
Abstract
Living with a person who has a mental illness can place great strain on family members. The aetiology of psychological disorders can be difficult for informal carers to understand, and providing the right assistance can seem a daunting task [1]. Those who care for a person with a mental illness can themselves experience adverse health outcomes and reduced social functioning [2, 3]. Spouses of people with chronic depression report considerable psychological distress [4–8], physical health problems [5], reduced family support [5], reduced social and leisure activities [9] and strained marital relations [6, 9].
Living with a spouse who has depression in the postnatal period may be even more taxing. Having a baby is a highly challenging life event that requires adaptation from all family members, but particularly from parents [10]. Many of the burdens experienced by informal carers, such as marital strain, are common in the postnatal period [11]. For men, this may be compounded by other stressors unique to this time, such as the absence of appropriate paternal role models in an era when men are expected to be more involved and emotionally responsive parents than previous generations [12]. The stressors associated with having a baby may lead to emotional disturbances, with recent community studies finding that between 2% and 5% of men experience depression at this time [12–15]. However, emotional disturbances in the postnatal period are more common among women, particularly post-partum depression (PPD) which is highly disabling [16] and affects between 8% and 13% of New Zealand women in the first postnatal year [17, 18]. This means that approximately one in 10 men experience the dual stressor of caring for a new baby
As in other contexts, those who have a partner with mental illness in the postnatal period are at increased risk of experiencing psychological distress themselves. Two studies [19, 20] found that 42% of male spouses of women in hospital with a severe post-partum psychological disorder had a psychological disorder themselves, compared with 4% in a community sample of men in the postnatal period [20] and none of the men with partners who did not have a post-partum mental illness [19]. In a further study, men with partners admitted to hospital with PPD had more symptoms of psychological distress than men with partners who did not have PPD or non-specific psychological problems [21]. Although these studies used small samples (n ≤ 40) and did not control for potential confounding variables known to be associated with poor mental health, such as socioeconomic status [22, 23], with such large between-group discrepancies in the men's psychological health status it is likely that these are clinically meaningful results.
Most people who experience mental illness are at the less severe end in the spectrum of severity, and live in the community without receiving professional assistance [23, 24]. Sampling from the community, Zelkowtiz
This study aims to extend previous research by investigating the psychological health of men with partners who have a range of PPD severity (mild to severe) and comparing this to a group of men with partners who do not have PPD (ranging from no symptoms to subthreshold depression). It will explore a broader range of psychological health problems, those that are more common to men at other times, such as alcohol use [27, 28] and aggression [29], in addition to non-specific psychological impairment. These problems affect functioning and increase the risk of developing a specific psychological disorder [30]. The measurement of a range of psychological problems will also allow an investigation of comorbidity which has not been explored between two such groups of men. We hypothesize that men with partners who have PPD will have more symptoms of psychological distress, higher rates of psychological disturbance, and more comorbid psychological disturbances than men with partners who do not have PPD.
Method
The study took place in the greater Wellington region of New Zealand, including the capital city, a provincial town and rural catchments (total population 382 000). In 2001, there were 5984 live births in this region [31].
Participants
One hundred and seventy-four couples participated in this study: 58 men with a partner who had PPD (index group) and 116 with a partner who did not have PPD (comparison group). The sample size was determined using an effect size of 0.56, calculated from Zelkowitz and Milet's study (although this differs from the effect size reported by Zelkowitz and Milet, it was calculated using their published standard deviations and means) [25], and a power of 0.80 [32]. The sample size was adjusted using the Bonferroni method to minimize a Type I error when implementing multiple comparisons [33]. A 2:1 group size ratio was used because comparison group participants were more accessible than index group participants [34].
The inclusion criteria were that couples were in a heterosexual relationship and their infant was less than 13 months old. Participants also had to have a sufficient level of English comprehension to understand and complete self-report questionnaires.
