
Abstract
Despite the existence of effective interventions for anxiety disorders, relapse – or the return of fear – presents a significant problem for patients and clinicians in the longer term. The present paper draws on the experimental and clinical behavioural literature, reviewing the mechanisms by which the return of fear can occur. The aim of the paper was to generate a list of treatment recommendations for clinicians aimed at reducing relapse in successfully treated anxiety disorders. Clinical and experimental literature on the mechanisms of renewal, reinstatement, spontaneous recovery and reacquisition are reviewed. These are linked with the clinical and experimental literature on the return of fear in successfully treated anxiety. A list of recommendations to assist in reducing the probability of relapse in successfully treated anxiety is presented. This list includes methods for use in behavioural (exposure) treatment of anxiety disorders that aim to enhance clinical outcomes. Despite the significant problem of relapse in successfully treated anxiety, there are methods available to reduce the probability of relapse through return of fear. Clinicians engaging in treatment of anxiety disorders should be mindful of these methods to ensure optimal patient outcome.
Anxiety disorders are high-prevalence conditions, occurring in almost 10% of the Australian population in any 12 month period [1]. The disorders significantly impair an individual's functioning [2], and reduce their overall quality of life [3–5]. They have attracted growing research interest, generating a rapidly expanding literature [6, 7]. Despite the existence of several effective treatments, relapse remains a problem, with between one-third and two-thirds of anxiety disorder patients relapsing after 8 years [8, 9]. In the present review we examine the behavioural conceptualization of anxiety and fear, as well as the common observation of relapse of successfully treated anxiety responses. We conclude with an examination of the factors demonstrated to influence the return of fear responses, and present a list of preliminary suggestions for clinical practice.
Learning models of fear
Learning models of anxiety and fear have become a key component in the understanding of anxiety disorders. In these models, conditioning research has provided invaluable insights into fear learning [10]. The conditioning of emotional responses such as fear is a central component of contemporary learning models of the development of anxiety disorders such as specific phobia [11, 12] and post-traumatic stress disorder [13], among others [14].
Conditioning models typically specify that certain salient stimuli are able to elicit anxiety responses automatically. An unconditioned stimulus (US) such as pain or loud noise is capable of triggering a reflexive unconditioned response (UR) of anxiety. Furthermore, when a neutral stimulus is paired with the presentation of the US, that previously neutral stimulus becomes a conditioned stimulus (CS), itself capable of eliciting a conditioned response (CR) of anxiety. Learning models also specify that avoidant behaviours that serve to reduce fear are negatively reinforced because they lead to a reduction in anxiety. Such reinforced avoidant responses are elicited when the fear-eliciting stimulus is encountered again.
It is important to note that CRs can manifest in numerous ways, including physiological changes such as the magnitude of skin conductance responses and changes in heart rate [15], emotional changes such as increased subjective fear levels, cognitive responses such as changes in deployment of attention, and behavioural responses such as avoidance or flight, which in turn serve to maintain the acquired fear response over time [16–18]. In addition, although Pavlovian conditioning has provided valuable insights into the understanding of fear and anxiety disorders, several other pathways, such as vicarious learning and verbal transmission, have been proposed in models of fear acquisition [19–21]. In many situations, even these alternative pathways can have as their basis the learning of the association between a stimulus and an aversive event (i.e. Pavlovian conditioning) [22].
Behavioural treatment of fear
Learning-based models of fear acquisition form the basis for contemporary approaches to the treatment of fear and anxiety disorders. Numerous studies have demonstrated the effectiveness [23, 24] and cost-effectiveness of behavioural and cognitive-behavioural interventions for anxiety disorders [25]; a key component of which is exposure therapy, which exerts its clinical effect (at least in part) through extinction processes [26–28]. In extinction, the feared object (i.e. CS) that elicits fear and anxiety (i.e. the CR) is presented in the absence of other anxiety-eliciting stimuli and with repeated presentations of the object alone, the fear response (i.e. the CR) is attenuated. In cognitive behavioural interventions, exposure therapy is also typically coupled with somatic and cognitive management strategies [29].
Despite the fact that behavioural and cognitive behavioural treatments have been shown repeatedly to produce strong treatment outcomes, with success rates as high as 85% for some anxiety disorders [29], relapse or the return of fear (ROF) can affect as many as 33–50% of successfully treated individuals [30–32]. A typical example of ROF as seen in clinical practice is the successful reduction in fear through exposure-based treatment, followed by a period in which the individual does not come into contact with their previously feared object or situation. After such a hiatus, presentation of the feared stimulus will produce a fear response in subjective experience and objective measures that is higher than the level present immediately after treatment. Although ROF does not commonly lead to a fear response of the same strength as pre-treatment fear levels, it can present a significant clinical problem [33]. There also exists the possibility that small lapses may recur with increasing strength to ultimately result in a full relapse to pre-treatment levels.
