
Abstract
Despite the immense personal and social impact of schizophrenia and the emerging expectation that studies need to consider recovery beyond symptom remission [1], there has been limited research characterizing its outcome from a longitudinal and multidimensional perspective. The National Institutes of Mental Health taskforce report on services research for persons with severe mental illness defined a number of critical elements required in ongoing research into clinical outcomes in schizophrenia [2]. The first of these principles was the requirement for the assessment of multiple dimensions of outcome.
Although this principle has been generally reflected in the literature [3] with an increase in the study of quality of life and alternative symptom measures, such as cognition, there have been few attempts to study the outcome of schizophrenia across all or most of the dimensions outlined in the taskforce report. These dimensions were described as (i) the clinical domain: categorical and dimensional aspects of the clinical presentations of schizophrenia as well as general health status; (ii) rehabilitation: the functional capacity of the individual and his/her adaptation to his/her environment, encompassing aspects of social and instrumental functioning, the later of which refers to a patient's capacity to problem-solve, learn, work or engage in other productive activities; (iii) the humanitarian domain: elements of personal (subjective) well-being, quality of life and satisfaction; and (iv) public safety: reflective of a need to balance the promotion of individual liberty while maximizing individual and societal safety [2].
Importantly, in addition to the principle of multidimensionality of outcome assessment, the report also argued that evaluations should be longitudinal and include detail regarding the costs of care for patients with schizophrenia. However, the assessment of treatment costs should be conducted only in combination with the study of clinical outcomes lest the results be subject to spurious interpretation [2].
Research of this kind is required to progress the development of treatment and service planning in addition to providing a richer picture of the outcomes of this critical disorder. The Schizophrenia Care and Assessment Programme (SCAP) study was developed and implemented to try and address such questions [4]. It involved the assessment of a broad range of outcomes in a large sample of schizophrenia patients treated in three countries in usual clinical care. In this paper we will present data from the Australian arm of the SCAP study describing these outcomes. A paper by Fitzgerald et al. provides further details of the economic consequences of schizophrenia [5].
Methods
Design
The SCAP study was developed by Lehman et al. as an international, multidimensional study to provide comprehensive data on the outcomes of for people with schizophrenia [4]. The Australian site for the SCAP study was based at the Dandenong Psychiatry Research Centre (DPRC) in Melbourne. Parallel studies were undertaken in the USA with 2400 patients from six sites [6], and the UK, with 600 patients from six sites [7]. Face-to-face assessments were conducted at baseline, and then every 6 months over a 3 year period. There was a 4 week window on either side of the interview date. Assessments took place in a mixture of clinical settings and at the patients’ residence. The 6 monthly assessment data were complemented by continuous health-care resource use data collection from existing electronic service use data capture systems.
Participants
The Australian SCAP cohort consisted of 347 people with a diagnosis of schizophrenia or schizoaffective disorder, confirmed against the case notes based on DSM-IV criteria, who were each followed up for 3 years. Participants were older than 18 years, and had sufficient capacity to communicate with the investigators in spoken and written English, and had not participated in a clinical drug trial in the preceding 30 days. Participants were recruited from four primary sources in order to represent the different locations of care, as well as the different types of people with a diagnosis of schizophrenia within the catchment area of the Dandenong Area Mental Health Service (DAMHS). The four sources were as follows.
Psychiatric Record Information System Manager: this is a computerized clinical record system designed to record information about patients treated in the public sector psychiatric services in Victoria. Researchers extracted names and contact details from Psychiatric Record Information System Manager (PRISM; now called RAPID) for all participants with a relevant diagnostic code. Participants who were eligible were then contacted and invited to participate in the study. Acute inpatient wards of the DAMHS: clients admitted to the service with a relevant diagnosis were approached and invited to participate. Acute and long-term follow-up community-based teams of the DAMHS: clients with a relevant diagnosis were referred to the research team by staff on these teams. Local community psychiatric services: information sheets and brochures were left in local community clinics to attract clients with schizophrenia to contact the research centre to participate.
Enrolment of participants commenced in December 1997 and was completed in June 2000. The final participant's last visit was completed in May 2003. The majority (67.7%) of participants enrolled in the study were recruited from the community psychiatric services in the area or from the community-based teams of the DAMHS. The remaining 32.3% were recruited from the inpatient wards of the DAMHS. During the course of the study a small number of participants dropped out of the study, that is, they requested to be withdrawn from the study and took no further part in it. A larger number of participants skipped one or more visits but remained in the study, allowing collection of certain types of data (e.g. resource utilization data from central databases) but not others (e.g. face-to-face interview-based data). As such, complete clinical outcomes data for a total of 198 participants (57%) and medical and economic data for a total of 267 participants (77%) were available for analysis for the full 3 years of the study.
SCAP data collection instruments
Data were collected using the following study-specific instruments.
Baseline Data Collection Form
The Baseline Data Collection Form (BDCF) collected demographic and clinical characteristics of the participants and was completed at baseline only.
Schizophrenia Care and Assessment Programme–Health Questionnaire
The Schizophrenia Care and Assessment Programme–Health Questionnaire (SCAP-HQ) [4] was completed via a face-to-face interview at baseline and every 6 months during the study, and consisted of 103 items on a broad range of domains including disease-specific outcomes, quality of life, and service use. Specifically, it covered areas such as housing, usual activities, recent symptoms, violence and suicide, alcohol and drugs, health in general, medications, service use and legal problems.
Medical Record Abstraction Form
The Medical Record Abstraction Form (MRAF) was designed to record information extracted from participants’ hospital medical records. It was completed at baseline and at each 6 month visit and pertained to the period since the previous study visit. It captured information including hospitalizations, contacts with the hospital's community services, and psychotropic medications taken during hospital stays.
