule has good psychometric properties, including interrater reliability (κ = 0.65–0.88) and test–retest reliability (Intraclass correlation [ICC] = 0.78–0.95) [31]. The ADIS-IV-C/P allows for the diagnosis of primary and secondary diagnoses, all of which are assigned a severity rating from 0 (absent) to 8 (severe–very severely disturbing/disabling). A severity level of ≥4 (moderate–definitely disturbing/disabling) is typically regarded as the clinical cut-off point. A minimum severity rating of 4 had to be obtained for inclusion in the study. If several diagnoses were obtained, the primary disorder status was assigned to the disorder with the highest severity score. Although parallel parent and child forms of the ADIS-IV-C/P are available, the parent version of the ADIS-IV-C/P was selected in order to allow between-study comparisons (due to the increasing use of this interview as a stand-alone diagnostic tool [26, 32]).
Questionnaire measures
At pre- and post-treatment, 3 and 6 month follow-up points, children completed the Spence Children's Anxiety Scale–Child Version (SCAS) [33]. The SCAS is a 45-item self-rated measure of how often a child experiences each anxiety symptom. The SCAS consists of subscales that reflect DSM-IV childhood anxiety disorders and yields eight correlated factors: panic and agoraphobia; separation anxiety; physical fears; social anxiety; obsessive–compulsive symptoms; somatic symptoms; worry 1 and worry 2. Spence reported high internal reliability (α = 0.92), retest reliability (0.85), and good discriminate and divergent validity [33]. Given the sample size of the present pilot study, the total SCAS was utilized after conducting reliability analyses on the individual anxiety scales (SCAS α = 0.847).
The parents completed the Strengths and Difficulties Questionnaire–Extended Version (SDQ) [34, 35] and a Family Demographic Form that provided parental education and occupation details.
The SDQ is a parent-report measure of psychopathology in children and adolescents aged 3–16 years. The scale consists of 25 items on a 3 point scale and generates five scale scores (Emotional Symptoms, Conduct Problems, Inattention/Hyperactivity, Peer Problems and Prosocial Behaviour) and a Total Difficulties Score. The Total Difficulties score has adequate internal reliability (α = 0.76) [36] and test–retest reliability (r = 0.85) [35]. The extended version assesses whether the parent thinks the child has a problem, and if so, the perceived impact on the child and burden on the family (rated on a 4 point scale). The SDQ has also been increasingly used in treatment outcome research with this population [31]. In the present study the SDQ Emotional Symptoms Scale (SDQ-Em) was used as a parent measure of child anxiety. It has been shown to have adequate internal reliability (α = 0.73) and good test–retest reliability r = 0.62 [37].
Treatment programme
Both the individual and group treatment conditions used the same integrated 12-session manualized CBT programme. The parent component of the intervention consisted of six parent-focused sessions as outlined in the Do as I do programme parents workbook [29] designed to accompany the child workbook. The child-focused component of the programme consisted of the six sessions outlined in the Facing your fears programme children's workbook [28]. The parent programme was run first followed by the child programme. One booster session took place approximately 3–4 weeks following completion of the child programme. The booster session provided an additional opportunity for children to practise the skills learnt in the previous sessions and to facilitate the generalization of these skills.
A total of three groups were run with 5–6 children in each group. Regardless of treatment condition the sessions were 60–90 min in duration, and sessions were generally weekly. Treatment sessions were conducted by the first author and postgraduate intern psychologists under the supervision of the second author. All groups were conducted with two psychologists. Fortnightly supervision sessions addressed any difficulties in implementing the programme. A randomly selected 20% of the therapy sessions were audiotaped. A research assistant who was unaware of each family's treatment condition reviewed the audiotapes and completed a treatment integrity checklist. This enabled session content between and within conditions to be reviewed for consistency, and to be confirmed for treatment integrity.
At least one parent from each family was required to attend each parent session, and the same parent was requested to attend all six sessions. In the majority of cases (90%), mothers attended the parent sessions. The therapists emphasized the importance of discussing session content with the partners who were unable to attend. The programme emphasized that the coping strategies taught, needed to be practised as a family on a daily basis.