The mechanisms underlying ROF after successful treatment have been the focus of considerable research attention in recent years [34, 35]. Renewal, reinstatement, spontaneous recovery, and reacquisition have been proposed as learning-based mechanisms by which fear may return. Contrary to earlier theory, recent research on these procedures has illustrated that the extinction of fear through exposure therapy does not destroy the original association between the feared object and aversive event (i.e. the CS–US association) [34, 35]. Instead, the extinction process produces new learning such that the feared object has two meanings: one that is based on the original fear association with the aversive event and one that is not (i.e. a CS–no US association). Thus, the feared object is essentially rendered ambiguous after extinction [34]. As a result, other cues, such as the context in which the object is encountered, are used to resolve the ambiguity. This may result in the retrieval of the original fear association rather than the extinction learning and, thus, the fear response may return. The mechanisms of renewal, reinstatement, spontaneous recovery, and rapid reacquisition illustrate the various ways in which this retrieval process may be activated.
Renewal
Renewal refers to the phenomenon whereby the context in which the feared object is presented, influences the extent of ROF. A clinical example of renewal is when the original acquisition of the fear response takes place in one context (e.g. acquiring a fear of honeybees following the experience of being stung in the backyard) and exposure therapy takes place in a second context (e.g. the therapist's consulting room). Once successful treatment has concluded, presentation of the feared stimulus in the original context (e.g. coming across a honeybee in the backyard again) may renew the fear response. Laboratory-based research using animal subjects has established this as a mechanism for ROF (Figure 1) [36–40]. The process outlined here is generally referred to as ABA renewal (i.e. fear learning occurs in context A, extinction in context B, and the renewal test context of A matches the original acquisition context). But renewal can also occur when the feared stimulus is presented in a third unrelated context (ABC renewal) [36, 39, 41, 42], or when the third context is different to that of acquisition and extinction (AAB renewal). ABC and AAB renewal are not generally not as strong as the ABA type [39].
Four major mechanisms of return of fear: renewal, reinstatement, reacquisition and spontaneous recovery. CS, conditioned stimulus; US, unconditioned stimulus.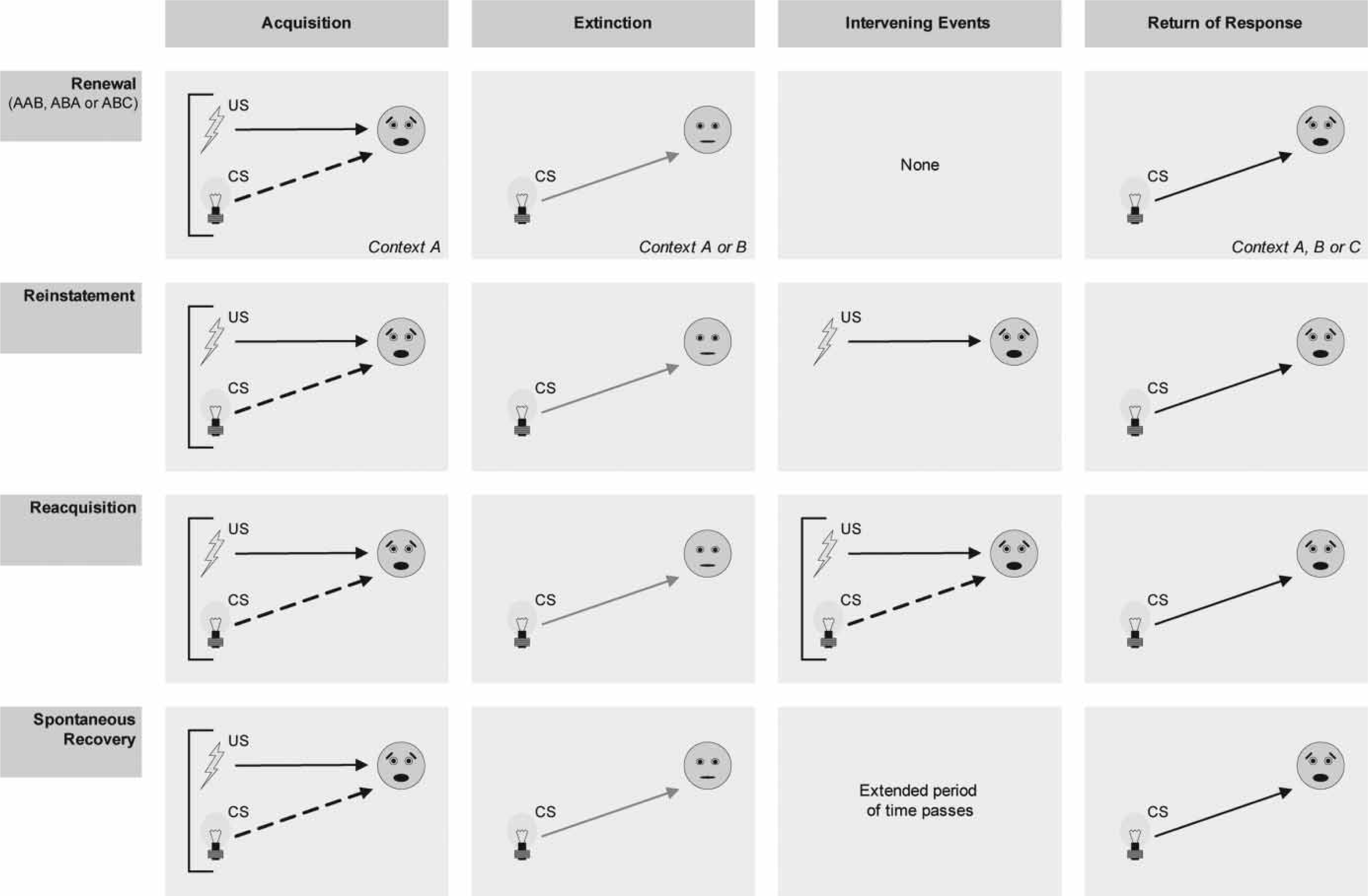
The various ways in which renewal of fear can occur has important clinical implications. It could be argued that relapse of fear via ABA renewal can be addressed by conducting exposure therapy in the original acquisition context. But this will not prevent relapse via AAB renewal when the patient encounters the feared stimulus in a novel context. Furthermore, the ABC renewal process suggests that regardless of the context in which exposure therapy takes place, there exists the possibility for ROF when the feared stimulus is encountered in a novel context. Clinically, a patient treated successfully for their fear of honeybees in both the consulting room and the backyard in which their original acquisition took place may still experience a renewal of their fear response when the honeybee is encountered in a different context.
