
Abstract
In Australia a number of residential mother–infant units have been established to provide interventions for families with unsettled infants [1–3]. While it is generally acknowledged that postnatal depression occurs in 13% of child-bearing women [4], rates of depression among mothers attending residential mother–infant programmes have been shown to be much higher. Reports about the percentages of residential unit clients who score within the range for depressive symptomatology on the Edinburgh Postnatal Depression Scale (EPDS) [5] have ranged from 34% [6] to 48% [7].
The majority of studies reporting rates of depression in such settings have relied on the EPDS to measure depressive symptomatology. The EPDS is a validated and widely used screening measure for depressive symptoms in the postnatal period [8, 9], but it is not a diagnostic tool [10]. Consequently its widespread use has meant that the prevalence of diagnosable mood disorders in this client group is not clearly understood. The only exception has been the work of McMahon et al. who conducted structured clinical interviews to determine DSM-IV depression diagnoses in a sample of mothers admitted to the Tresillian residential mother–infant centre [2]. These authors reported that since the birth, 62% of mothers met DSM-IV criteria for a major depressive disorder and a further 13% met criteria for a minor depressive disorder. But the results of that study were limited by the inclusion of only women with first-born singleton infants aged 0–3 months. Further, they assessed only depressive disorders and not other disorders common in the postnatal period, such as anxiety disorders.
Prevalence rates for diagnosable anxiety disorders in general postnatal populations have not been extensively researched. However, in a recent review of the postnatal anxiety literature, Ross and McLean reported prevalence rates for perinatal obsessive compulsive disorder (OCD; 2.7–3.9%), post-partum panic disorder (1.3–2.0%) and postnatal generalized anxiety disorder (GAD; 4.4–8.2%) [11]. These figures can be compared to the DSM-IV 1 year prevalence rates for OCD (1.5–2.1%), panic disorder (1.0–2.0%) and GAD (3%) [12], suggesting heightened levels of at least some anxiety disorders in the postnatal period. In a recent Australian study Matthey et al. reported the prevalence of anxiety disorders (panic, phobia, acute adjustment disorder with anxiety – that is, those meeting all criteria for GAD except for that of duration) in a community sample of mothers at 6 weeks post-partum to be 16.2%, with a further 4.2% identified to have comorbid depression and anxiety [13].
Anxiety is known to be a symptom commonly experienced by mothers attending residential mother–infant intervention programmes. McMahon et al. found that 35% of residential unit mothers were classified as highly anxious according to the Spielberger State–Trait Anxiety Inventory (STAI) [2, 14]. Fisher et al. found that 75% of a residential unit sample endorsed the anxiety item of the EPDS (item 4) and 45% fell within the clinical range on the Tension-Anxiety subscale of the Profile of Mood States (POMS) [7, 15]. Furthermore, the recent identification of a distinct anxiety subscale within the EPDS (three items) [16], accounting for 38% of the total EPDS score variance [17], highlights the role of anxiety symptoms in post-partum depression. However, as with depression, the use of self-report anxiety symptom measures in most studies has meant that rates of diagnosable anxiety disorders in this patient group are unknown.
The comorbidity between anxiety and depression has been well established in the general psychiatric literature [18–23] and this has also been shown to be the case in the postnatal period [17, 24–26]. But to date there has been little research investigating the comorbidity between anxiety and depressive disorders in residential mother–infant programmes.
The aim of the present study was to fill these gaps and (i) determine the rate of depressive and anxiety disorders in a residential mother–infant programme for unsettled infant behaviour; and (ii) examine the comorbidity between depressive and anxiety disorders in this population. We hypothesized that (i) rates of current DSM-IV depressive and anxiety disorders among women admitted to a residential mother–infant intervention programme for unsettled infant behaviour will be higher than in other community post-partum samples; and (ii) rates of comorbidity between depressive and anxiety disorders will be high, as is the case in general community samples.