Clinical outcome measures
The following clinical assessment instruments used in SCAP were administered four times: at baseline and at each 12 month visit:
Positive and Negative Syndrome Scale
The Positive and Negative Syndrome Scale (PANSS) [8] was derived from a structured clinical interview consisting of 30 items, each scored from 1 (absent) to 7 (extreme). It contains three subscales: a Positive Syndrome Scale (7 items), a Negative Syndrome Scale (7 items), and a General Syndrome Scale (14 items).
Montgomery–Asberg Depression Rating Scale
The Montgomery–Asberg Depression Rating Scale (MADRS) consists of 10 items each scored on a 7-point scale, from normality (0) to severe symptoms of depression (6) [9].
Global Assessment of Functioning
The Global Assessment of Functioning (GAF) is a single measure of the participant's psychological, social and occupational functioning on a hypothetical continuum from 1 to 100, with higher scores representing better functioning and less severe symptoms [10].
Abnormal Involuntary Movement Scale
This scale examines participants for the presence and severity of involuntary movements consistent with tardive dyskinesia [11]. The total Abnormal Involuntary Movement Scale (AIMS) score ranges from 0 to 28, with a higher score corresponding to more severe involuntary movements.
Simpson–Angus Scale
The Simpson–Angus Scale (SA) is a nine-item clinical assessment instrument used to monitor treatment-related extrapyramidal side-effects [12]. Each item was scored on a scale from 0 (absence of condition) to 4 (extreme presence of condition).
Quality of Life Scale
This scale consists of 21 items designed to evaluate current function, from 0 (most severe impairment) to 6 (normal function) [13]. Scores are generated on four domains: (i) Interpersonal Relations; (ii) Instrumental Role Functioning; (iii) Intrapsychic Foundations; and (iv) Common Objects and Activities. Due to the nature of the instrument the Quality of Life Scale (QLS) was not completed for participants if they were inpatients at the time of their visit or during the previous 4 weeks.
Assessment of Quality of Life
The Assessment of Quality of Life (AQoL) is a 15-item health-related quality of life measurement instrument that enables computation of utility values for use in economic evaluations [14]. Each item was scored on a scale from 0 (quality of life unaffected) to 4 (quality of life extremely affected).
Clinical ratings were made by three trained research assistants. Interrater reliability was established prior to the conduct of the study and was reviewed on a 6 monthly basis for the PANSS, MADRS and GAF (ratings with a coefficient of variance of >0.9).
Medication utilization
Data from internal and external electronic data collection systems were used in conjunction with the participant's medical records, and self-report data to evaluate medication utilization for each participant.
Dandenong Hospital Computerized Dispensary Records System
This provided details of medications dispensed by the DAMHS for participants who were outpatients.
Pharmaceutical Benefits Scheme
Details of medications dispensed by community pharmacies throughout Australia under the Pharmaceutical Benefits Scheme (PBS) were extracted from the electronic database of the Health Insurance Commission (HIC). Because the majority of participants (>90%) held some form of health-care concession card, most were eligible to access the highest level of subsidized service without having to reach a predetermined safety-net threshold. Thus, data extraction from these electronic registries was very complete
Statistical analysis
Clinical outcomes analysis
Repeated measures analysis of variance models were used to analyse changes in psychopathology and other dependent variables over time, and the Bonferroni correction was used to control for multiple comparisons. Pearson's correlation coefficients were calculated to study the relationship between change in baseline variables to end-study change scores (significance set at p < 0.01). Next, participants were divided into two groups, defined by improvement of >20% (group 1) or <20% (group 2) on both the PANSS and GAF scores across the study. t-tests and χ2 tests were used to study differences between them. All procedures were two-tailed and all statistical analysis was conducted with SPSS 11.5 (SPSS, Chicago, IL, USA).
Medication usage analysis
Medication usage was of considerable interest but the definition of treatment groups proved to be complex. To resolve the problem, participants were classified as being on typical, atypical or both typical and atypical antipsychotic medications during each of the study phases by looking at the number of defined daily doses (DDDs) [15] of each medication taken. The DDDs were used to calculate the approximate number of days that the patient was on a particular class of medication. Participants were categorized as taking only atypical medications if they had taken the equivalent in mg of at least 45 DDDs of any atypical antipsychotic and <45 DDDs of any typical antipsychotic during each study period of 180 days. Similarly, participants were categorized as taking only typical medications if they had taken at least 45 DDDs of any typical antipsychotic and <45 DDDs of any atypical antipsychotic during that period. Those who had taken at least 45 DDDs of any atypical antipsychotic and at least 45 DDDs of any typical antipsychotic in the same study period were categorized as taking both atypical and typical medications. The cut-off point of 45 DDDs per 180 day period was used as a proxy for the minimum therapeutic course of treatment because this is equivalent to the participant receiving one-quarter of the DDD of the medication over that period, for example, 1.25 mg risperidone, 2.5 mg olanzapine or 2 mg haloperidol.
The total amount taken (in mg) of each class of medication was calculated for each patient by study period, independently of the source of medication. PBS and hospital pharmacy medications were attributed to the period in which the medication was dispensed. The analyses were based on the assumption that all dispensed medications were taken by the patients. For consistency, in-hospital medications were attributed to the period in which the medication was started.
Results
Participants
A total of 347 people participated in the study (215 male, 132 female). Their mean age at study enrolment was 33.8±11.0 years. The majority of the population was white/Caucasian (81.3%); 0.9% were Aboriginal or Torres Strait Islander and 4.0% were Asian (13.2% other). At the time of enrolment 65.2% had never been married, 14.1% were currently married and living with their spouse and the remaining 20.7% were separated, divorced or widowed. The highest level of education achieved by the majority (60.9%) was some secondary or high school education. Ten per cent had completed a vocational course and 3.2% a university degree. The mean self-reported age of onset of mental and/or emotional problems was 24.0±7.9 years. A total of 88.8% of participants had a diagnosis of schizophrenia and 11.2% had a diagnosis of schizoaffective disorder.