Renewal effects are strong and robust, with the original learning shown to be resilient to extensive efforts to achieve extinction. Even large numbers of extinction trials (e.g. >160) have been demonstrated in some laboratory studies to be ineffective at preventing renewal [40, 42], although other non-human research suggests that massive extinction procedures using up to 800 trials can be effective in attenuating renewal [43]. The applicability of this research to clinical practice remains largely untested, and the ability to conduct such massive extinction in the clinical context may be difficult for practical reasons.
Renewal effects have been observed in human clinical research using spider-fearful individuals. Mineka et al. conducted a 2 h exposure/modelling session in which individuals with spider fear had their fear responses extinguished [44]. After a 1 week hiatus those individuals who were successfully treated were reassessed using a combination of a behavioural approach test, as well as self-report questionnaires assessing subjective fear. For half of these participants the follow-up assessment was conducted in the same location (i.e. context) as the extinction procedure, while for the other half the follow-up assessment was conducted in a different (novel) location. Individuals who were retested in a context different from extinction showed a moderate renewal of fear comparative to those who underwent extinction in the same context as follow-up testing. Rodriguez et al. used spider-fearful individuals in a similar study, but allowed a 2 week hiatus period between extinction and retesting [45]. In that study contextual differences included the presence/absence of a particular therapist and salient visual cues within the test rooms, as well as the location itself. Although self-reported fear did not show renewal in a different context, other measures such as heart rate and behavioural avoidance provided support for ROF through renewal.
Mystkowski et al. demonstrated that contextual differences that lead to renewal of fear may be interoceptive as well as external environmental stimuli [46]. These researchers administered caffeine or a placebo to spider-fearful individuals who were undergoing exposure treatment for their fear. To test for the interoceptive context effect, participants were retested for fear levels after a delay, by re-exposure to the spider stimuli, with half being given the same solution and half being given the alternative. For those who were subsequently retested after being given the same solution, a significant renewal of fear responses was observed. The implications of these results are relevant for therapeutic approaches that combine medications with exposure treatment. The ROF via renewal may remain as a potential danger if the individual discontinues their medications after exposure treatment has concluded. At the very least, the exposure treatment should be continued well beyond the cessation of all medications.