Methods
Participants
The Karitane Residential Family Care Unit (RFCU) is a 10-bed parent–infant unit located in South West Sydney, Australia. The 5 day multidisciplinary programme provides intensive interventions for families with complex early parenting difficulties. Two hundred and forty-three English-speaking women with infants aged 2 weeks–12 months admitted to the Karitane RFCU between September 2005 and April 2006 were invited to participate in the study. Twelve women were not asked to participate because they were either not proficient in speaking English (n = 4) or because their infants were very young, that is, <2 weeks old (n = 8). In total, 167 women (69% of eligible women) agreed to participate. Of the 76 who were asked but did not participate, 25 agreed but were subsequently prevented from doing so because of practical constraints associated with the admission (e.g. insufficient time) and 51 declined. Common reasons given by clients for not participating was that they felt too overwhelmed by the admission to participate in research, that they did not want to have to talk about how they were feeling or that they did not have time to participate. The mean±SD EPDS score of women who participated in the study (10.0±5.2) was not significantly different from the mean±SD EPDS score of the entire sample of eligible women admitted to the RFCU during the given time period (obtained from routinely collected de-identified EPDS data records; 10.5±5.4; t(165) = − 1.4, p = 0.18).
Procedure
During their admission, participants were interviewed using the Depression and Anxiety modules of the Structured Clinical Interview for DSM-IV diagnosis (Research version) (SCID-I) [27]. EPDS scores (completed routinely as part of the RFCU admission) were obtained from client clinical files. Ethics approval was obtained from the Sydney South West Area Human Research Committee and University of Sydney's Human Research Ethics Committee.
Measures
Structured Clinical Interview for DSM-IV diagnosis
The SCID-I is a semi-structured diagnostic interview for current and lifetime history of DSM-IV disorders [27]. The SCID-I has been used widely in psychiatric research studies and clinical settings, including pregnancy and post-partum samples [28–30]. The SCID-I has demonstrated interrater reliability, with kappa coefficients for diagnoses of major depressive disorder ranging from 0.67 [30] to 0.72 [31] and 0.80 [32]. Kappa coefficients for anxiety disorder diagnoses (0.63 for GAD, 0.63 for social phobia, 0.57 for OCD, 0.65 for panic disorder) have also shown the SCID to be a reliable diagnostic tool [32]. In the current study participants were administered sections of the Mood episodes module (current and past major depressive episode, current and past manic or hypomanic episode, current dysthymia) and Optional module (minor depressive disorder, symptomatic details of past major/minor depressive episodes). Participants were also asked screening questions relating to lifetime experience of panic disorder, social phobia, specific phobia, OCD, GAD and anxiety disorder not otherwise specified (ADNOS). Corresponding sections of the Anxiety disorders module were administered when individuals responded positively to screening questions. Although previous authors have altered the DSM-IV GAD duration criteria in postnatal women to identify generalized anxiety occurring since childbirth [13, 24, 33], in the present study a diagnosis of GAD was given when all DSM-IV criteria were met (including 6 months duration). A diagnosis of ADNOS was given in cases (i) in which there was evidence of clinically significant excessive and uncontrollable worry, but where the worry was limited to the specific topics of the baby or their role as mother (i.e. worry was not generalized to a number of different topics), or (i) in which they fulfilled all DSM-IV criteria for GAD except for duration.
Edinburgh Postnatal Depression Scale
The EPDS is a 10-item self-report measure for depressive symptoms in the perinatal period [5]. The EPDS yields scores ranging from 0 to 30. For English-speaking women, EPDS scores of 13 or more are considered indicative of likely major depression and scores between 10 and 12 of likely minor depression [5]. The validity and reliability of the EPDS have been demonstrated (split half reliability = 0.88, internal consistency α = 0.87) [10].
Statistical analyses
Descriptive statistics and frequency analyses were used to examine demographic characteristics of clients and to determine rates of disorders. A one-sample t-test was used to compare mean EPDS scores of study participants and the entire sample of eligible women admitted to the RFCU during the given time period. Data were analysed using SPSS for Windows version 13.0 (SPSS, Chicago, IL, USA).