A total of 267 patients (77%) completed 3 years of the study. The most common reason for dropping out was loss of contact. Health outcomes for discontinued patients remained available; these were compared to those patients who completed SCAP. No statistically significant difference was found at any of the study phases and for any of the outcome measurements, except 12 months. Participants who had discontinued at this time had significantly worse positive, general and total PANSS scores compared to the rest of the group.
Clinical outcomes
Table 1 presents the PANSS, MADRS, GAF, side-effect and Quality of Life (QOL) assessment scores for the various study phases. Most of the improvement in clinical states occurred in the early phases of the study, with the most significant gains seen in the reduction of general and positive symptoms of the PANSS and in SA scores in the first year. There was a significant reduction in PANSS positive, negative and general symptoms (all p < 0.001) as well as depression (MADRS score, p < 0.001) over the course of the study. Changes in total PANSS scores were calculated from baseline to study end. A total of 79.1% of patients experienced a decrease in total PANSS scores (and thus improved functioning) and 20.9% an increase (indicating a worsening of symptoms). However, only 4.1% achieved a >50% improvement across the course of the study.
Baseline and yearly study assessments
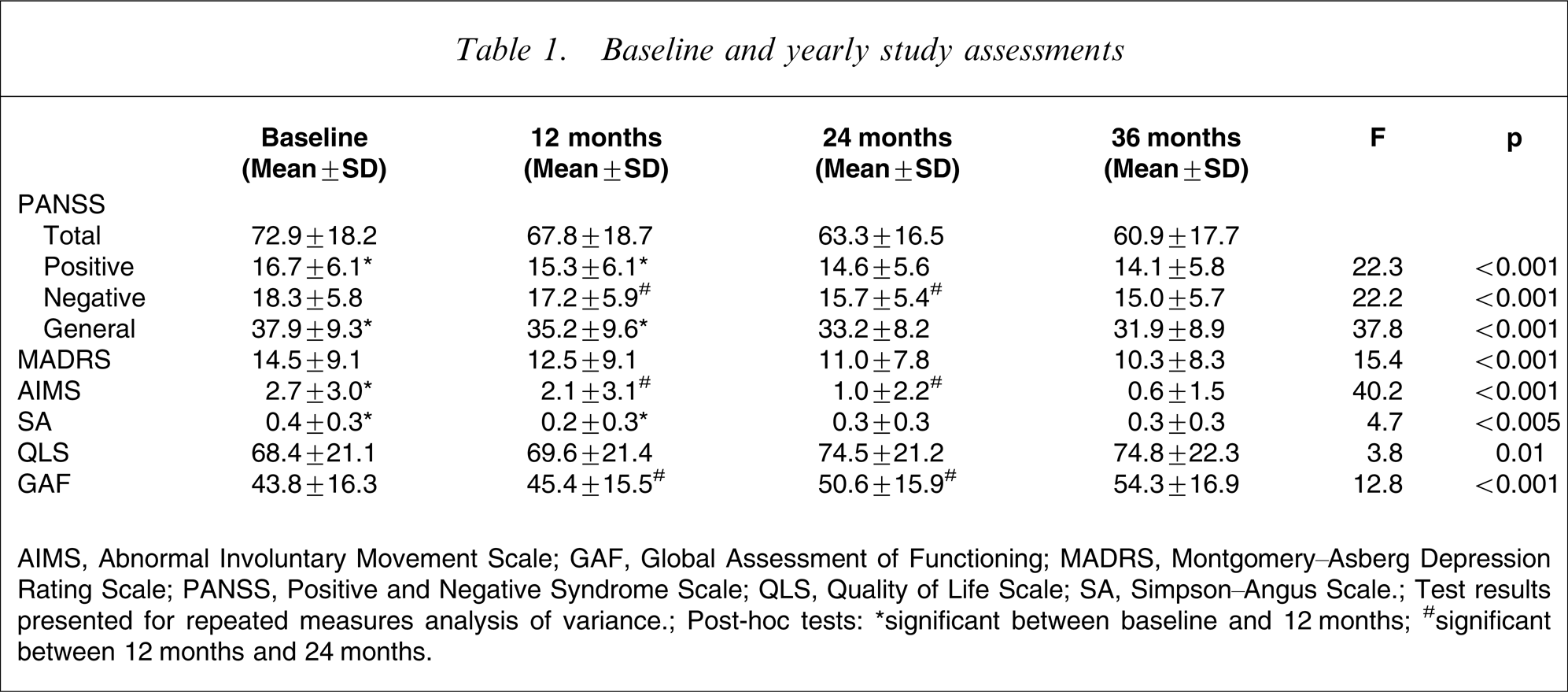
AIMS, Abnormal Involuntary Movement Scale; GAF, Global Assessment of Functioning; MADRS, Montgomery–Asberg Depression Rating Scale; PANSS, Positive and Negative Syndrome Scale; QLS, Quality of Life Scale; SA, Simpson–Angus Scale; Test results presented for repeated measures analysis of variance; Post-hoc tests: ∗significant between baseline and 12 months; #significant between 12 months and 24 months.
There was also a significant overall increase in GAF scores (p < 0.001) indicating better functioning with lower symptomatology. The greatest mental health improvements as measured by reduced negative symptoms and increased GAF scores occurred in the second year of the study. A total of 68.8% of patients reported an improvement in GAF scores from baseline to study end, with 38.7% experiencing a >50% increase in GAF scores; 21.2% experienced a reduction in GAF scores indicating a worsening of global functioning. With regards to medication-related motor side-effects, there were reductions in the AIMS (p < 0.005) and SA scores (p < 0.01), denoting less symptoms.
Clinical data from the SCAP-HQ instrument are presented in Table 2, and show a significant decrease in psychopathology (p < 0.001) across the time of the study. There was also a decrease in suicidality (p < 0.001), although this difference was small in magnitude and of questionable clinical significance. There was no change in self-reported problematic drug and alcohol use (p > 0.05). There was a significant reduction in subjective medication-related side-effects (p < 0.001).