Recent research has also hinted at procedures by which renewal of fear may be attenuated. Again using spider-fearful participants, Vansteenwegen et al. extinguished fear responses using an exposure procedure in one building, and then followed participants up for retesting after a 3 and 12 month delay [47]. After 3 months there was no evidence of increased ROF for those participants who were retested in a different room and building. At 1 year follow-up, however, participants tested in a different location showed significantly less ROF on their self-report measure of spider anxiety. The authors suggested that this reduction in the ROF reflected that the participants were exposed in multiple contexts (i.e. the initial extinction and 3 month follow-up context) prior to the 1 year follow-up testing session. Exposure in multiple contexts may have increased the generalization of extinction learning to the follow-up testing session. Animal and human research has also supported the proposition that when extinction is conducted in multiple different contexts, renewal may be attenuated [42, 48, 49], although not all authors have found this [50, 51]. Although requiring further direct experimental and clinical support, this interpretation suggests that there are means by which ROF via a renewal effect may be attenuated.
A more direct attempt to explore factors that may attenuate the renewal of fear was reported by Mystkowski et al. [52]. Spider-fearful individuals participated in exposure treatment that was conducted in a room with distinctive environmental stimuli. When follow-up assessment was conducted (in a different room), half of the participants were asked to mentally retrieve the memories of the treatment room, while the other half were instructed to retrieve memories of events from a different, unrelated time. Significantly less renewal of fear responses were observed for those participants who mentally retrieved the extinction treatment context at follow-up. The results are encouraging in suggesting that there may be cognitive strategies that could be used by individuals after treatment in order to reduce ROF through a renewal effect.
Reinstatement
Reinstatement refers to the phenomenon whereby successfully extinguished fear responses recur after one or more exposures to the aversive stimulus (US) alone has taken place (Figure 1). Such reinstatement is often strongest when exposure to the previously feared object is conducted in the same context as that in which the aversive stimulus was presented alone [34]. A clinical example of reinstatement is when an individual develops a driving phobia following a motor vehicle accident in which they were seriously injured. After successful exposure treatment of the driving phobia, the individual is injured while working at home, which serves to reinstate the association between driving and fear.
While reinstatement has been extensively investigated in experimental studies, there is considerably less clinical research into this mechanism of ROF. This is likely due to the difficulty in testing for reinstatement effects in an ethical and experimentally controlled manner in the clinic. By definition, reinstatement occurs due to the re-experiencing of the fear response after successful exposure treatment. Such a fear response can be difficult to elicit in clinical contexts. One example of this difficulty is an investigation by Rachman and Whittal with snake- and spider-phobic individuals [53]. Phobic individuals participated in an exposure procedure in which fear responses were successfully extinguished, and then were asked to return in 2 weeks. After this 2 week hiatus the participants took part in a retest session in which half were presented with an electric shock to their forearm during their behavioural approach test, while the other half did not receive such a shock, acting as a control. Despite the reported increase in subjective anxiety and nervousness in the shock group, there was no significant difference in subjective fear or heart rate response to the feared objects between the experimental and control conditions. In that research the authors posited that the failure to observe a reinstatement effect was due to the shock stimulus being insufficiently aversive, supported by the fact that the shock alone failed to elicit an increased heart rate in the experimental group.
Despite these methodological concerns in the Rachman and Whittal study [53], results from other human laboratory investigations suggest that reinstatement in humans can also be observed [54–57]. Dirikx et al., for example, used a differential conditioning paradigm in which undergraduate students were conditioned using a shock US paired with one of six facial images [55]. After a subsequent extinction phase in which all images were presented without the shock, half of the participants underwent a reinstatement procedure in which they received a shock during playback of a series of audio stimuli. Following this reinstatement phase, participants who received these additional shocks reported significantly greater fear ratings towards the facial image than those participants who did not undergo reinstatement using a shock US. These experimental findings require replication and extension to clinical contexts.
Spontaneous recovery
Spontaneous recovery is the most well-known process to occur after extinction, with observations of this behavioural phenomena dating back to the seminal work of Pavlov in laboratory experiments with dogs [58]. In spontaneous recovery, a successfully extinguished fear response can be elicited by the feared object following a period of time in which the feared object (CS) or aversive event (US) are not experienced. Such a CR can recover to the extent that it is as strong after the hiatus period as before the extinction procedure (Figure 1) [59]. A clinical example of spontaneous recovery is when an individual successfully treated for agoraphobic fear and avoidance of shopping centres, does not go to shopping centres for a period of several weeks. Following this hiatus, the individual experiences a recovery of the successful treated fear response when return to a shopping centre.
Numerous explanations exist for the spontaneous recovery phenomenon [60, 61]. One explanation proposed by Bouton suggests that the passage of time represents a gradually changing context [34, 35]. In that model, extinction may be specific to the environmental context in which it occurs, as well as the temporal context. Such an explanation likens spontaneous recovery to the renewal effect, with the changed context being a different time rather than different environment. One similarity that supports this suggestion is that when a retrieval cue is presented that reminds the individual of the extinction process, the return of the conditioned behaviour is attenuated [62]. These results suggest that spontaneous recovery and renewal both represent problems with retrieval of extinction information in contexts (whether physical or temporal) that are outside the original extinction context [34].