Results
Demographics
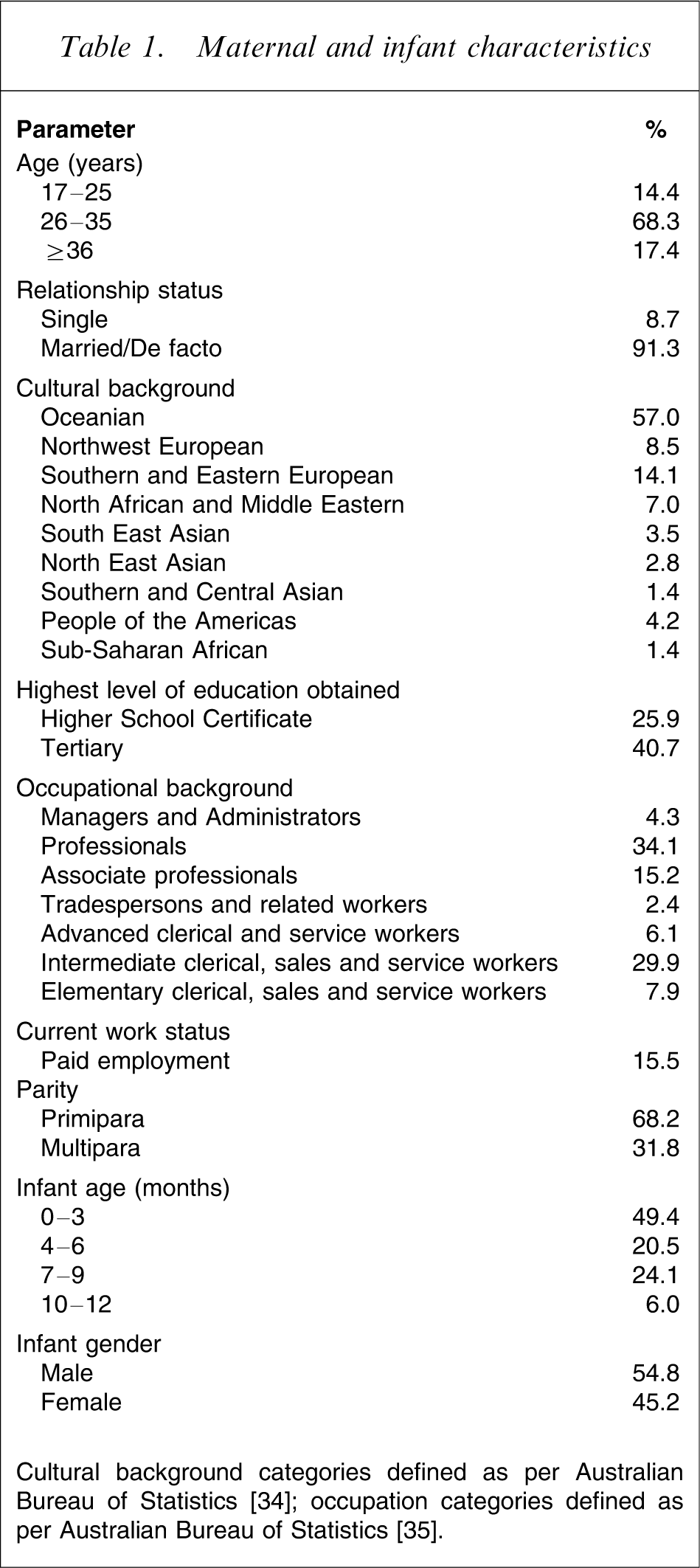
Demographic characteristics for participants are shown in Table 1. The mean±SD maternal age was 31.4±5.1 years and the range was 17.2–44.1 years. There were 10 sets of twins in the sample and the mean±SD infant age was 5.3±3.2 months, with a range of 0.7–11.9 months.
Maternal and infant characteristics
Depression
Table 2 shows the percentages of women in this sample who met criteria for major or minor depression (i) at the time of the interview, (ii) at any time since the start of their most recent pregnancy (including at the time of the interview) and (iii) at any time throughout their lifetime (including at the time of the interview). The mean EPDS score was 10.0
Prevalence of depressive disorders
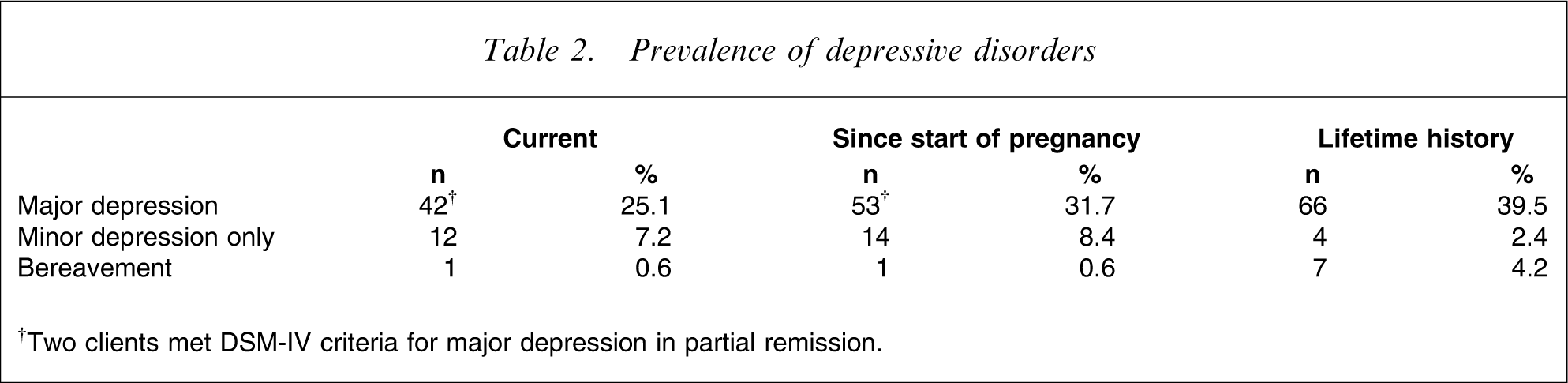
†Two clients met DSM-IV criteria for major depression in partial remission.