SCAP-HQ results
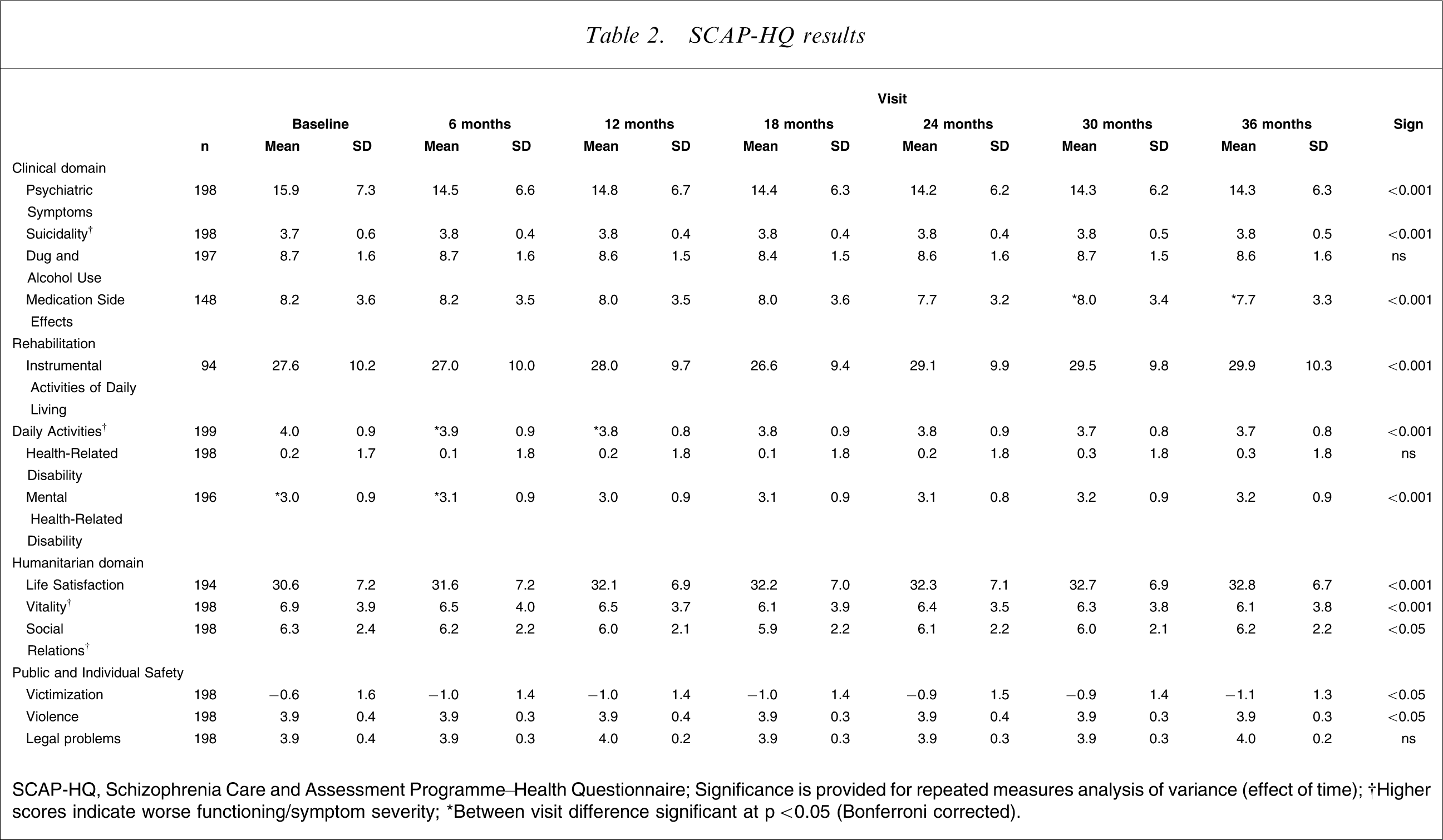
SCAP-HQ, Schizophrenia Care and Assessment Programme–Health Questionnaire; Significance is provided for repeated measures analysis of variance (effect of time); †Higher scores indicate worse functioning/symptom severity; ∗Between visit difference significant at p < 0.05 (Bonferroni corrected).
Antipsychotic medication use
The use of medications during the study is presented in Figure 1 and Table 3. There was a significant change in the percentage of patients taking only atypical antipsychotics (35.9–59.9%) over the course of the study. There was a concurrent fall in the use of only typical and combination of typical and atypical antipsychotics. There was also a significant decline in the proportion of patients receiving very low doses of antipsychotics (defined as <25% DDD [15, 16]) over the course of the study. Because medication use was measured by the number of prescriptions filled, this was used as a proxy measure for poor medication adherence.