ROF can occur in successfully treated individuals, despite no clear evidence that they have been re-exposed to pairings of the feared stimulus and an aversive event. When such relapse occurs it may be explained by the process of spontaneous recovery. An early description of spontaneous recovery of fear was reported by Rachman in a seminal paper in 1979 [63]. Numerous clinical and laboratory studies have since reported on similar observations. Such spontaneous recovery of fear responses has been documented to occur after both short-term and long-term time delays. Moreover, spontaneous recovery occurs in a sizable proportion of successfully treated individuals. For example, Philips completed successful treatment with a small group of emetophobic patients, finding that just under half of patients showed significant spontaneous recovery of their anxiety responses [64]. Broadly comparable findings have been reported in claustrophobia [65], spider phobia [66], and snake phobia [32].
Reacquisition
Reacquisition refers to one or more additional pairings of the feared object (CS) and aversive event (US) after successful extinction, leading to a reacquired ability of the CS to elicit the CR (Figure 1). For example, a patient successfully treated for learned agoraphobic avoidance of shopping centres, rapidly reacquires a fear response following an unexpected panic attack at their local shopping complex. Reacquisition can occur at different rates, with some studies requiring numerous re-pairings of the CS and US [67–69], and others demonstrating rapid reacquisition as though extinction had never occurred [70]. Variations in the speed of reacquisition have been theorized to relate to whether the context under which reacquisition is tested leads to retrieval of the conditioning or extinction associations [34]. In this model, when the context leads to retrieval of the original conditioned association, reacquisition is rapid, while when the extinction associations are retrieved the process is significantly slower. Thus, contextual cues are important in determining the rate and strength of reacquired CRs. Clinical research into reacquisition has, unfortunately, been limited due to several difficulties, including ethical issues with re-exposure to an aversive stimulus, and difficulty in identifying the original CS–US pairing [19].
Factors influencing return of fear
Previous authors have divided the factors that influence the ROF into (i) training factors and variables during the exposure process; (ii) post-training factors that occur after the successful extinguishing of the fear response; and (iii) state-related factors of the individual. Training factors such as the level of difficulty of the exposure task (‘demand’ [71]), number of exposure trials [30], utilization of distraction techniques [32], and speed of fear reduction [53, 72] have all been evaluated to assess their relationship to ROF. Results of this research, however, are often inconsistent across studies. Post-training factors hypothesized to influence ROF include reinstatement and related phenomena mentioned here. As noted earlier, research into reinstatement of fear in humans has been scarce. Finally, several state-related factors have been investigated in studies of the ROF phenomenon. Several of these factors have been demonstrated to influence ROF, although it could be said that the single most consistent finding is the lack of consistency across different studies. Variables including initial fear levels, cognitive content and process, and mood state during exposure have all being examined.
One example of the inconsistent findings regarding state-related factors in predicting ROF is that of the original intensity of fear when an individual is exposed to their feared stimulus. Some studies using clinical populations have demonstrated that ROF is positively correlated with initial fear levels for individuals with panic disorder [73], and social/performance anxiety [30]. Conversely, in a sample of patients with claustrophobia, subjective fear ratings did not predict ROF, while heart rate during initial exposure did [65]. A similar negative finding was reported by Rose and McGlynn, who found that initial fear level did not predict ROF in a sample of snake-phobic individuals [32]. These differences may relate to methodological differences or differences across different anxiety disorders.
One finding that has emerged with some consistency is the ability of cognitive variables to predict ROF. A small collection of studies now support the idea that both cognitive content and cognitive processes can be associated with ROF. Craske and Rachman reported that anxiety-related cognitions were associated with ROF in anxious music performers [30]. Cognitive biases such as covariation biases (the tendency to associate aversive outcomes with phobic stimuli) were also associated with eventual ROF in spider-phobic individuals [66]. Individuals who experience a sudden and subjectively important reduction in fear responses during treatment have also demonstrated reduced incidence of ROF [72].
The mood state of individuals during exposure tasks may also have an impact on the likelihood of ROF. At least three studies have demonstrated that there is a higher probability of ROF in patients who undergo exposure treatment while in a dysphoric mood state, than for those patients in a positive mood state. This increased ROF has been observed when participants are tested 30 min [74], 1 week [64], or 1 month [75] after exposure. Such a difference is still observed even when all participants are retested when in a neutral mood state at follow up [74]. It has been suggested that this effect may result from both a more elaborate encoding of negative material and a less elaborate encoding of positive material during exposure conducted in a dysphoric mood state.