Timing of depression onset in relation to childbirth†
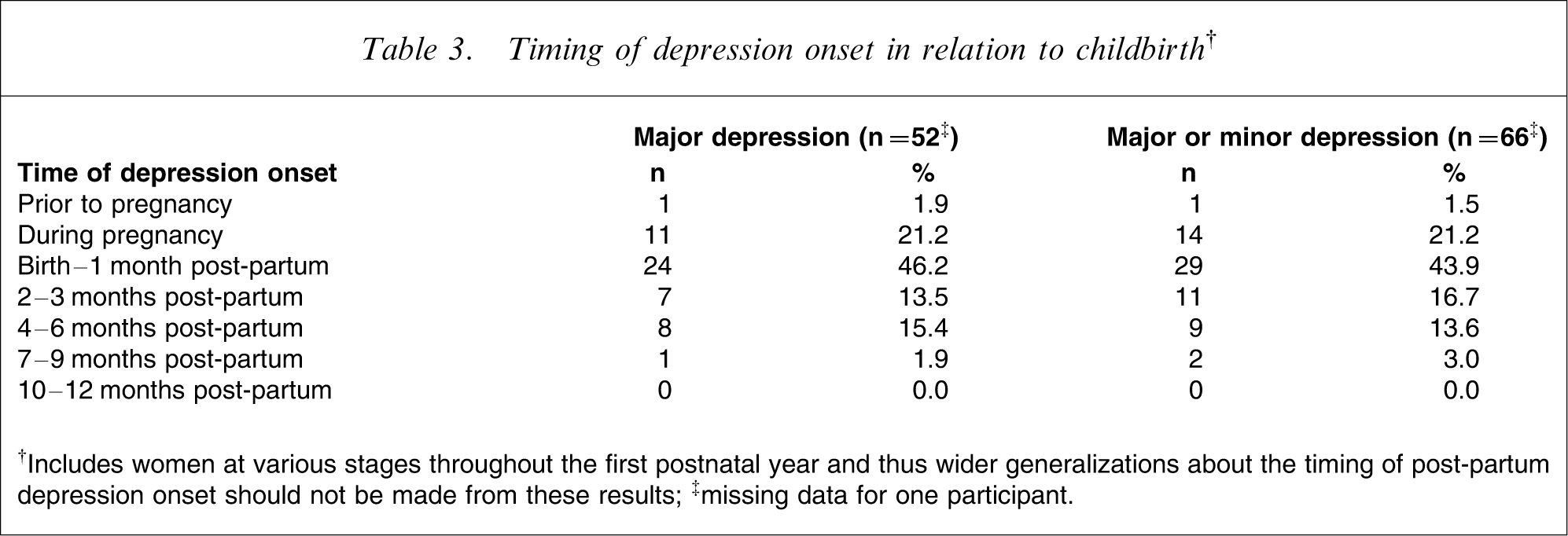
†Includes women at various stages throughout the first postnatal year and thus wider generalizations about the timing of post-partum depression onset should not be made from these results; ‡missing data for one participant.
