
Abstract
While becoming a parent is generally a rewarding life experience, this major life transition can be a trigger for depression and/or anxiety. The issues faced by men during this life transition have taken second place to the extensive work on women's distress, especially postnatal depression. The First-time Fathers’ Study was a prospective study of the specific issues faced by men during their transition to parenthood. This study demonstrated that there was no increased risk for men of developing depression after the birth of their first child but found that the men experienced significant distress when their partners were pregnant [1].
This paper examines in more detail associations of this psychological distress in first-time fathers during pregnancy. In particular, we wished to examine whether this distress was associated with a general vulnerability to anxiety and depression (vulnerability characterized by early life adversity, poor personality functioning and inadequate social support [2]). We present associations in relation to psychological, personality, gender role function, interpersonal relationships and lifestyle factors.
Methods
A longitudinal cohort design was used and the men were recruited into the study when their partners booked into the antenatal clinics of two large Australian public hospitals. The men completed a baseline assessment by postal questionnaire when their partners were approximately 20 weeks pregnant and were then reassessed at 3, 6 and 12 months after the baby was born. Only data for the initial assessment conducted during the antenatal period are presented in this paper. Further details regarding recruitment of participants and the assessments conducted at other time points can be found in Condon et al. [1].
Instruments
The men were asked to complete a series of questionnaires at the baseline assessment that covered demographic features, their attitudes towards pregnancy and childbirth, symptom severity, personality attributes, intimate relationship, alcohol consumption, lifestyle and quality of life.
Symptom measures
The General Health Questionnaire (GHQ) was used as the key measure of psychological distress [3]. A cut-off point of ≥ 5 was used to distinguish between cases and non-cases with those scoring ≥ 5 being classified cases.
The Hopkins Symptom Checklist (HSCL-90), containing 90 items, provides reliable and valid measures of symptomatology on nine subscales. Those reported upon in the present paper include retarded and agitated depression, anger–hostility, phobic anxiety and somatic symptoms [4].
The Self-Assessment of Irritability Scale (SAIS) was used to measure inwardly and outwardly directed irritability [5].
The Edinburgh Postnatal Depression Scale (EPDS) is a 10-item self-report scale that was developed to screen for postnatal depression. It has been shown to be valid for men and can also be used antenatally [6].
Alcohol use
Alcohol intake was assessed using the Alcohol Use Disorders Identification Test (AUDIT) with a cut-off point of >7 used to identify at-risk drinkers [7]. The CAGE alcohol questionnaire [8], a simple 4 item screening tool designed to detect alcoholism focusing on ‘Cutting down’, ‘Annoyance by criticism’ and ‘Eye-openers’, was also utilized.
Personality attributes
The Eysenck Personality Questionnaire (EPQ) was used for assessing the personality traits of neuroticism and extraversion [9].
The Defence Style Questionnaire (DSQ) measures the major ego defence styles and allows these to be grouped into mature, neurotic and immature defence styles [10].
The Bem sex role inventory measures psychological masculinity, femininity and androgyny [11].
Relationship and social support measures
The Dyadic Adjustment Scale (DAS) is a 32-item scale, with four subscales that measure dyadic cohesion, consensus, satisfaction and affectional expression [12].
The Sarason 12-item Social Support Scale (SSSS) measures the amount of social support a person perceives themselves to receive, and how satisfied they are with that support [13, 14].
The Intimate Bond Measure (IBM) is a 24-item scale that measures perceived caring and controlling in a partner on two subscales [15].
The Parental Bonding Instrument (PBI) was used to access the men's perceptions of how their own parents behaved towards them for the first 16 years of their life [16].
The men's relationship to the unborn baby was assessed using the Paternal Antenatal Attachment Scale [17].
Concerns about pregnancy
The men were asked a series of questions about whether the pregnancy was planned or unplanned, whether they had clear or unclear expectations about the birth, and whether they were aware of positive or negative experiences of other men in the transition to fatherhood.
Life events
A brief version of the Tennant and Andrews life event scale [18] was used to identify stressful life events in the past 3 months. [19]. The total number of events scored as occurring provided the life event score.
Statistical analysis
Data were analysed using SPSS 13.0 for Windows (SPSS, Chicago, IL, USA). A cut-off score of > 4 on the GHQ was used to discriminate between cases of psychological distress and non-cases; subsequent analyses utilized this dichotomization. Data were analysed using one-way ANOVA and independent samples t-tests to determine the differences between cases and non-cases in the personality, relationship, and lifestyle variables. The data were cleaned as per methods described in Condon et al. [1].
A series of stepwise multiple regression analyses were used to investigate the association between psychological distress (as measured by the raw GHQ score) as the dependent variable and (i) personality, and (ii) relationship and social support variables. Significant variables from these analyses were then entered into a hierarchical multiple regression, again with the raw GHQ score used as the dependent variable.