Recruitment
Recruitment took place between March 2002 and September 2003. All comparison group participants and most of the index group (79.3%) were recruited from the Royal New Zealand Plunket Society (‘Plunket’). This organization is primarily responsible for providing health and developmental assessments of infants, and information and support to parents. More than 90% of parents with a New Zealand-born infant access Plunket services. Index group participants were also recruited from a specialist maternal mental health service (10.3%), those involved in a research project exploring PPD in women (5.2%), a postnatal and antenatal distress support group (3.4%) and those who responded to a paper on PPD in a women's magazine (1.7%). As most of these sources provide services to women and their infants, the majority of men were recruited through their female partners.
The process of recruitment involved three stages: initial contact, a telephone assessment and questionnaire completion. Health professionals at the sources of recruitment made the initial contact, inviting all individuals who met the inclusion criteria into the study. It was not possible to get a complete record of the number of refusals at this stage. The principal researcher (S.R.) contacted those who agreed via telephone (n = 853) and administered the Edinburgh Postnatal Depression Scale (EPDS) [35] to screen for depression in women. To maximize detection of depression at this stage of recruitment, all those who scored above 10 on the EPDS and their male partners were invited into the study as
The Wellington and Plunket Ethics Committees approved all procedures used in this study.
Measures
Dependent variables
There were six measures of psychological health. Depression was measured with the Beck Depression Inventory – II (BDI-II), using a threshold score of greater than 13 to indicate depressive disorder [37]. Anxiety was measured with the Beck Anxiety Inventory (BAI), using a threshold score of greater than seven to indicate anxiety disorder [38]. Two measures were used to assess non-specific psychological impairment: the General Health Questionnaire – 28 (GHQ-28), employing the binary scoring system with a threshold score of greater than five to indicate non-specific psychological problems [39]; and the Somatic and Psychological Health Report (SPHERE), utilizing two subscales to indicate problem fatigue (Soma6: six questions about sleeping difficulties and muscular symptoms) and general affective problems (Psych6: six questions relating to symptoms of depression and anxiety) [30]. Alcohol use was measured with the Alcohol Use Disorders Identification Test (AUDIT), using a threshold score of greater than seven to indicate hazardous alcohol use [40]. Symptoms of aggression were measured with the Aggression Questionnaire (AQ) which includes four subscales (anger, hostility, physical aggression and verbal aggression) and a total score (general aggression) [29].
Independent variable
The men's group status was determined by whether their female partner had PPD or not. Male partners of women who scored above 12 on the written version of EPDS [35] were categorized in the index group (n = 36), and partners of women who scored less than 11 on the EPDS were categorized in the comparison group (n = 111). To assess the men's group status of all other participants, their female partners completed a semistructured clinical interview according to DSM-IV criteria for Major Depressive Disorder [41] conducted by an intern clinical psychologist (S.R.). These were couples where the women either scored 11 or 12 on the EPDS (n = 12 index group; n = 4 comparison group), women who had a dramatic change in EPDS score as demonstrated by switching group status between the stages of the telephone assessment and the questionnaire completion (n = 6 index group; n = 1 comparison group), and women who scored less than 11 on the written version of the EPDS yet reported receiving treatment for PPD from a health professional (n = 4 index group).
Most index group women reported current psychological or emotional disturbance (91.4%), of which 63.8% had discussed these difficulties with a health professional, predominantly a general practitioner, and 34.5% were taking prescribed medication. The onset of reported problems was evenly distributed between the period before pregnancy, the antenatal period and the postnatal period (33.3% each). The mean EPDS score of index group women was 14.2 (SD = 3.8; range 5–21). The mean EPDS score of comparison group women was 4.8 (SD = 3.1; range 0–13).
Sociodemographic variables
Several sociodemographic characteristics were collated as potential control variables. Poor psychological health in postnatal men has been associated with indicators of low socioeconomic status [15, 20], age [15], the duration of the couple relationship [42] and the time postpartum (i.e. the infant's age) [13, 43]. The total number of children was hypothesized as influencing the challenges associated with parenting and its potential psychological impact.