Use by class and study phase for Schizophrenia Care and Assessment Programme participants.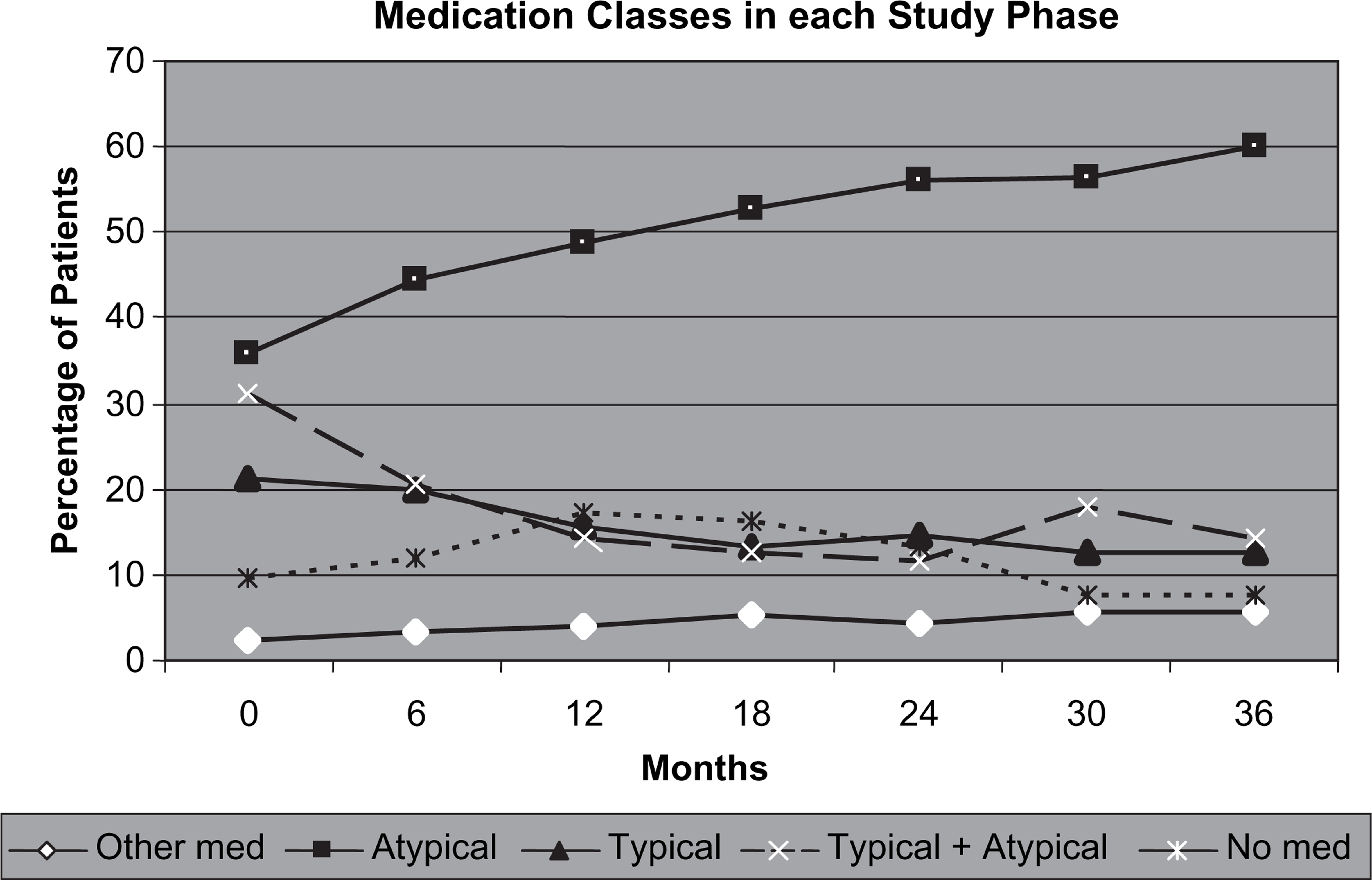
Medication use per study phase
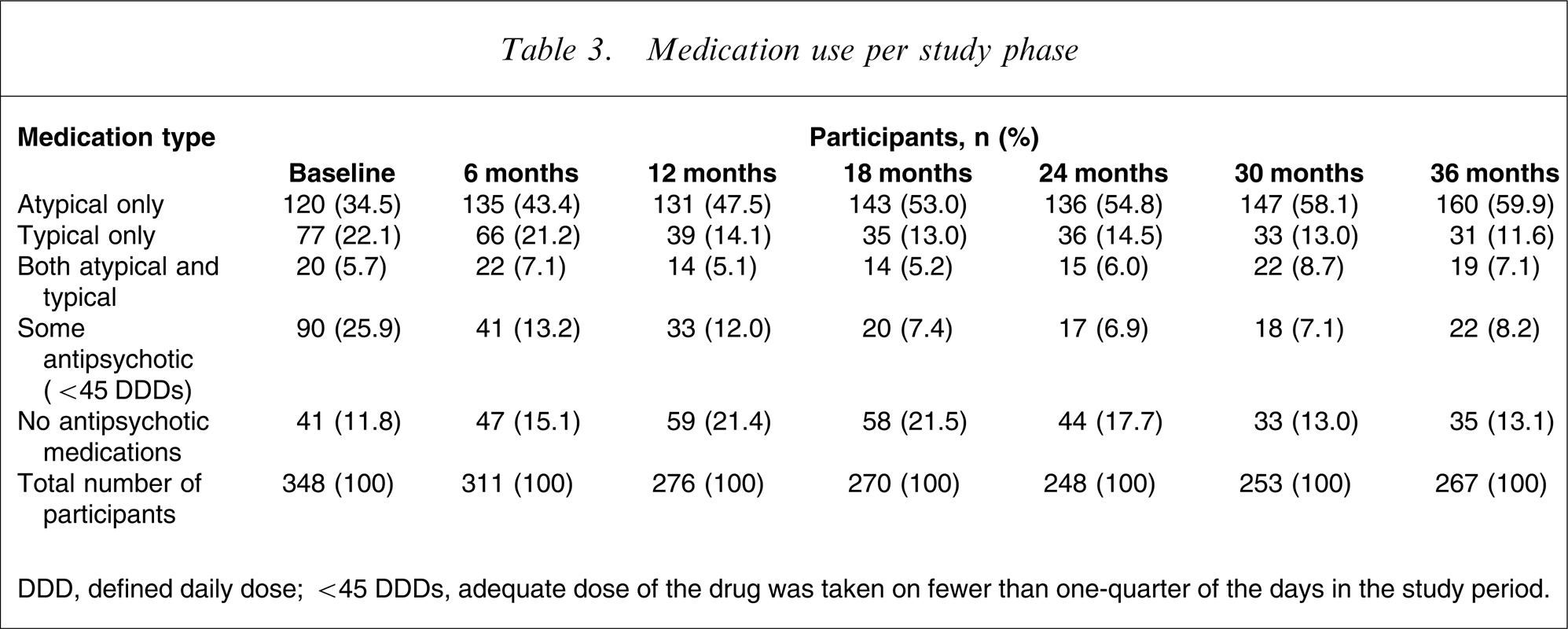
DDD, defined daily dose; <45 DDDs, adequate dose of the drug was taken on fewer than one-quarter of the days in the study period.