Results
Sample characteristics
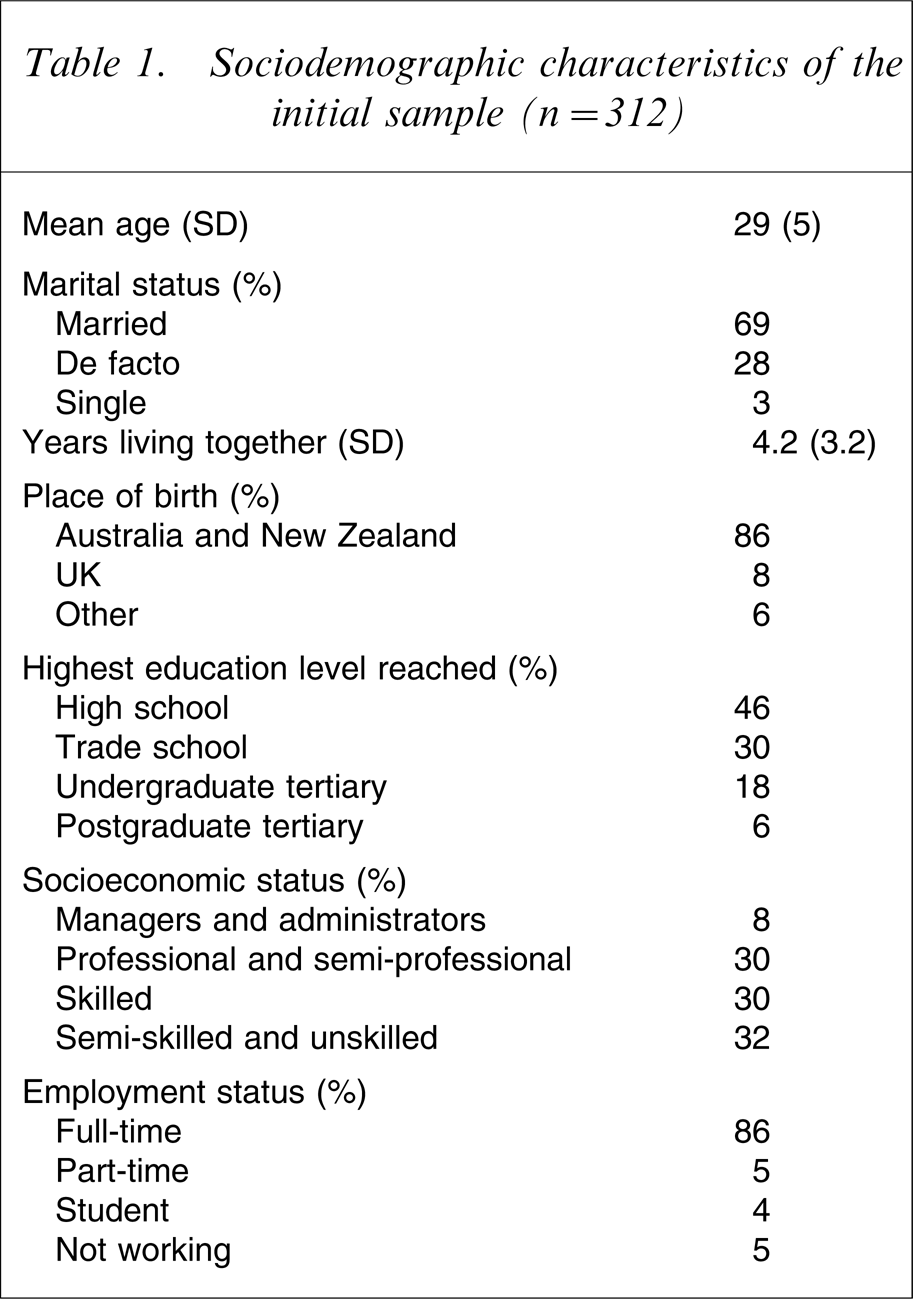
The sociodemographic profile of the sample is reported in Table 1. Of the 312 men initially assessed, 68% of the men were married to their partners, 29.4% were in a de facto relationship and 3% remained single. The majority were born in Australia and New Zealand (86%), or in the UK (8%). The highest levels of education achieved by the men were high school (46%), trade certificate (30%), tertiary education (18%), and 6% had completed a higher degree. Thirty-two per cent were semi-skilled or unskilled workers, 30% were skilled workers, 30% were in professional or semiprofessional jobs and 8% were managers or administrators. Five per cent of the men were not working and 4% were still students. They had been living with their partner on average for approximately 4 years (range = 0–15 years).