Analysis
Parametric tests were used whenever the data met parametric assumptions; log transformations were used if required. Correlations between sociodemographic data (i.e. control variables) and psychological health data (i.e. dependent variables) were explored using Pearson's correlation coefficient for parametric data and Spearman's Rank correlation coefficient for non-parametric data. Those sociodemographic variables found to be significant were adjusted for in the comparison of psychological health scores between the two groups using analysis of covariance. For data that did not meet the parametric assumptions, the analysis was made on the ranked data [44]. Odds ratios between the two groups of men reaching threshold scores indicating psychological disturbance (i.e. nominal data) were compared using logistic regression, adjusting for significant sociodemographic variables.
Results
Sample
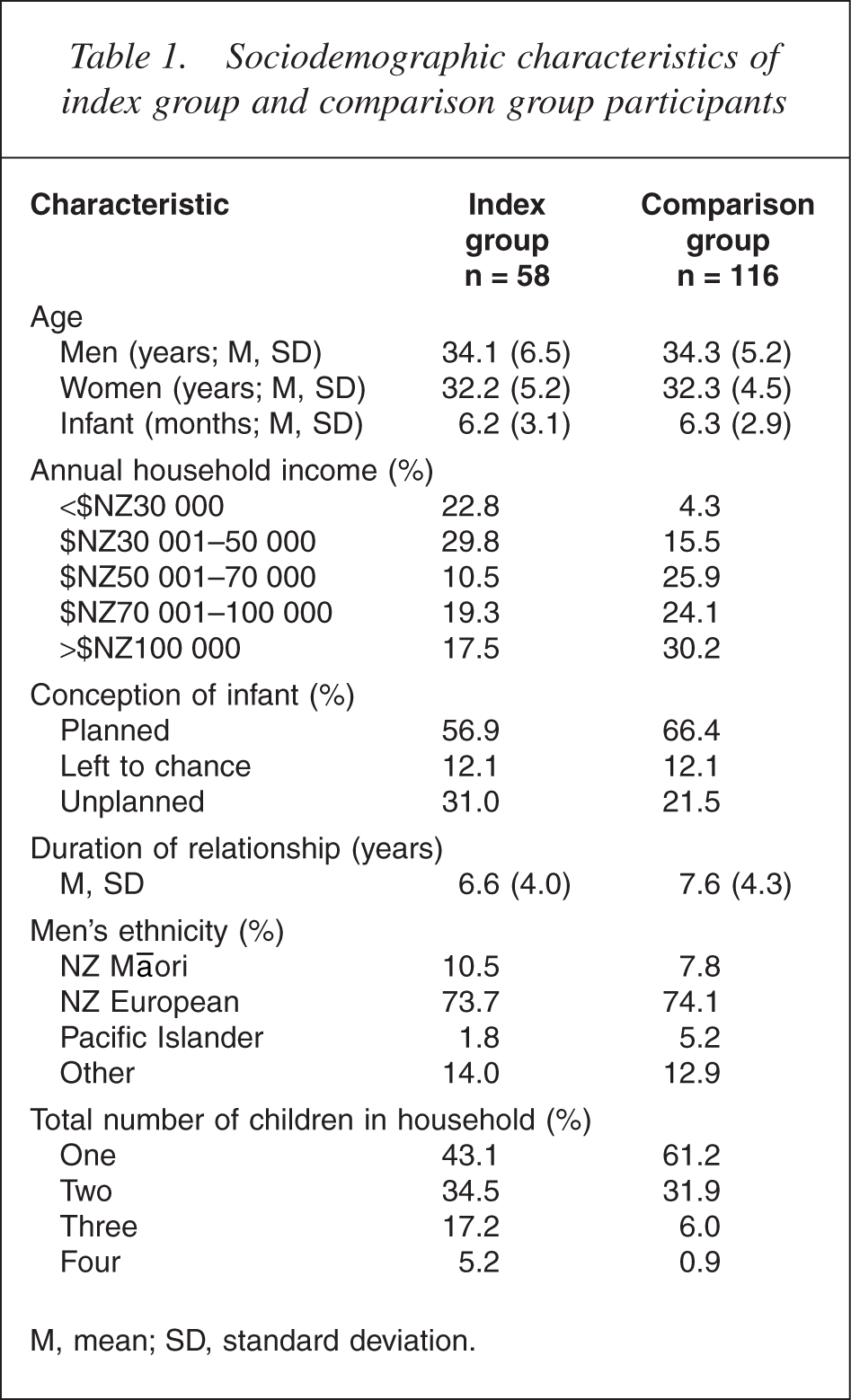
The sociodemographic characteristics of participants are shown in Table 1.