Rehabilitation and functioning
There was a significant improvement in reported instrumental activities of daily living (p < 0.001) as well as daily activities (p < 0.001; Table 2). There was no significant change in health-related disability but a slight increase in mental health-related disability (p < 0.001).
With regard to observer-rated quality of life, there was a significant improvement in QLS scores (p = 0.01). There was a significant improvement on the intrapsychic foundations (p < 0.001), instrumental role functioning (p = 0.05) and common objects and activities (p < 0.005) subscales but no change for interpersonal relations (p > 0.05).
When considering employment, we found that a minority of patients held paid employment in the 4 weeks prior to each study visit (11% at baseline–16% at 36 months). The average number of days worked over the 4 week period ranged from 13.4±7.9 (18 months) to 11.7±8.1 (24 months). There was no clear pattern of increased or decreased employment over the course of the study. Use of vocational rehabilitation over the period of the study was low, with <10% of patients participating in job training or back-to-work programmes.
Satisfaction and Quality of Life
There was a significant increase in reported life satisfaction (p < 0.001), vitality (p < 0.001) and engagement in social relations (p < 0.05; Table 2). Participants were asked to indicate how satisfied they were with their life in general; most felt ‘mixed’ or ‘mostly satisfied’. Only approximately 3% felt ‘terrible’ about their life, while at the other end of the scale >30% felt either ‘pleased’ or ‘delighted’ (Figure 2). We have previously reported the differences between subjective and objective experiences in the quality of life of this same cohort at the beginning of the study [17]. In contrast to the results seen with the disease-specific quality of life measure (QLS), the 15-item AQoL instrument mean baseline score was 0.6 (S.D = 0.3), on a scale from 0 (worst) to 1 (best), and scores were stable during the course of the study.
Life satisfaction of Schizophrenia Care and Assessment Programme participants by study phase.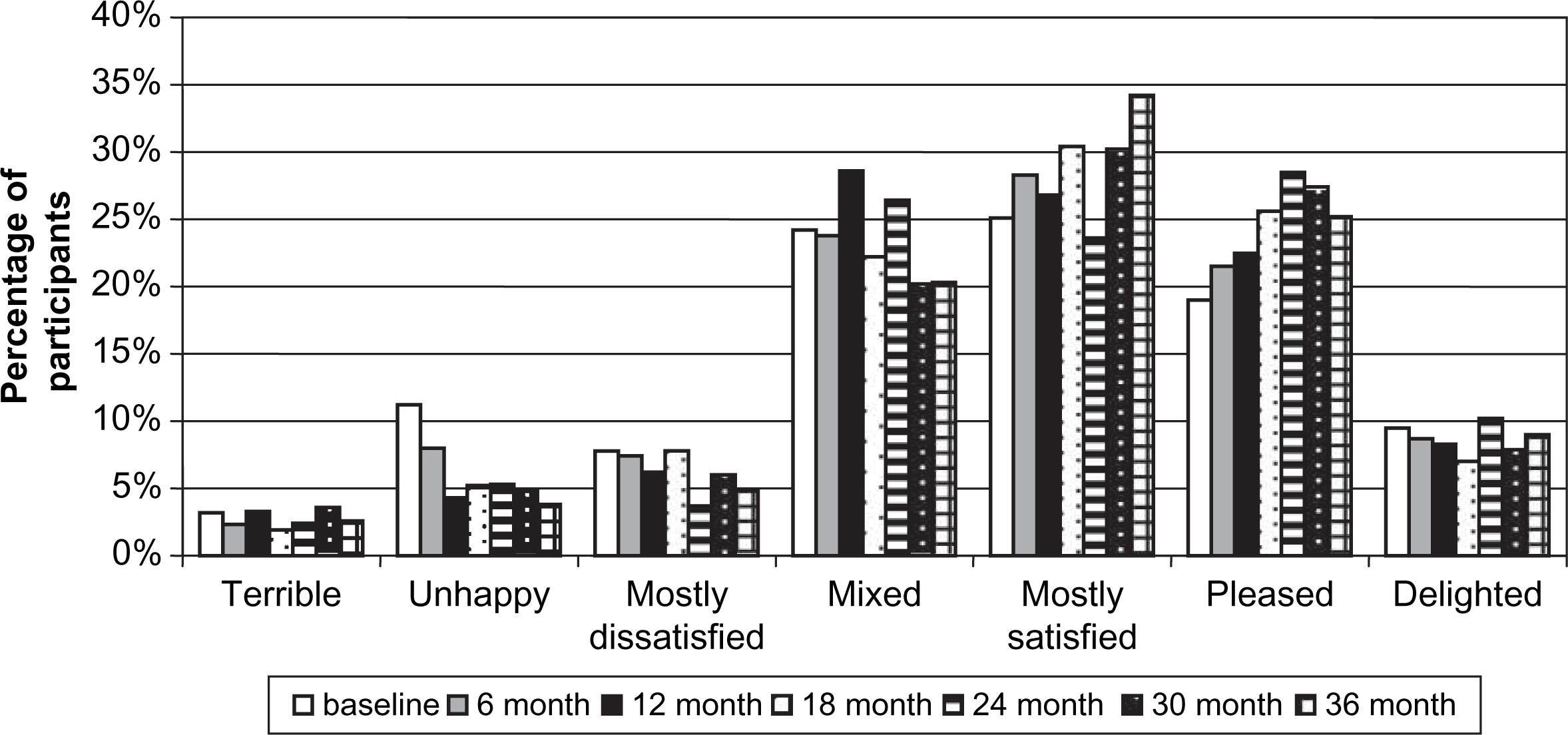
Safety and violence
Over the course of the study there was a reduction in reported victimization (p < 0.05) as well as a reduction in the self-reports of violence committed by the patient group (p < 0.05; Table 2). There was no difference in rates of legal difficulties.