Sociodemographic characteristics of the initial sample (n = 312)
The mean GHQ score was 2.5 (SD = 3.9). For the purposes of the present study, men who scored ≥ 5 on the GHQ were considered to be cases. Of the 312 men who completed the baseline assessments, 18.6% scored ≥ 5 on the GHQ. There was no significant difference in age between the cases (28.7 years) and non-cases (29.0 years), or any other sociodemographic variables (country of origin, educational level, employment status and income). The non-cases had been living with their partners significantly longer (51.9 months) than the cases (39.8 months; F = 4.95, p < 0.05). There was a significant difference between the marital status of the two groups: 74% of non-cases were married versus 53% of the cases, while 23% of the non-cases were in de facto relationships versus 41% of the cases (χ2=10.2, p < 0.05)
Univariate analyses
We compared the cases with the non-cases on the baseline measures, and the results are given in Tables 2 and 3. As shown in Table 2 the cases scored significantly higher on the EPDS, AUDIT, CAGE and the total and subscale scores on the HSCL-90.
Symptom and quality of life measures of psychological distress (mean, SD)
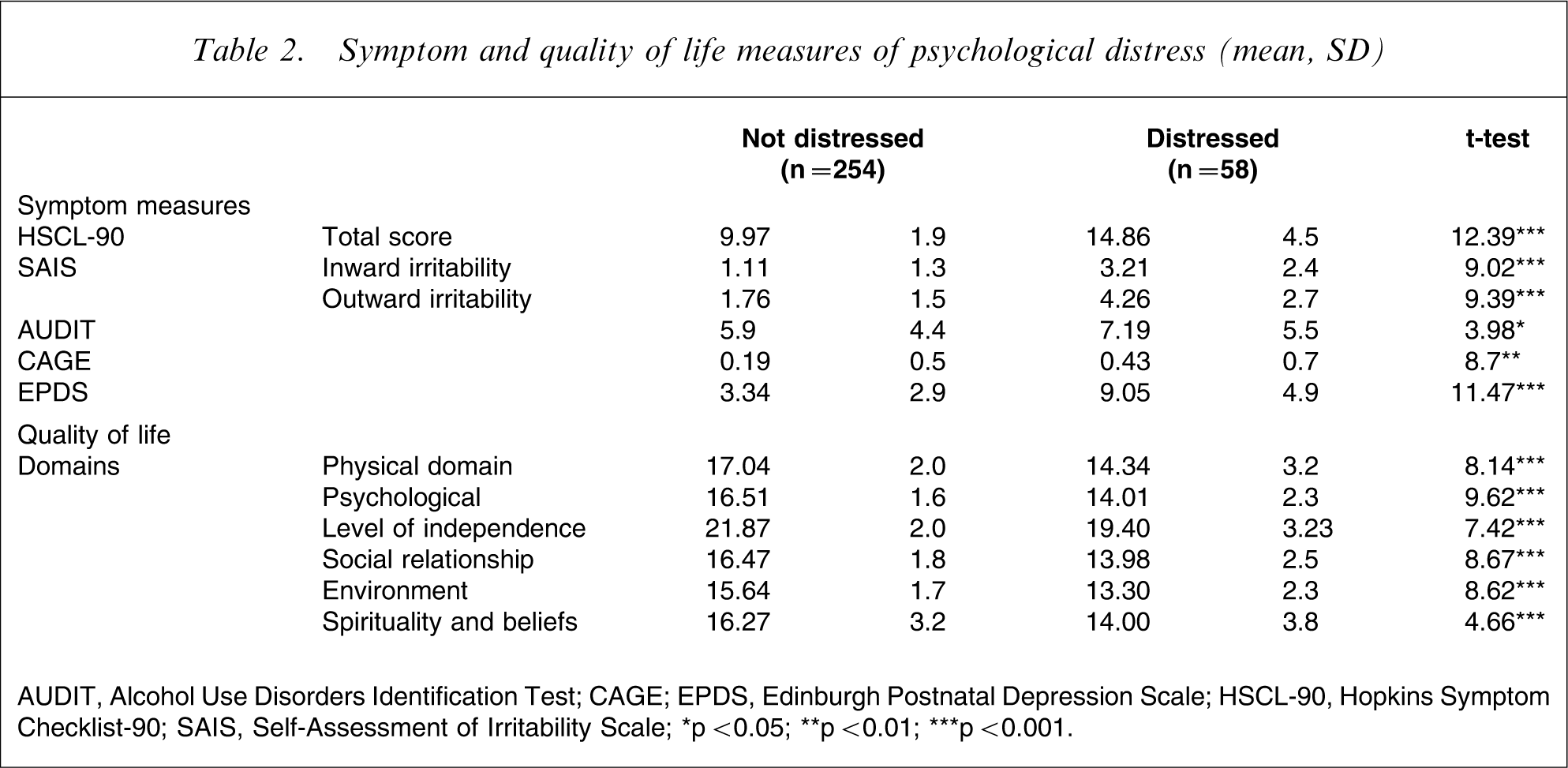
AUDIT, Alcohol Use Disorders Identification Test; CAGE, XXX; EPDS, Edinburgh Postnatal Depression Scale; HSCL-90, Hopkins Symptom Checklist-90; SAIS, Self-Assessment of Irritability Scale; ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Relationship and personality measures of psychological distress
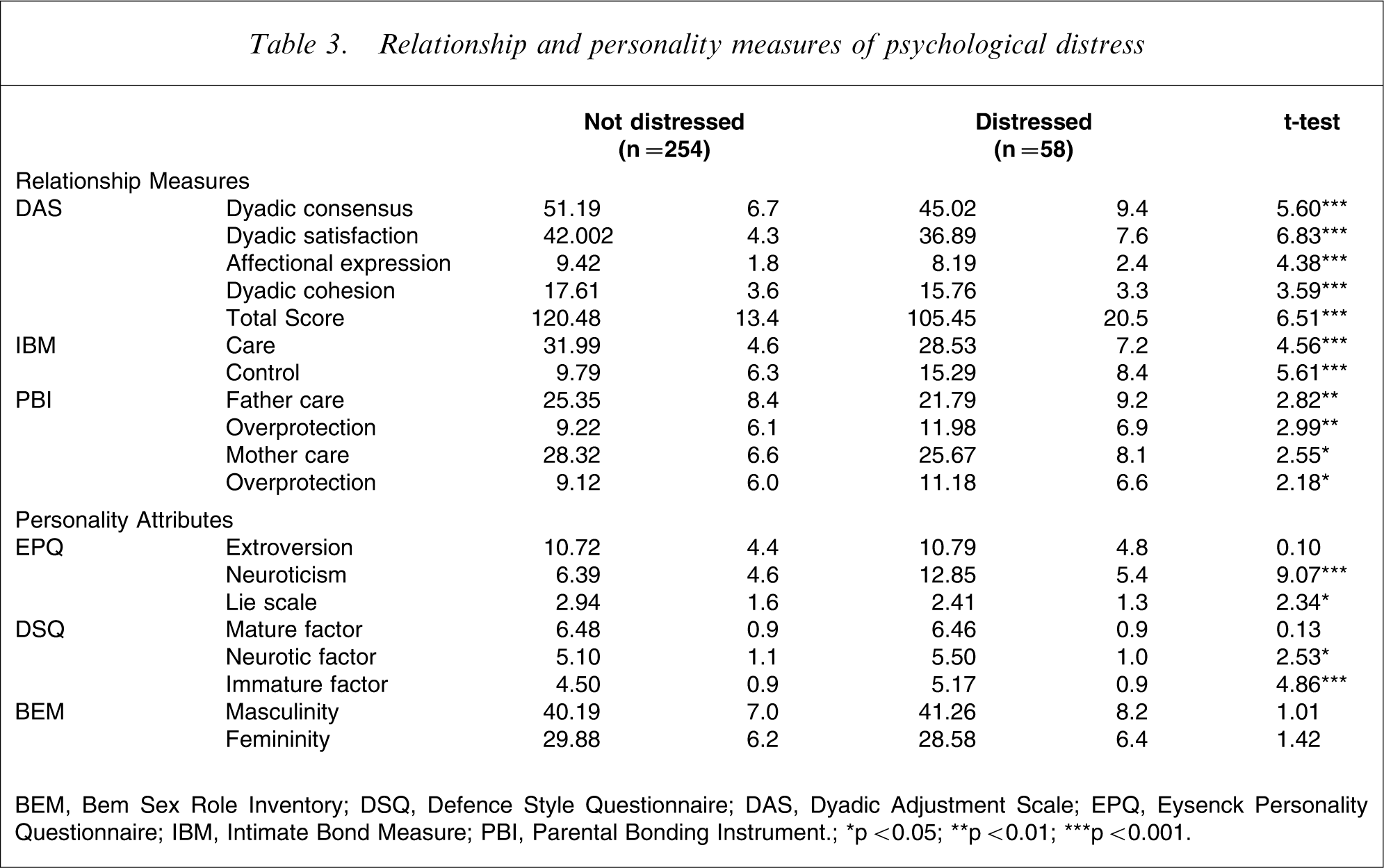
BEM, Bem Sex Role Inventory; DSQ, Defence Style Questionnaire; DAS, Dyadic Adjustment Scale; EPQ, Eysenck Personality Questionnaire; IBM, Intimate Bond Measure; PBI, Parental Bonding Instrument.; ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
The cases reported a lower quality of life as measured on the World Health Organization Quality of Life (WHOQOL), scoring significantly lower on all of the domains (Table 2).