A fundamental aim of the Do as I do programme (parent) was to explore the potential role the parent/s may play in the development and maintenance of their child's anxiety disorder. Sessions involved psychoeducation, teaching parents awareness and management of their own anxiety responses, and modelling appropriate anxiety management strategies to their children. Finally, parents were taught to reinforce their child's brave, non-anxious behaviour through cognitive restructuring, relaxation training, graded exposure, and problem solving.
The goal of Facing your fears programme children's workbook was to teach children a two-step plan for overcoming anxiety: helpful thoughts and ‘brave behaviours [28]. Helpful thoughts involved learning to identify thoughts; understanding the role of thoughts in anxiety; learning to apply a scientific approach to evaluate thoughts; learning to generate alternative, more realistic thoughts; and coping self-talk. Brave behaviours involved learning about the role of avoidance in maintaining anxiety, and the completion of parent-assisted exposure tasks.
Regardless of treatment format, child sessions began with a 10 min conjoint meeting with children and parents to outline session content, review homework activities and monitor progress. Parents were invited back for the last 5 min of the child session to discuss new homework and practise strategies for the coming week. In the group condition, when sessions were missed, parents were asked to catch up individually and attend group early on the subsequent week to address any questions arising from the content.
Statistical analysis
The child and parent questionnaire data were analyzed in two stages, first from pre- to post-treatment time-points to investigate immediate treatment effects; and then across post-treatment, 3 month and 6 month follow up to investigate the maintenance of any effects over the follow-up period. Repeated measures multivariate analysis of variance (MANOVA) was performed to investigate treatment condition differences in the child self-report and parent report measures of child anxiety symptoms. Two dependent variables were used: SCAS-Total and SDQ-Em. The independent variables were treatment condition (group or individual) and time (pre-treatment, post-treatment, 3 and 6 month follow up). The analysis examined the questionnaire data for a within-subjects interaction effect, a main effect, and univariate effects. Preliminary assumption testing was conducted to check for normality, linearity, univariate and multivariate outliers, homogeneity of variance–covariance matrices, and multicollinearity, with no serious violations noted. Statistical significance was set at the usual 0.05 level.
Results
Of the 29 children, 55.2% of children had a primary diagnosis of generalized anxiety disorder (GAD; n = 16); 17.2% had a primary diagnosis of social phobia (n = 5); 10.3% had a primary diagnosis of separation anxiety disorder (SAD; n = 3); and 17.2% had a primary diagnosis of specific phobia (n = 5). The mean severity level of the primary anxiety diagnosis was 6.93 (SD = 0.88), while the mean number of anxiety diagnoses per child was 2.86 (SD = 0.95). Ninety-three per cent of children met criteria for a secondary comorbid anxiety disorder (41.4% GAD; 31% social phobia; 10.3% SAD; 10.3% specific phobia). Sixty-five per cent of children met criteria for a third anxiety disorder (17.2% social phobia; 20.7% SAD; 20.7% specific phobia; 3.4% panic disorder; and 3.4% agoraphobia without panic).
Pre-treatment comparisons
There were no significant differences across conditions for any sociodemographic variables including child's gender or age, parents’ age, education or occupation. The two treatment groups did not differ significantly on any of the diagnostic variables, specifically: the total number of diagnoses; the severity of the primary diagnosis; and the percentage of children with each of the other disorders as their primary diagnosis. There was no significant difference between the treatment groups on pre-treatment child-report or parent-report measures of child anxiety.
The 29 children came from a total sample of 31 participants (one child from each condition dropped out of treatment). There were no significant differences on any of the measures between families who completed the programme and those who did not. Data on dropouts were not included in the analyses. Of the remaining 29 families, the participants in the individual condition attended on average 94% of all sessions, whereas the participants in the group condition attended on average 86% of all sessions.
Treatment effects: diagnostic status
All of the 29 participating families completed the telephone ADIS-IV-C/P interview at each of the three follow-up occasions. Descriptive statistics on diagnostic status and the severity of primary diagnosis at pre-treatment and post-treatment assessment, 3 and 6 month follow up are presented in Table 1.