Sociodemographic characteristics of index group and comparison group participants
Psychological symptoms
After adjusting for sociodemographic variables, men who had partners with PPD had more symptoms of depression (BDI-II), non nonspecific psychological impairment (GHQ-28, SPHERE) and general aggression (AQ) than men with partners who did not have PPD (Table 2). Analysis of subscale scores on the AQ showed that index group men had more symptoms of physical aggression than comparison group men (t = − 2.54, df = 7, 165, p = 0.012), and that there was a trend for index group men to report more anger (t = − 1.95, df = 9, 163, p = 0.052). There was no difference between the two groups regarding hostility (t = − 1.07, df = 6, 166, p = 0.29) and verbal aggression (t = − 1.18, df = 8, 164, p = 0.24), and there was no difference for symptoms of alcohol use (AUDIT) and anxiety (BAI) as well.
Between-group comparison of men's symptom scores on psychological health measures
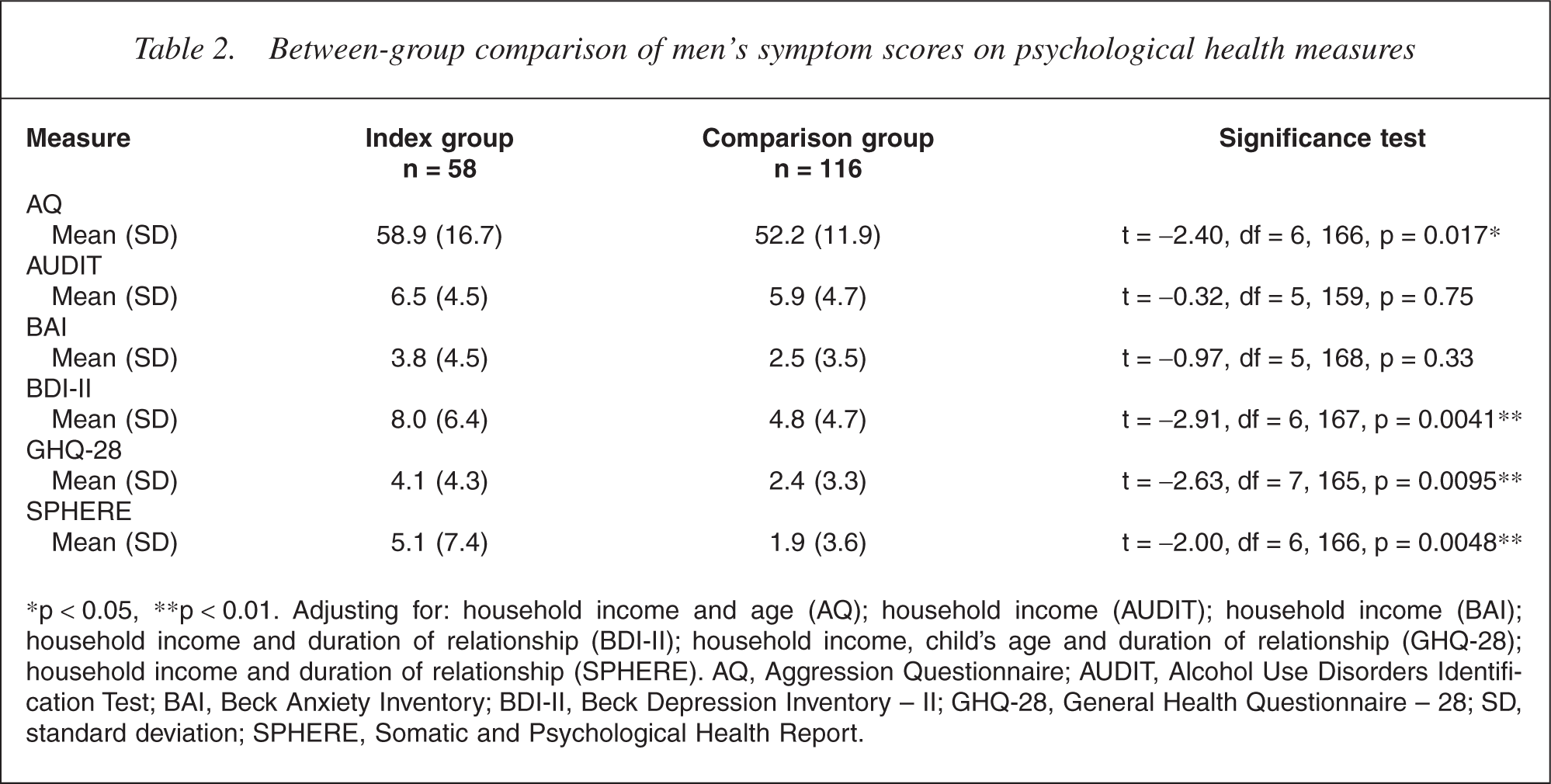