Predictors of outcome
The group was divided into patients who experienced a >20% reduction in total PANSS scores and a >20% increase in total GAF scores from baseline to study end (yes, n = 84; no, n = 180). There was no difference between the groups in baseline demographics (age, sex, education, ethnic background) or illness variables (age of illness onset, number of episodes of illness, diagnosis, and family history of schizophrenia). The group who improved on both dimensions across the study, however, had greater baseline PANSS positive (p < 0.001), negative (p < 0.05) and general (p < 0.001) scores and a lower score on the SCAP-HQ violence subscale (p < 0.01).
Correlations
Correlations were examined between change scores on outcome variables from the four studied domains. As expected, there were significant positive correlations within the outcome domains, for example between the SCAP-HQ Psychiatric Symptoms factor and PANSS positive (r2=0.35, p < 0.001), negative (r2=0.26, p < 0.001) and general (r2=0.45, p < 0.001) symptoms. There were considerably weaker relationships between the items within the outcome domains (SCAP-HQ factor correlations: Table 4). For example, Psychiatric Symptoms correlated with only two of the four Rehabilitation factors, Health-Related Disability (r2=0.20, p = 0.001) and Mental Health-Related Disability (r2=0.28, p < 0.001) but not Instrumental Activities of Daily Living and Daily Activities. Similarly, Psychiatric Symptoms correlated with Life Satisfaction (r2=0.30, p < 0.001) but not with the other Humanitarian factors. There were also limited relationships between Humanitarian and Rehabilitation factors and very few significant correlations between Safety factors and the other variables.
Correlations between SCAP-HQ factors
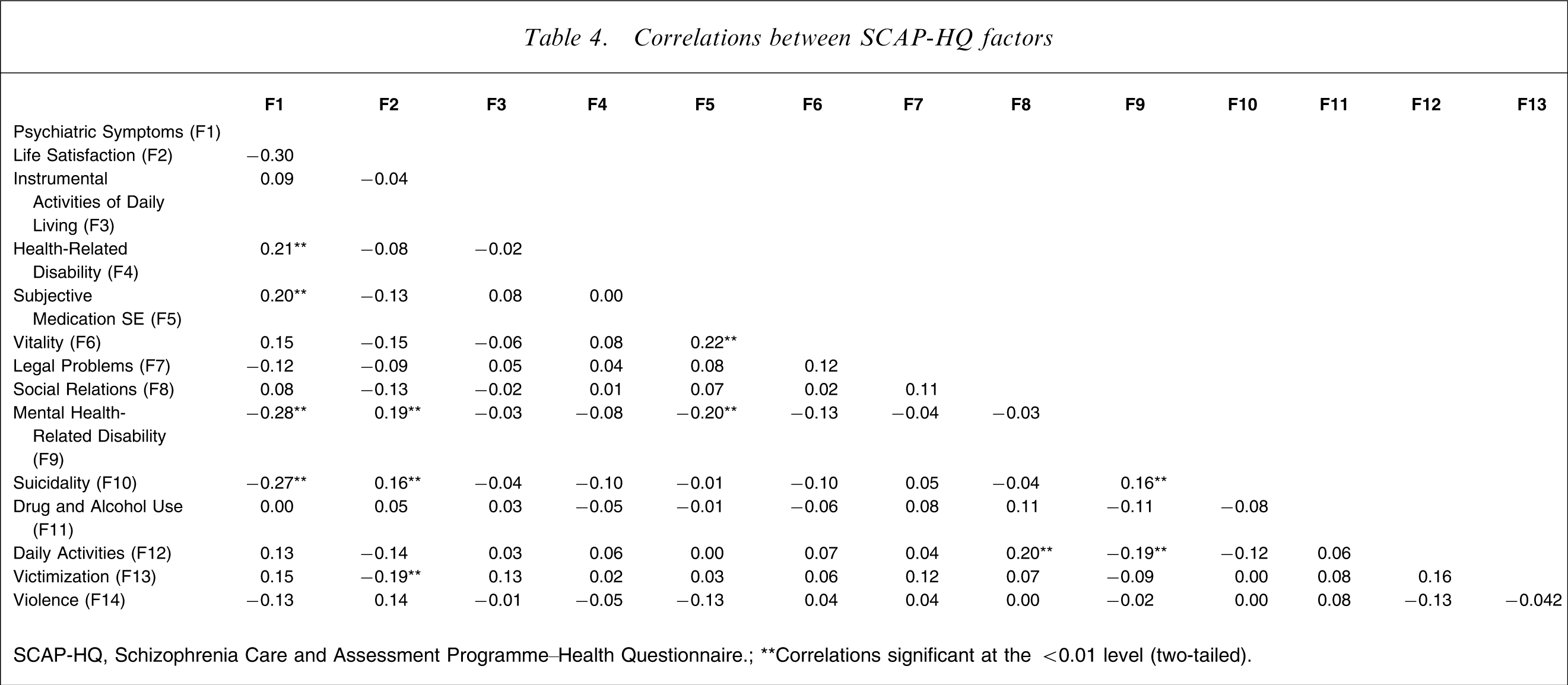
SCAP-HQ, Schizophrenia Care and Assessment Programme–Health Questionnaire; ∗∗Correlations significant at the <0.01 level (two-tailed).