Diagnostic Information
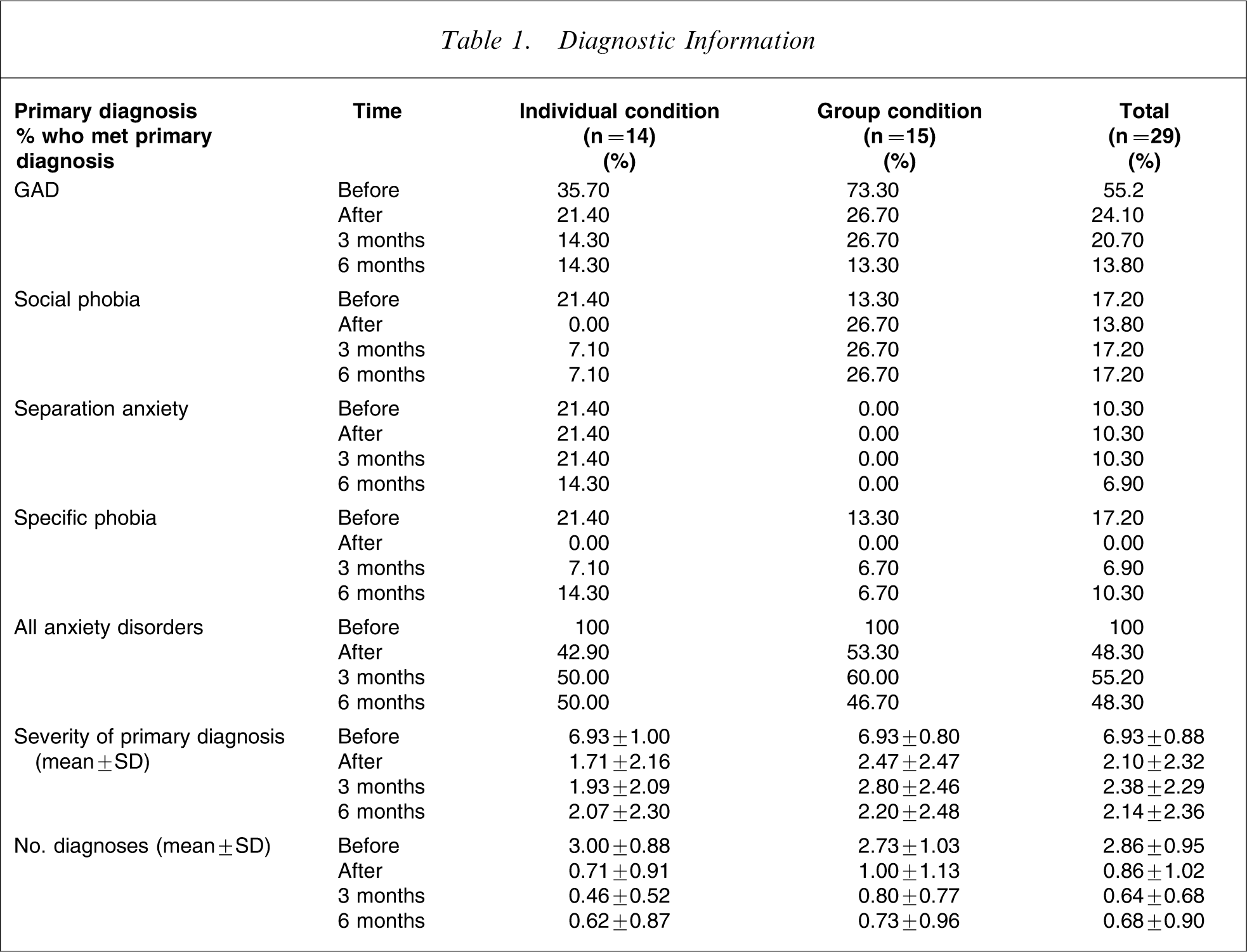
At post-treatment assessment the percentage of children who were free of a DSM-IV diagnosis did not differ significantly according to whether they had been assigned to the individual or group treatment condition (χ2 (1,n=29)=6.56, p = 0.07). In the ICBT condition eight of the 14 children (57.10%) no longer met diagnostic criteria for an anxiety disorder at post-treatment assessment compared with seven out of 15 children (46.70%) in the GCBT condition. At 3 month follow up the difference between treatment groups continued to be non-significant, with 50% of children in the ICBT condition being diagnosis free compared to 40% of children in the GCBT condition (χ2 (1,n=29) = 5.22 p = 0.26). Similarly, at 6 months there was no difference between the diagnostic status of children in the two conditions, with 50% of participants in the ICBT condition and 53.30% of participants in the GCBT condition being diagnosis free (χ2 (1,n=29) = 3.87 p = 0.44).