∗p < 0.05, ∗∗p < 0.01. Adjusting for: household income and age (AQ); household income (AUDIT); household income (BAI); household income and duration of relationship (BDI-II); household income, child's age and duration of relationship (GHQ-28); household income and duration of relationship (SPHERE). AQ, Aggression Questionnaire; AUDIT, Alcohol Use Disorders Identification Test; BAI, Beck Anxiety Inventory; BDI-II, Beck Depression Inventory – II; GHQ-28, General Health Questionnaire – 28; SD, standard deviation; SPHERE, Somatic and Psychological Health Report.
Psychological disturbance
After adjusting for sociodemographic variables, more index group men had non-specific psychological problems (GHQ-28), problem fatigue (Soma6, SPHERE) and depressive disorder (BDI-II) than comparison group men (Table 3). There was no difference between the groups for hazardous alcohol use (AUDIT), anxiety disorder (BAI), general affective problems (Psych6, SPHERE), comorbid problem fatigue and general affective problems (Psych6 and Soma6, SPHERE).
Between-group comparison of men reaching thresholds indicative of psychological disturbance
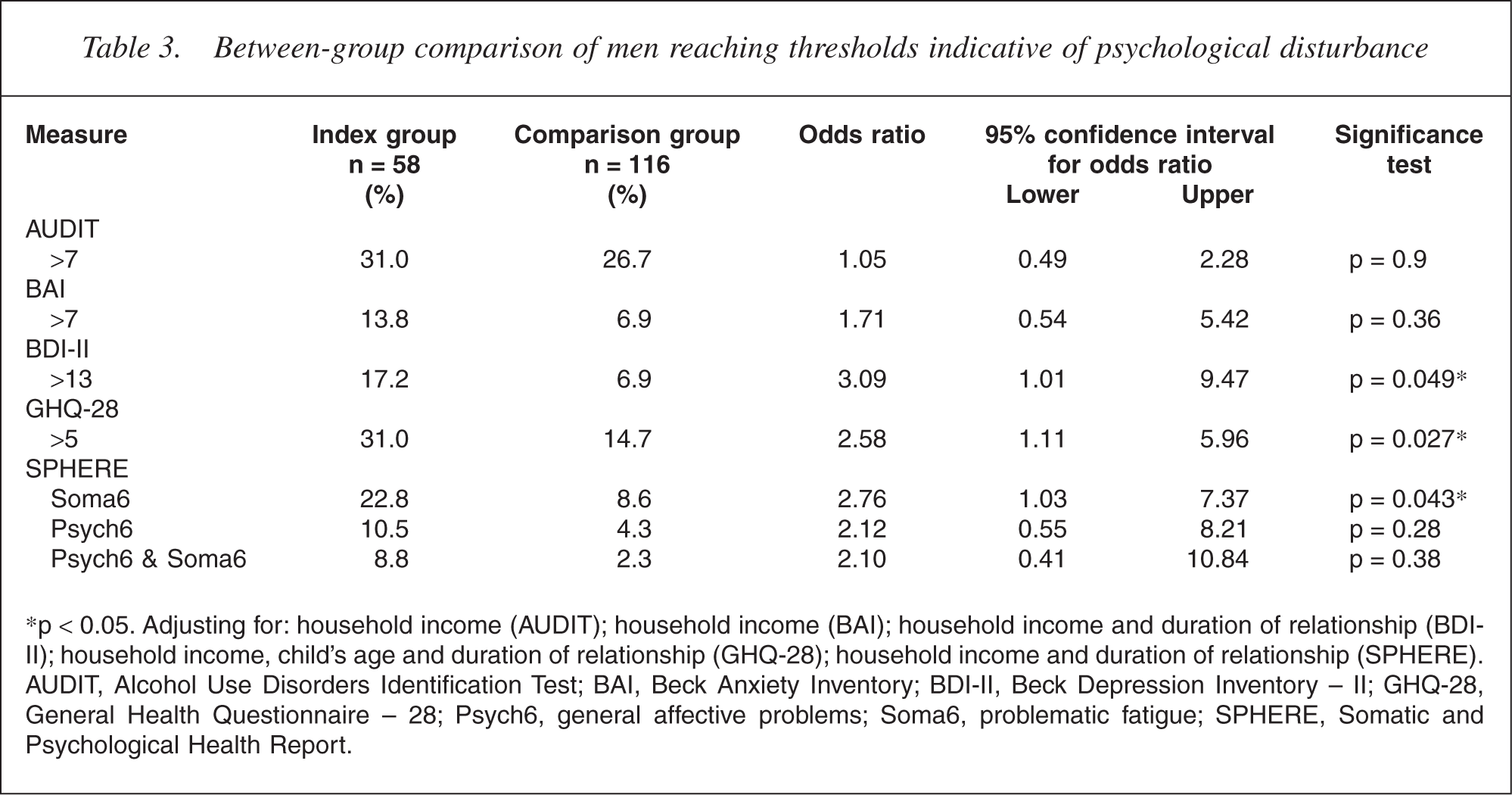
∗p < 0.05. Adjusting for: household income (AUDIT); household income (BAI); household income and duration of relationship (BDIII); household income, child's age and duration of relationship (GHQ-28); household income and duration of relationship (SPHERE). AUDIT, Alcohol Use Disorders Identification Test; BAI, Beck Anxiety Inventory; BDI-II, Beck Depression Inventory – II; GHQ-28, General Health Questionnaire – 28; Psych6, general affective problems; Soma6, problematic fatigue; SPHERE, Somatic and Psychological Health Report.
Multiple psychological disturbances
After adjusting for sociodemographic variables, a trend was revealed in which more index group men than comparison group men reported psychological disturbances in two or more areas. This reached significance for three or more disturbances; the odds of index group men having psychological disturbances in three or more areas were 4.21 times greater than comparison group men (Table 4).