Discussion
This report describes a comprehensive study of outcomes in a large cohort of patients with schizophrenia and schizoaffective disorder followed for 3 years. We observed outcomes across a broad range of variables to provide information on whether these indices of clinical outcomes and response to treatment alter over time.
In general, the patients in the study experienced an overall decline in positive and negative symptoms of schizophrenia, a reduction in general psychopathology as rated by the PANSS and a reduction in severity of depression. There were also improvements in medication-related side-effects (subjective and objectively scored). Importantly, this improvement was accompanied by an increase in functioning and a reduction in mental health-related disability. It was also accompanied by an improvement in patient- and observer-rated quality of life.
There were relationships between changes in severity within the variously assessed domains over time but these were restricted to certain assessed factors and were often of limited magnitude. This implies that improvement across these domains may be relatively independent or associated in a more complex manner not apparent to simple correlation analysis. There was also a significant change in medication provided to participants over the course of the study, away from first-generation or typical antipsychotics and toward the second-generation or atypical antipsychotic agents
The analysis of clinical data in the study provides an interesting and important overview of outcomes for patients with schizophrenia, especially at a time of a shift in prescribing patterns. We cannot, however, make inferential judgements about causal relationships based on these data. The observable pattern of progressive clinical improvement over the 3 years of the study is consistent with studies that report a progressive improvement in clinical outcomes for patients with schizophrenia over time [18]. It must be acknowledged that treatment gains observed in SCAP were more modest than those yielded from modelling studies [19, 20]. Again, however, the value of real-life data and the rich detail it can provide compensates for this shortfall.
Another point of interest to arise from the clinical data was that in the present sample there was an improvement in both positive and negative symptom dimensions with a progressive reduction in negative symptoms across the course of the study. It is commonly thought that there is a dissociation in outcome between positive and negative symptoms: positive symptoms are believed to improve and negative symptoms to worsen over time [21], although not all studies have concurred with this notion [22]. It is possible that the present results reflect the shift to prescribing atypical antipsychotic medications which was also accompanied by a progressive reduction in extrapyramidal side-effect scores. This is especially important because the presence of extra-pyramidal side-effects can confound the assessment of negative symptoms [23, 24]. It is also possible that this pattern of outcome reflects the highly community-based focus of care that may prevent secondary negative symptoms possibly associated with long periods of hospital treatment.
On a less positive note, the improvements seen in many dimensions were not reflected in a substantial improvement in functioning as assessed by rates of employment. Other factors are perhaps at play, such as the lack of evidence-based, readily available, employment rehabilitation programmes in the local community at the time of the study. Based upon evidence drawn from two trials, each with short follow-up periods, Chalaman et al. [25] proposed a hypothetical model to test cost-effectiveness of individual placement support, a specific vocational rehabilitation service. Conclusions were that clinical benefit was not found and the economic cost of the programme was greater than the economic gains. The authors were swift to argue, though, that the model was based upon data from a US sample, and that the psychological tools chosen as well as the brief follow-up period may have meant that effects were underestimated, and clinical change undetected. We echo their assertions that more investigation into the value of vocational training for a largely unemployed population is warranted.
Although there was a relationship between the changes in clinical symptoms over time, there was less consistency in the pattern of change in broader outcomes. In particular, alterations in the four assessed dimensions of outcome were not strongly correlated. This is a novel finding: these broad dimensions of outcome have not been previously tracked in patients with schizophrenia. Furthermore, it has several important implications. First, it reinforces the need to approach outcomes investigations in a multidimensional fashion. We cannot automatically assume that one variable can act as a proxy for other dimensions of outcome, although in certain areas it may be reasonable to assume that improvement in one dimension may be reflected in another (e.g. psychiatric symptoms and life satisfaction).
Second, the weak correlations suggest that treatments specifically focused upon a single dimension alone may not impact upon the other outcomes to a similar degree. This is especially relevant in the area of psychopharmacology, where outcomes have traditionally been defined in terms of positive or other specific psychopathological symptoms [3]. The absence of strong correlations does not necessarily indicate that treatments that target traditional symptoms do not impact on other dimensions. Treatment changes across differing dimensions may occur on a differing trajectory and/or be mediated by other intermediate factors. These relationships require further investigation and the relative benefits offered by a range of interventions targeting dimensions such as life satisfaction, disability and functioning should be quantified as much as is feasible. One such outcome from this approach might be a gradual refocusing of the development of treatments from the therapy of narrowly defined symptoms to the management of more broadly defined aspects of the impact of this illness.
Several issues are worthy of comment. We did not recruit a pure epidemiological incidence cohort and as such the study suffers from the potential impact of selection biases. However, recruitment was directed to widely target the diversity of patients managed in the service and at the time of the study there were very few alternative treatment services for this patient population in the local region except for primary care. Therefore the study was likely to have included a sample representative of that found in a mainstream general psychiatric service. The reasonable retention rate also enhances the capacity of these results to be more widely generalized. The use of person-level measures to quantify outcome may show greater benefit than a more conservative population-level recording, such as disability-adjusted life years (DALYs). The fullness of the information that these measures yield, however, was the impetus behind their inclusion in the methodology. Last, assessment on each domain was conducted at each visit by the same assessor. This could overestimate the strength of the relationships between assessment dimensions but, given the relative lack of close relationships demonstrated, this does not seem to have exerted any major impact.
The longitudinal study of outcomes and the success of interventions for patients with schizophrenia require assessment across a broad suite of domains. Outcome domains should not be considered closely related and the use of complementary and easy-to-implement instruments such as the SCAP-HQ should be a focus for further research. The data from the present study also highlight a population bereft of employment: it would be of considerable interest to observe an introduction of well-resourced and widely available evidence-based programmes for employment rehabilitation for patients with schizophrenia in Australia and elsewhere.
Footnotes
Acknowledgements
We would like to thank all the participants who took part and the staff of Dandenong Area Mental Health Service who facilitated the study. The study was funded by Eli Lilly.