With regard to their intimate relationships the cases reported a poorer quality relationship on the DAS (and its subscales), and perceived their partners to be more uncaring and more controlling than the non-cases on the IBM, as shown in Table 3.
The distressed men were significantly more neurotic but not more introverted than the non-cases. They tended to use more immature defences than the non-distressed men, and, to a lesser extent, more neurotic defences, whereas there were no differences between groups in their use of mature defences. There were no differences in levels of masculinity and femininity on the BEM sex role inventory between cases and non-cases. The distressed men perceived their parents to behave towards them as less caring and more overprotective than the non-distressed men.
The men were asked a series of questions about their partner's pregnancy, breast-feeding and the birth of the baby. There were no differences in the responses between the distressed and non-distressed men with regard to their partner's intentions about breast-feeding. With regards to the delivery there were no differences between distressed and non-distressed men and their intentions about whether to be present at the birth or not (or their reasons for this), their expectations regarding the amount of pain and distress their partner would experience and how stressful they considered the birth to be. There were no differences in the type of information they had received about the birth or their expectations of the baby's gender.
There were significant differences, however, between the distressed and non-distressed men for three variables (Table 4). The distressed men were more likely to have a partner with a pregnancy that was unplanned or left to chance (50.9%) than the non-distressed men (35.3%; odds ratio (OR) = 1.9, 95% confidence interval (CI) = 1.1–3.4). They were also more likely to have unclear birth expectations (30.9%) than the non-distressed men (20.6%; OR = 1.7, 95%CI = 0.9–3.3), and they were more likely to have been given reports of negative or mixed experiences from other men (28.8%) than the non-distressed men (8.8%; OR = 3.8, 95%CI = 1.6–8.9).
Prevalence of risk factors first-time fathers according to psychological distress
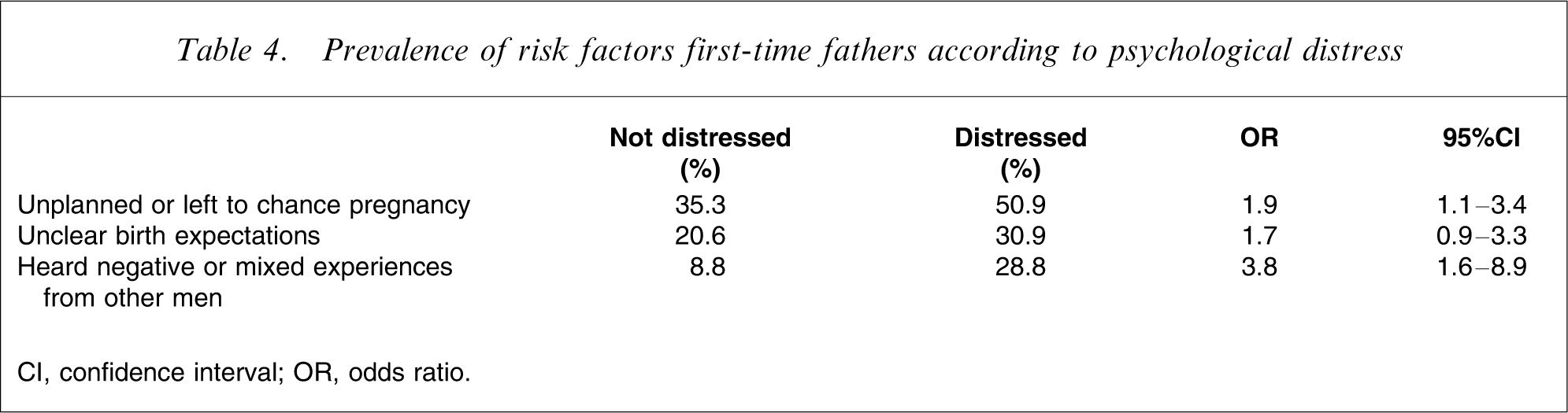
CI, confidence interval; OR, odds ratio.
Multivariate analyses
On each of the variables associated with the men's psychological distress we conducted a hierarchical multiple regression analysis. Variables were entered in blocks; the order in which the blocks were run was based on their theoretical chronological order. Thus, parenting style was entered as the first block, followed by personality style, then social support and intimate relationship variables, with life events, antenatal attachment and irritability entered last.
Because personality can be affected by mood state, the regression was re-run, this time forcing in current mood state first (using the HSCL-90 total score as a measure of mood state).