Anxiety
The frequencies of current and lifetime anxiety disorders are shown in Table 4. Almost one-third of clients met criteria for at least one current anxiety disorder, and many (12.6%) met criteria for more than one anxiety disorder. All of the anxiety disorders were well represented. Of particular note was the frequency of excessive and uncontrollable worry, with more than one-fifth of clients (n = 36) meeting criteria for either GAD or for ADNOS (diagnosed where there was evidence of clinically significant excessive and uncontrollable worry about the baby or about their role as mother). Some of these women (14.3%) recalled the onset of the worry as prior to having children, and the same number again (14.3%) recalled worry onset at the time that their previous children were born. However, the majority recalled the time of symptom onset as being either during their most recent pregnancy (20.0%) or immediately following the birth (51.4%).
Prevalence of anxiety disorders
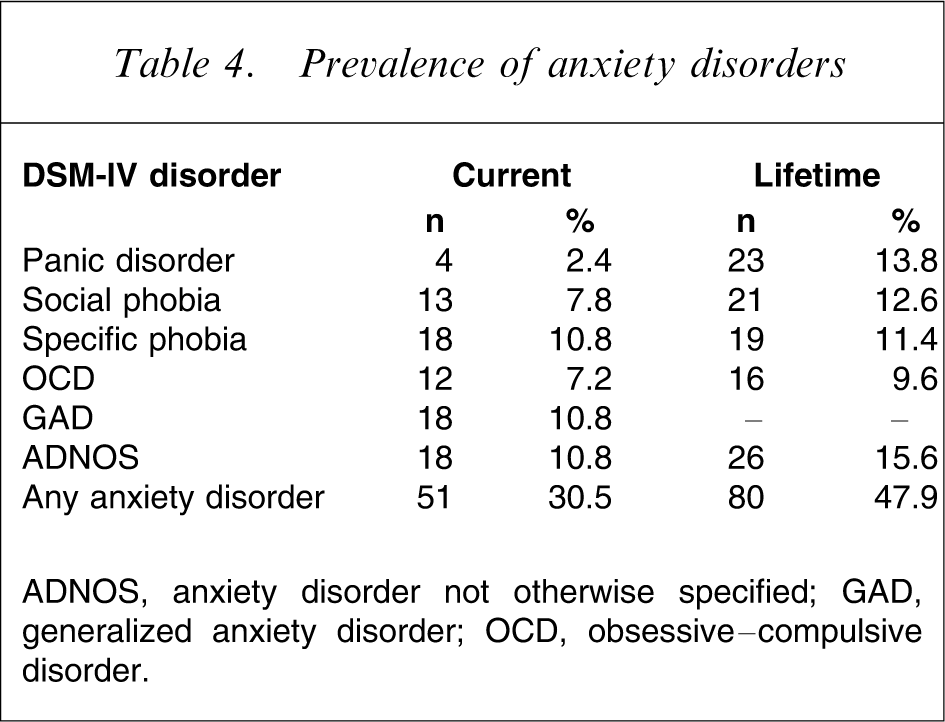
ADNOS, anxiety disorder not otherwise specified; GAD, generalized anxiety disorder; OCD, obsessive–compulsive disorder.
Comorbidity
Approximately half of the women in the sample (52.1%) met criteria for either a current anxiety disorder or for depression (major or minor) since the start of their pregnancy. Of these 87 women, 31 (35.6%) met criteria for a current anxiety disorder and for depression since the pregnancy (major or minor), 20 (23.0%) met criteria for an anxiety disorder only and 36 (41.4%) met criteria for depression only. Of the 51 women who met criteria for a current anxiety disorder, 31 (60.8%) had also met criteria for depression since the start of their pregnancy (major or minor) and 20 (39.2%) had not. Of the 67 women who met criteria for depression since the start of their pregnancy (major or minor), 31 (46.3%) also met criteria for an anxiety disorder.
Discussion
This study is the first to report rates of DSM-IV depressive and anxiety disorders among mothers with infants aged 0–12 months admitted to a residential programme for unsettled infant behaviour. As hypothesized, results show elevated rates of depressive disorders compared with normative postnatal populations, with 25.1% meeting criteria for a current diagnosis of major depression and 31.7% meeting criteria since the birth. Similarly high rates of anxiety disorders were found. High levels of comorbidity were confirmed, with 60.8% of those with a current anxiety disorder also experiencing a mood disorder since the birth.