Clinical practice research
An important application of the understanding of the ROF phenomenon is attempts to reduce the likelihood of relapse in patients successfully treated for an anxiety disorder. The aim of research was to elucidate the treatment approaches that may assist in reducing the possibility of relapse from ROF. Psychologists and psychiatrists conducting behavioural or cognitive behavioural interventions for the anxiety disorders can draw on this literature when planning their treatment, and educate their patients of this relapse risk. Treatment variables demonstrated to reduce the probability of ROF after successful treatment include extended duration exposure sessions, increased numbers of exposure sessions, increased hiatus between exposure sessions, reducing or eliminating the use of distraction during exposure, the use of multiple assorted exposure stimuli, use of diverse contexts, and rehearsal out of session.
In typical clinical practice, exposure sessions are conducted for as long as is required for a patient to demonstrate habituation to the feared stimulus. In this scenario, habituation is deemed to have occurred when the patient shows little or no anxiety response despite continued exposure to the phobic stimulus. At least one previous study has suggested that ROF may be attenuated through extending individual exposure sessions beyond the point of habituation. According to unpublished data, Craske, Lopatka and Rachman (as cited in [33]) conducted exposure procedures in which the participant's individual exposure sessions were extended for a further 10 min after habituation had occurred. Rachman [33] reported that this extended exposure procedure resulted in some suppression of ROF in their participants.
Some authors have suggested that increasing the overall total number of exposure sessions may reduce the probability of ROF. In an early investigation, Agras reported that repeated exposure reduced spontaneous recovery of fear in a group of six individuals with a specific phobia [76]. A similar small cohort of patients with emetophobia was treated by Philips, who used an extended number of sessions to treat participants who showed significant between-session ROF [64]. In that report a larger number of exposure sessions (13 compared to eight) resulted in the elimination of spontaneous recovery of fear in the short term, and at 6 month follow up. Although human clinical studies are few in number, there is also evidence from animal fear studies that repeated massive extinction procedures can reduce the renewal of extinguished fear responses that are otherwise difficult to reduce by standard extended extinction treatments [77]. It is also important to note that clinical research using this method has been restricted to attenuating spontaneous recovery, and is yet to be investigated as a method of reducing other mechanisms of ROF such as renewal and reinstatement.
Clinical studies using exposure therapy have also varied the hiatus period between each exposure session. Although there is some indication that massed or even single-session exposure can be effective [78], there is also evidence that increasing durations between successful exposure may help reduce the probability of ROF occurring. To assess this possibility, Rowe and Craske compared the use of massed exposure procedures versus an exposure schedule with increasing durations between exposure sessions using a sample of spider-phobic individuals [79]. In that study, individuals who received massed exposure sessions showed more complete habituation during treatment than the expanding-spaced exposure groups. Despite this, however, those participants on the expanding-spaced exposure schedule showed significantly less spontaneous recovery of fear. This was true when they were presented with either the same spider used for exposure treatment, or a different, novel spider. Problematically, these results were not replicated when Lang and Craske used expanding-spaced exposure sessions in treatment of height phobia, finding no significant differences in ROF [80]. The authors did, however, question whether their 1 month follow-up period was a sufficiently long enough time for differences in ROF to be observed.
Early behavioural theory in which some explanations of exposure therapy are grounded suggests that the use by patients of distraction techniques during exposure may serve to prevent full engagement and habituation to the feared stimuli. Surprisingly, few studies have examined the impact of distraction during exposure on spontaneous recovery of fear responses. Rose and McGlynn reported on an experimental study in which snake-fearful participants were asked to either focus on the snake stimuli, or monitor an irrelevant audiotape for certain key phrases [32]. Both experiments in that paper showed that ROF was more frequent in the group who utilized distraction, but those results did not reach statistical significance. Although the authors interpreted their findings as being suggestive that distraction may increase the likelihood of ROF being observed, replication with a larger sample would be required to more comprehensively answer questions around the role of distraction in ROF.
The renewal effects discussed here may be reduced by conducting exposure therapy with multiple different stimuli, as well as in multiple different contexts. Two published studies examining the use of varied stimuli, however, have returned inconsistent findings. Using a group of 28 spider-phobic students Rowe and Craske assessed the impact of using a variety of stimuli on eventual ROF [81]. Half of the students were exposed to a single tarantula over four exposure trials, while the other half was exposed to a different tarantula in each of the four exposure trials. When the participant groups were reassessed after a 3 week hiatus, the group that had seen only the single spider showed greater ROF than those who had undergone exposure to a series of different spiders. Lang and Craske attempted to replicate the earlier work of Rowe and Craske using participants who had a specific phobia of heights [80, 81]. Using a similar design, half of their participants were exposed to the same situation across exposure trials, while the other half was exposed to a series of different situations. Unlike Rowe and Craske [79], however, there was no significant difference in ROF between the two groups as seen on subjective, behavioural, or physiological measures. The authors cited reasons such as differences in exposure duration, and insufficient variability in the stimulus materials as potential reasons for the difference between their findings and those of Rowe and Craske. The effect of varied exposure stimuli on eventual ROF remains unclear, and further work using longer-term follow up is also needed.