Before we could run this hierarchical regression analysis there needed to be some rationalization of the variables to be used. We used different measurements of personality, (neuroticism, extraversion, defence style, masculinity, femininity) and two separate measures of the quality of the intimate partner relationship, (the DAS and IBM). Stepwise multiple regression analyses were conducted first on the personality variables, with the GHQ score as the dependent variable, in order to pick out significant personality variables to use in the hierarchical regression model. The stepwise regression model was highly significant (F(2,344)=60.51, p < 0.000) and accounted for 33% of the variance, with neuroticism (β = 0.45) and use of the immature ego defence factor (β = 0.13) being the significant variables. When this analysis was rerun, this time forcing in mood state (the SCL-90 total score) first, only neuroticism remained as a significant predictor on GHQ score. Neuroticism and immature ego defences were selected as the personality variables to be used in the subsequent hierarchical regression analysis.
A similar stepwise regression analysis was run on the partner relationship measures. The quality of the intimate relationship emerged as being highly significant (F (2, 279)=48.0, p < 0.001, R2=0.25), with low total dyadic satisfaction (β = − 0.40) and reporting a partner as providing low care on the IBM care scale (β = − 0.14) being the significant variables. These two variables were used in the hierarchical regression analysis.
The men's perceptions of their own parenting (PBI subscale scores) were entered as the first block of the hierarchical regression. While the overall regression model was significant (F(4,275)=2.51, p < 0.05, R2=0.02), none of the PBI variables reached significance. In the second block, neuroticism and immature defences were entered into the model. There was a significant improvement in the model, R2(change) = 0.30, with a highly significant regression including both neuroticism (β = 0.50) and immature factor (β = 0.13). The amount of, and satisfaction with social support was entered next, again with a significant improvement of the model, R2(change) = 0.05. Dissatisfaction with support (β = − 0.25) was the significant contributing variable. The addition of dyadic satisfaction and IBM care scales again improved the model in the next block, with a further increase in the R2 of 0.019, with dissatisfaction with the intimate relationship being the significant variable (β = − 0.15). In the final block, the number of life events the person experienced in the previous year was entered, to determine if external stress over and above the pregnancy made an additional contribution to the men's distress. The final model was highly significant (F(10,217)=13.23, p < 0.001) with a final R2 of 0.38. The coefficients for the final model are shown in Table 5, with significant contributions to the GHQ score being for neuroticism (β = 0.31), dissatisfaction with social support (β = − 0.18), and the number of life events reported (β = 0.20).
Final hierarchical multiple regression model of predictors of psychological distress in first-time expectant fathers
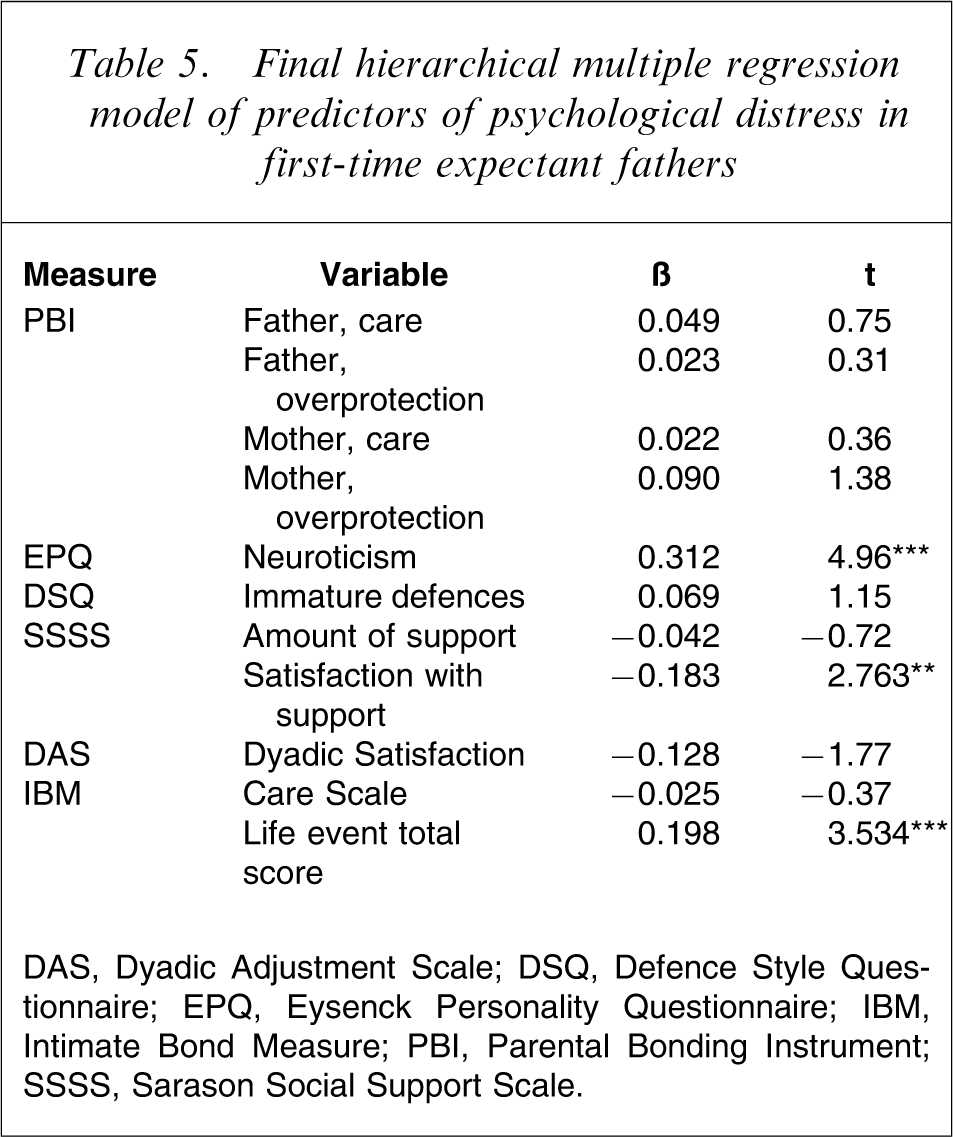
DAS, Dyadic Adjustment Scale; DSQ, Defence Style Questionnaire; EPQ, Eysenck Personality Questionnaire; IBM, Intimate Bond Measure; PBI, Parental Bonding Instrument; SSSS, Sarason Social Support Scale.