Despite careful attention to methodology, a few limitations should be borne in mind when interpreting the results. First, the recruitment rate (69%) was not optimal. However, it was comparable to recruitment rates of 59% [6], 75% [7] and 80% [2] obtained for studies in similar settings. Furthermore, there were no significant differences between EPDS scores of participants and non-participants. Few women (n = 4) were excluded because they were non-English speaking. Hence, results are likely to be representative of the client group. In light of the multicultural nature of the South Western Sydney population, these figures highlight the problem of accessibility and/or utilization of the service by women from non-English-speaking backgrounds. A second limitation is the cross-sectional design. Participants ranged from 1 to 12 months post-partum. The current study can only report on disorders experienced by the time of the interview, thus offering no information about participant experiences throughout the remainder of the first postnatal year. Rates in the present study will therefore be an underestimation of true prevalence rates for the first 12 post-partum months, particularly because many women reported delayed onset of depressed mood. These limitations notwithstanding, the current study has a number of strengths including a large sample size, a wide infant age range (0–12 months) and utilization of both a questionnaire measure and a diagnostic tool for DSM-IV diagnosis.
The present study confirms that rates of depression in residential mother–infant settings are higher than in community postnatal samples, where it is generally accepted that approximately 13% of women develop major postnatal depression [4]. Nonetheless, rates were lower than those given in the only previous study reporting rates of depression in a similar service (62% major depression, 13% minor depression) [2]. One difference between the studies was that McMahon et al. limited their sample to women with infants aged 0–3 months. But, because rates of major and minor depression for mothers of infants aged 0–3 months in the present study were still lower (25.6% and 12.2%, respectively) than in the McMahon et al. sample, this is unlikely to explain the differences. In all other respects the studies are similar, making it difficult to know the reason for such a discrepancy. Interestingly, rates of likely depression according to the EPDS in the present study were similar to those of previous studies [1, 6, 7]. Regardless of the reason for the discrepancy, both studies are consistent in demonstrating substantially higher rates of major depression in women presenting to residential services for unsettled infant behaviour.
The present study also provides new information about rates of anxiety disorders among women admitted to residential programmes for unsettled infant behaviour, showing that 30.5% meet diagnostic criteria for an anxiety disorder, with panic disorder, social phobia, specific phobias and OCD all being represented. The prevalence of clinically significant uncontrollable and excessive worry was particularly noteworthy, with one in five patients meeting criteria for GAD (10.8%) or ADNOS (10.8%). This confirms findings by Wenzel et al., who reported that while 4.4% of an 8 week postnatal sample met full diagnostic criteria for GAD, a further 27.9% reported subsyndromal GAD symptoms [33].
The current study also highlights two issues relevant to the diagnosis of depressive and anxiety disorders in postnatal populations. The first relates to the timing of symptom onset. DSM-IV diagnosis of major depressive disorder with post-partum onset requires symptom onset to be within the first postnatal month. In practice, researchers and clinicians often take a broader approach, commonly referring to any depression beginning within the first 12 months as postnatal depression [36]. The present results support this broader definition because symptom onset was within the first post-partum month for less than half (46.2%) of those who developed major depression in the first post-partum year. A further 30.8% reported symptoms after the first postnatal month and 23.1% reported symptom onset during pregnancy. The second issue relates to postnatal worry. The present study identified a large number of women who were experiencing significant levels of worry but who did not meet criteria for GAD (10.8%) because of the restricted focus of the worry (confined to the topics of the baby or motherhood). Where such worry was judged to be of clinical significance, a DSM-IV classification of ADNOS was given. Without any standardized guidelines for classifying such symptoms in DSM-IV, alternative diagnoses such as ‘adjustment disorder with anxious mood’ or ‘subsyndromal GAD’ could, and have, been utilized in other studies [13, 24, 33]. This phenomenon therefore seems worthy of further investigation.
Overall, the frequency with which depressive and anxiety disorders occurred in the present clinical population highlights the important role that psychological and psychiatric interventions can have in services for women presenting with unsettled infants. It is also likely that in many cases in which postnatal psychiatric disorders are present, early identification and intervention could decelerate or prevent the establishment of a self-sustaining cycle of maternal distress and infant unsettledness. Early intervention would likely have significant positive consequences for women and infants, and decrease the need for residential mother–infant programmes. Last, the fact that postnatal worry occurred so commonly in this sample suggests that further investigation of postnatal worry is warranted.
Footnotes
Acknowledgements
This research was supported by the National Health and Medical Research Council of Australia (NHMRC), Karitane, and the women who kindly participated.