Early findings that ROF is more frequently observed when exposure tasks are more demanding suggests another avenue by which clinicians may reduce the likelihood of ROF. Exposure therapy sessions that result in dramatic increases in subjective anxiety have been associated with increased likelihood of ROF [71]. This suggests that the level of difficulty for exposure treatment sessions needs to be carefully planned, with collaboration between patient and clinician. A balance needs to be struck between exposure to significant stimuli to allow meaningful extinguishing of fear responses, and the not placing of unnecessarily high demand on the individual and thereby increasing the probability of ROF occurring.
Individuals who engage in behavioural or cognitive behavioural treatment for anxiety disorders are usually assigned homework tasks to consolidate the gains made in therapy. There is preliminary evidence that one such task, imaginal exposure, may assist in reducing ROF. Sartory et al. assessed the impact of a 30 min imaginal exposure session immediately following a successful in vivo exposure session in a group of 28 animal-phobic individuals [82]. Half of the participants spent 30 min after exposure conducting imaginal exposure, while the other half were asked to distract themselves with unrelated magazine articles. When participants were reassessed 1 week later the group who used distraction immediately following exposure showed increased ROF as measured on subjective fear ratings. Although it could be argued that the imaginal exposure group received an increased number of exposure trials, these findings give tentative support to the importance of rehearsal and imaginal exposure after successful treatment to reduce ROF.
Recent research has investigated the ability of the N-methyl-D-aspartate (NMDA) agonist, d-cycloserine (DCS) as an adjunct to the treatment of phobic anxiety. While DCS has been demonstrated to be effective in enhancing exposure therapy in a virtual reality environment and social anxiety [83, 84], there is less evidence of its ability to prevent ROF. In a large group of undergraduates, DCS treatment did not lead to differences in ROF [85]. Because the authors did not administer DCS throughout the experiment up to the assessment of ROF, it could be argued that presence/absence of the drug may have acted as a context based on interoceptive cues, thus leading to renewal of the fear response. DCS, however, has little or no subjective effect when administered, making such a possibility less likely. The role of DCS in exposure and ROF attenuation remains unclear, and requires further research to replicate the recent findings of Guastella et al. using clinical participants [85].
Cognitive factors in the return of fear
While a detailed examination of the cognitive factors involved in anxiety disorder relapse is beyond the scope of the current review, it is important to consider the role of these factors in the narrower phenomenon of ROF. ROF has been conceptualized as a primarily behavioural process, with little experimental or clinical research into cognitive processes that may exacerbate or attenuate the effect. This is particularly surprising when considered in light of the trend towards combined cognitive and behavioural interventions in clinical practice. Although there remains considerable room for research into the use of cognitive techniques in reducing ROF, a small number of articles provide hints as to how clinicians mat attempt to attenuate ROF using cognitive techniques.
Using a sample of spider phobics, Mystkowski et al. attempted to reduce renewal of fear response by having patients mentally reinstate the conditions under which treatment occurred [52]. Instructions were given to half of the successfully treated participants to recall details of the treatment context before being re-exposed to the feared spider stimulus. The other participants were asked to remember an irrelevant task (getting ready for work or school in the morning). ROF, as measured by subjective discomfort, was reduced for those participants who attempted mental reinstatement of the treatment context. The authors suggested that mental reinstatement may be incorporated into exposure treatment protocols to assist in reducing ROF, and to assist in generalizing treatment effects from the treatment setting into other contexts.
Another investigation into the cognitive influences on ROF provides a tentative suggestion that ROF may be reduced through cognitive restructuring of covariation bias. As stated previously, individuals who associate phobic stimuli with aversive outcomes are more vulnerable to relapse after treatment than those with weaker associations [66]. Cognitive restructuring aimed at assisting patients to evaluate, reconsider, and restructure these associations may assist in the reduction of risk of ROF. Such a suggestion, however, is very tentative and requires further experimental and clinical validation.