Discussion
In this paper we have explored the associations with psychological distress among a group of expectant fathers. We had previously reported that the time of maximal distress among this cohort of men going through the transition to first-time fatherhood was when their partners were in the early stages of the third trimester of pregnancy [1]. The men were categorized according to their scores on the GHQ-28, using the conventional cut-off of ≥ 5, into cases of distress and non-distress. A total of 18.6% of the men were categorized as cases; this is higher than the commonly reported prevalence rates for the common mental disorders (anxiety and mood disorders) reported for men, such as the prevalence rate of 7.1% for anxiety disorders and 4.2% for affective disorders [20]; or the New Zealand mental health survey, which reported 17.1% point prevalence for any mental disorders among men [21].
It must be noted that caseness on the GHQ does not equate to caseness using formal diagnostic criteria such as the DSM or ICD. While the 18% prevalence rate for GHQ does not directly indicate that these men are suffering from a categorical psychiatric diagnosis, it does highlight that there is considerable stress associated with the transition to fatherhood. This distress was not trivial because they also reported considerable symptoms as measured by the other scales we used. They scored significantly higher than non-distressed men on all symptom-rating scales, suggesting that they both experienced anxiety (including irritability) and depressive symptoms. Their distress had an impact on their quality of life, with the distressed men reporting a poorer quality of life than those men who were not distressed; this was reflected in all facets of the WHOQOL measure, suggesting that there was some global impairment for them during this stressful period. The distressed men tended to consume more alcohol, as measured by the CAGE and the AUDIT; it is not clear whether this was a consequence of discovering their partner was pregnant or whether they became distressed as a result of their alcohol consumption. The important issue here is the impact that such drinking could have upon their partners when it is known that men who are drinking in excess during pregnancy may continue afterwards. A study exploring drinking patterns in couples during pregnancy [22] found that the proportion of men drinking at a high risk level remained static before and during pregnancy, but that the number of men increasing their drinking to low risk levels increased during pregnancy from 10% to 20%.
There has been considerable emphasis on the stress associated with childbirth and the impact that it has on women; there has been less emphasis on the impact upon men of discovering that they are about to become a father for the first time. In a psychological sense, first pregnancy provides a 9 month period for both expectant parents to prepare for the transition to parenthood. This involves grappling with a number of psychological tasks, particularly for expectant new fathers, and we would argue that the distressed group (cases) may be struggling with one or more of these tasks.
First, there is the transition from a dyadic to a triadic relationship, and the need to share their partner's affection with a third party. They will also be expected to care for their infant, a role for which they often have little preparation. Men who feel threatened by this are likely to have a less secure relationship with their partner and have poorer social support systems outside that relationship, as we found with the cases in the present study. It is not clear whether the distress is a consequence of a poor quality of the intimate relationship that is stretched further by the pregnancy or whether the distress of finding out that their partner is pregnant leads to a worsening of the relationship. The crucial importance of this finding is that it has been demonstrated in previous studies that marital or intimate dysfunction during the course of pregnancy is a major risk factor for women subsequently developing postnatal depression [23].
Second are changes that will happen to their self-concept, and the need to prepare for the relinquishment of a more carefree independent lifestyle and the adoption of the responsibilities and restrictions of the parent role, preparations that would involve some degree of grieving. They will have to take on additional responsibilities, not only in providing financially for their new family but also in providing emotional and practical support to their partners. Men with higher levels of neuroticism and who use more immature defence mechanisms would be less likely to cope with these changes and thus would experience distress.