Severity of primary diagnosis
The means and standard deviations of the severity ratings of primary diagnoses across the two treatment conditions before treatment and at each of the follow-up occasions are shown in Table 1. Post-treatment results show a highly significant change in severity ratings of primary diagnosis over time for children in general (F(1,27) = 122.09, p < 0.001). No main effect was found for treatment condition (F(1,27) = 0.60, p = 0.45), and there was no interaction effect between treatment condition and time (F(1,27) = 0.73, p = 0.40). From post-treatment assessment to 3 month to 6 month follow up there was no significant change in severity ratings for children's primary diagnosis in general (F(2,26) = 0.24, p = 0.79), suggesting that pre- to post-treatment reduction in diagnostic severity was maintained across follow up. Again, no significant effect was found for the between-subject variable of treatment condition (F(1,27) = 0.73, p = 0.40), nor were there any interactions between treatment condition and time (F(2, 26) = 0.52, p = 0.60).
Child and parent questionnaire data
Of the 29 participating families, the majority completed all of the questionnaire measures at each of the four assessment occasions (at the three follow-up points the number of families who returned all questionnaire measures was as follows: post-treatment assessment, n = 29; 3 month follow up, n = 25; 6 month follow up, n = 26). Given this high return rate, missing data were replaced with the respective condition mean. Descriptive statistics for the SCAS and SDQ-Em are presented in Table 2.
Child self-report and parent-reported anxiety questionnaire measures (mean±SD)
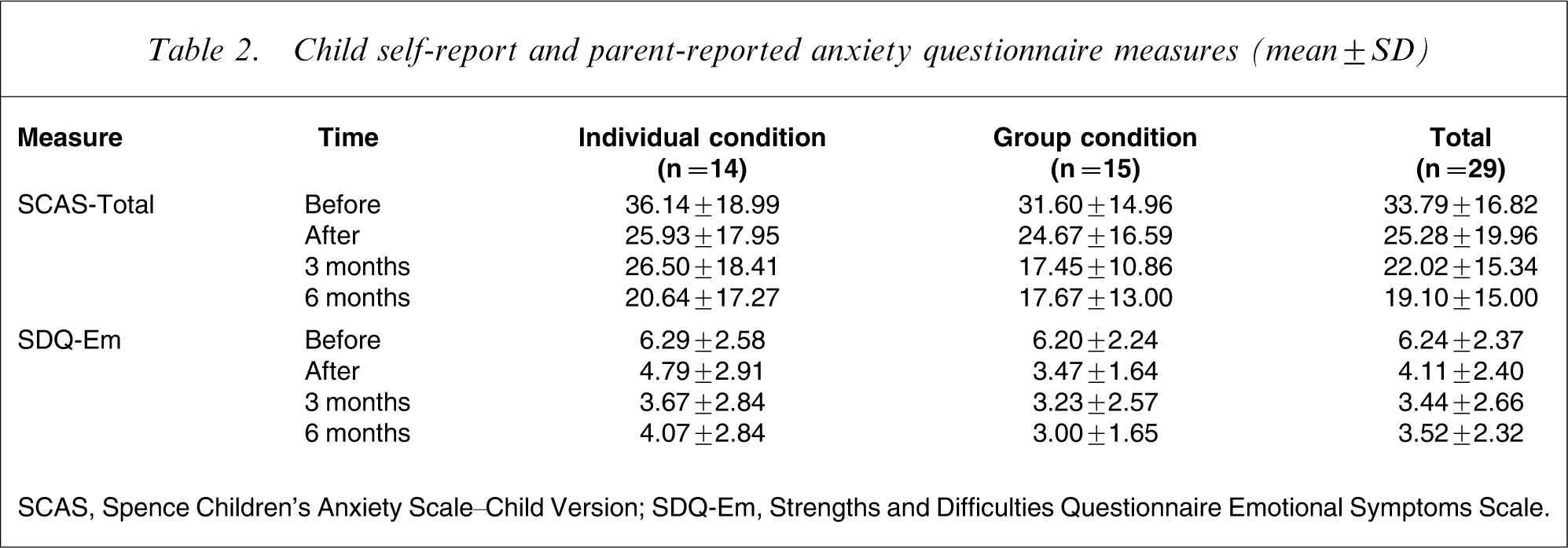
SCAS, Spence Children's Anxiety Scale–Child Version; SDQ-Em, Strengths and Difficulties Questionnaire Emotional Symptoms Scale.