Conclusions and recommendations for clinical practice
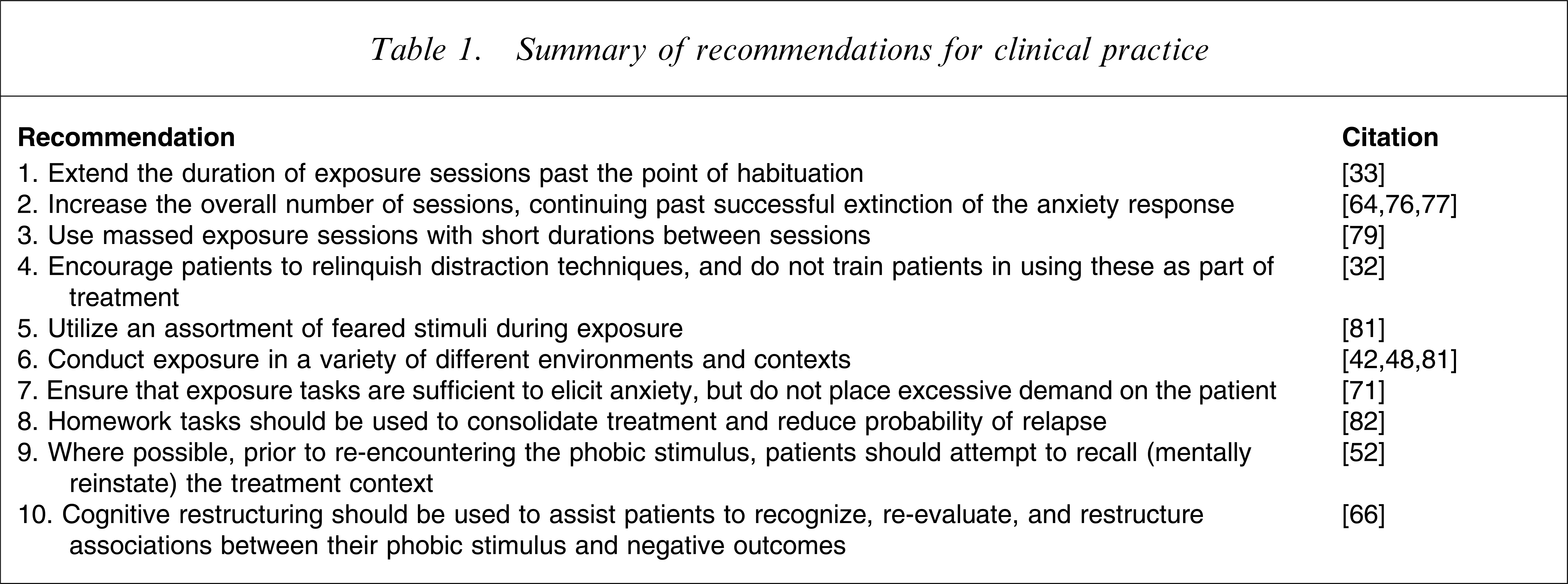
We offer 10 recommendations for clinical practice in anxiety disorders that may serve to reduce the probability of relapse following exposure-based treatments. Many of these recommendations, however, are tentative, based on studies requiring replication, including in clinical contexts. A summary of the recommendations is provided in Table 1. First, therapists should extend the duration of individual exposure sessions beyond the point of within-session habituation by at least 10 min. Second, therapists should increase the overall number of exposure sessions, past the successful extinction of the anxiety response. Third, therapists should consider using massed exposure sessions, with little time between each session. Fourth, we suggest that exposure therapists encourage patients to relinquish the use of distraction techniques, preferably not using these at all during treatment. Fifth, we suggest that therapists use a variety of different feared stimuli during the exposure treatment to ensure that fear reduction is not specific to a given stimulus. Sixth, exposure should be conducted in a number of treatment contexts, including outside the consulting room and in situations that the patient is likely to frequent or in which they are likely to encounter the feared stimulus. Seventh, exposure tasks should be carefully planned so that although they are sufficient to elicit an anxiety response, they are not so fearful as to place excessive demands on the patient that may increase the likelihood of ROF. Eighth, therapists should collaborate with patients in setting homework tasks, including imaginal exposure of the feared stimulus or cues of the exposure treatment process, to consolidate the effect of treatment. Ninth, mental reinstatement of the treatment environment may be used by patients if they expect an encounter with their phobic stimulus. Tenth, patients should be assisted to restructure cognitions that inflate the association between their phobic stimulus and aversive outcomes.
of recommendations for clinical practice
Relapse remains a serious obstacle to effective, long-lasting treatment of anxiety and anxiety disorders. Behavioural research provides insights into several mechanisms by which ROF, and anxiety disorder relapse, may occur. There is an emerging body of research that also suggests clinical techniques by which the probability of relapse can be reduced. Although this evidence is in its infancy, several considerations such as the duration, frequency and number of exposure sessions, as well as careful choice of the exposure stimuli may assist the clinician and patient in reducing the chance of eventual return of successfully treated anxiety. Future research will provide additional data on which to base evidenced-based clinical practice.