Third, men also often adopt the traditional role of “protector”, and feel more comfortable when in control of situations and able to nurture their partners. During pregnancy the woman comes under the protection of midwives and obstetricians in a world where the father has little influence and very little control. She will often turn to her women friends for support, thus the man loses some friendship and intimacy. He will have lost much of his main source of social support. This will also be the case for men who have poor social networks to turn to for support at this life stage. If the pregnancy was unplanned, men might feel unready and experience anxiety, as might men who have heard about negative parenting experiences from other men. The present findings highlight these characteristics of the distressed group.
The fourth task is to grapple with the concept of “father” and what kind of father the man wishes to be. Men who lack an ego-syntonic model derived from the parenting they received from their own fathers may struggle to develop a model of fatherhood de novo. Men often have not had experience in looking after infants and consequently they experience anticipatory anxiety about how they will cope in a role for which they have not been adequately prepared; or they have not experienced optimal fathering themselves as shown by the cases group, who reported low care and overprotection from their own fathers.
Finally, any of the psychological tasks involved in a life transition can be potentially disrupted by adverse life events, depression or excessive anxiety.
Correlates of distress
We measured key psychosocial variables that could represent vulnerability for distress. The distressed men in the present study were more neurotic, used more immature defences and to some extent reported lower care, particularly from their fathers in the first 16 years of their life. The quality of their intimate relationships was poorer than that in non-distressed men and they reported sparser and few adequate social networks. This is in accord with other studies on the transition to parenthood [22] as well as being consistent with studies on the psychosocial correlates of common psychiatric problems. In general, personality dysfunction, poor social support and early adversity have all been identified as risk factors for the onset of such disorders when confronted with adversity [24]. Based on these data we would argue that we have identified a general vulnerability for distress among the case group. These men, when they discover that their partners are pregnant, perceive it as an adverse event, and thus experience considerable distress as a result. When the putative risk factors in the present study were entered into a regression model, the significant predictors in the final model were neuroticism, perceived inadequate social support and an excess of adverse life events. This is consistent with other studies that have identified these as key risk factors for the onset of non-psychotic distress [25].
Some limitations of the present study should be commented on. First, we acknowledge that the sample that we have collected is not truly representative and there may have been a self-selection because the men were recruited through their partners. Men who were more likely to be vulnerable may not have agreed to participate in the study. Second, we have relied on questionnaire data for the study rather than extensive interviews to identify the men's experiences; this was a pragmatic decision because it would have been very costly and difficult to carry out extensive qualitative interviews in addition to collecting quantitative data about experiences. Although we had some concerns about the reliability of the responses from the men, the internal consistency of responses and the interrelationship between the instruments suggested that the responses were reliable. Finally, we have relied on the GHQ scores to identify cases rather than using categorical diagnoses. Although this may be seen as a major limitation, we would argue that it is more important to identify the level of distress the men experience, rather than rely on categorical diagnoses.
What this study has highlighted is the amount of distress experienced by men during their partners’ pregnancy. Our baseline data were collected early in the third trimester, thus any initial transient reactions (e.g. surprise) would have been long gone, and the reported distress would be accompanying the actual experience of having a visibly (and emotionally) pregnant partner. Attention should be paid to the men who are experiencing such distress, by acknowledging their feelings and helping them overcome their discomfort. This process may be assisted by the provision of information, explanations of what will happen to the partner during the pregnancy and childbirth, suggestions about how they can be of tangible and beneficial assistance to her and, most importantly, by allowing them to discuss their feelings about becoming a new father.
Men experiencing the unanticipated pregnancy of a partner seem to have suffered a greater adjustment reaction. It may also be that men who are planning a family with their partner explore in advance what the experience may entail, for example through discussing with other fathers, attending antenatal classes or reading. This may lead them to feel less anxious about the prospect of becoming a father. They may develop some strategies to involve themselves and thus feel more in control and able to see the positive side of their new situation. Expectations may become clearer and their identity as a new father may become more acceptable to them.
Thus, the results highlight a number of risk factors that may characterize the subgroup of men who are most likely to become distressed or be prone to psychiatric disorder during a first pregnancy. It is likely that many of this group are experiencing difficulty with the psychological tasks confronting them at this life stage. Greater awareness of such risk factors by health professionals may assist them in identifying and supporting men at risk, and assisting them through the adjustments involved. Pregnancy may be a window of opportunity to better prepare more vulnerable men for the arrival of their child, with subsequent long-term benefit for the man himself, his partner and the child.
Footnotes
Acknowledgements
This study was completed with the assistance of funding from the National Health and Medical Research Council of Australia.