From pre- to post-treatment assessment there was a highly significant change in self-reported anxious symptomatology over time for children in general (Phillais F(3,25) = 0.59, p < 0.0005). Univariate ANOVAs indicated that there was an effect for time for both questionnaire measures. There was a significant reduction over time for the total anxiety scale of the SCAS, F(1,27) = 19.36, p < 0.0005, and the total emotional scale of the SDQ as rated by the parents, F(1,27) = 25.84, p < 0.0005. A trend emerged for children across conditions to report lower scores on the SCAS at post-treatment compared to pre-treatment assessment, and parents rated similar reductions in their child's anxiety symptomatology. No significant effect was found for the between-subject variable of treatment condition (F(3,25) = 0.06, p = 0.70), nor were there any interactions between treatment condition and time (F(3,25)= .15, p = 0.24).
Discussion
Anxiety is a significant problem among children and adolescents, and the majority who experience this problem do not receive professional help [38]. The present pilot study compared the effectiveness of delivering treatment in a group and individual format. The study results demonstrate that children who received the family-focused CBT intervention in either group or individual format reported significant and marked improvement over time. No difference was detected between treatment conditions in the percent of children who recovered from their anxiety disorder. The effects were of clinical significance as indicated by a reduction in the percentage of children in the treatment conditions who had a clinical diagnosis of anxiety at post-treatment assessment. In children who did retain a diagnosis at post-treatment assessment, the severity was significantly reduced from before to after treatment. Such improvements were evident for children across group and individual treatment formats. Further, measured by positive case status for an anxiety disorder, treatment effects were maintained at 3 and 6 month follow up for children who had received treatment in either GCBT or ICBT format. There were trends for further reduction in anxiety symptoms from post-treatment assessment to the 3 and 6 month follow ups.
The benefits of the trialled interventions were in keeping with previous publications. Flannery-Schroeder and Kendall reported that 64% of children in the ICBT condition no longer met criteria for any anxiety diagnosis after treatment compared to 50% of children in the GCBT condition [26]. Direct diagnostic comparisons are not possible with the Manassis et al. study because no post-treatment diagnostic information was collected [27]. However, on measures of anxiety symptoms the Manassis et al. findings [27] compare with the present study. Contrary to the present results there was a trend for superior results for the ICBT in the Flannery-Schroeder and Kendall study [26].
There are a number of limitations related to the present study, most of which were due to the practical constraints associated with conducting a pilot study. The most important of these is the small sample size: the present study was under-powered to test for small to moderate effect sizes between the treatment groups. The absence of a control group also represents a significant limitation of the study. However, in examining the literature there is a clear consensus that waitlist control groups do not tend to demonstrate improvements from the pre- to post-wait assessment point. In addition, the generalizability of the results to other clinical populations is valid only for presentations with a primary anxiety disorder, with or without comorbid depression. Further, study participants were not recruited from a generalist child and adolescent mental health setting, but rather within a university clinic. Finally, the use of the parent version only of the ADIS-IV-C/P is also a limitation of the present study, given that standard practice involves administration of both the parent and the child version. However, as indicated above, practical constraints meant that this was not possible in the present study.
In conclusion, the present pilot study provides preliminary support for the efficacy of the integrated family-focused CBT programme described in this paper, whether delivered either individually or in a group format. The hypothetical advantage offered by group delivery of the programme was not found to add significantly to the effectiveness of the treatment itself. On a practical level the results indicate that the intervention used in the present study can be delivered in a time-limited group format, and has the potential to be a practical and usable psychosocial intervention for practitioners who, in the context of diminishing mental health resources, need to provide time- and cost-efficient treatments. Further research with a larger sample size and recruitment from a clinical setting is indicated.