Between-group comparison of multiple psychological disturbances†
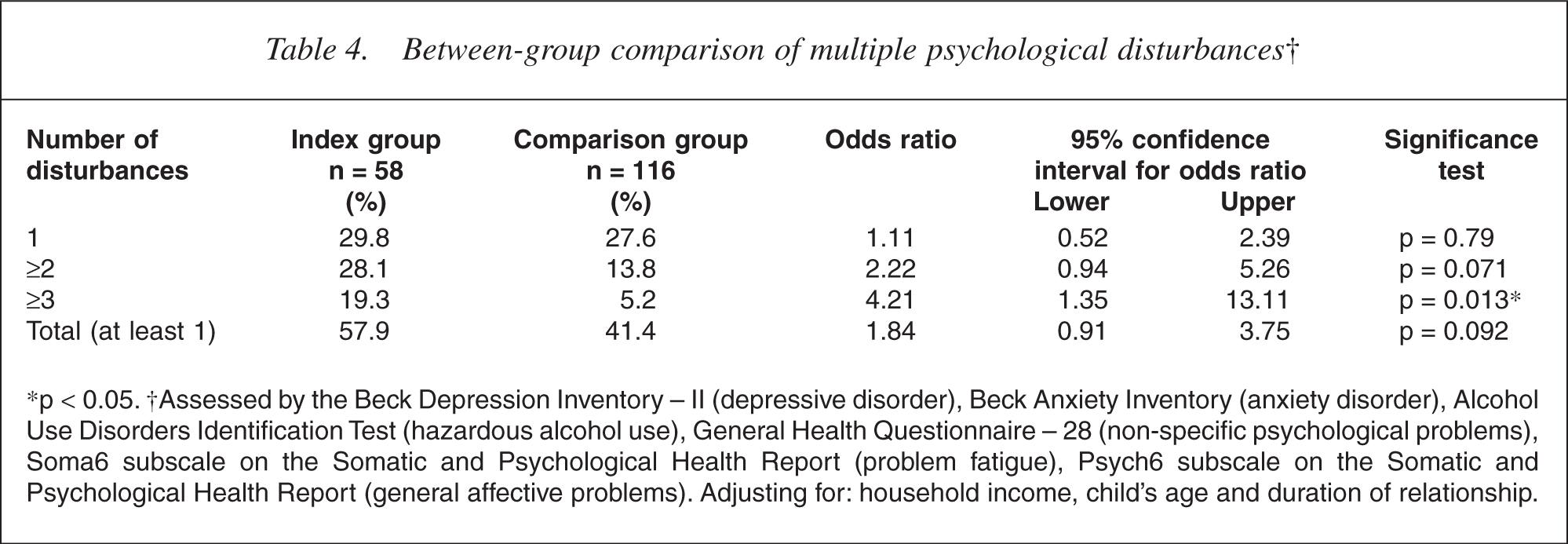
∗p < 0.05. †Assessed by the Beck Depression Inventory – II (depressive disorder), Beck Anxiety Inventory (anxiety disorder), Alcohol Use Disorders Identification Test (hazardous alcohol use), General Health Questionnaire – 28 (non-specific psychological problems), Soma6 subscale on the Somatic and Psychological Health Report (problem fatigue), Psych6 subscale on the Somatic and Psychological Health Report (general affective problems). Adjusting for: household income, child's age and duration of relationship.
Discussion
The principal finding was that men with partners who had PPD reported poorer psychological health than men with partners who did not have PPD. Index group men had more psychological symptoms and disturbances than comparison group men on measures of depression, nonspecific psychological impairment and aggression. Index group men were also more likely than comparison group men to have widespread distress with psychological disturbances in three or more areas.
To our knowledge, this is the first study to report paternal mental health discrepancies between groups that are reasonably representative of postnatal men in the community. A variety of psychological health problems were explored in a sample of men with partners who had a range of depression severity, particularly the more common presentations of mild to moderate PPD, and in a sample of men with partners who were not depressed, or whose depression was subthreshold in terms of severity.
This study mainly relied on a screening tool to classify women's depression and thus allocate group status for the majority of men. To minimize misclassifications, women considered at risk of wrongful categorization underwent a semistructured clinical interview to clarify their depression status. Considering a high proportion of women interviewed were diagnosed with PPD (64.7%), the validity of these interviews is questionable. The use of a validated structured interview to diagnose women's depression would have strengthened the design by providing uniformity of assessment. However, this does not reduce the significance of the findings considering the probable direction of this potential bias, that is some female partners of men classified in the index group may not have had PPD. Although some discrepancies in the mental health of men in the two groups were just within the 5% level of significance, a consistent pattern of poorer health for men with depressed partners was evident and suggests that these appear to be clinically meaningful results. Finally, although the cross-sectional design does not allow investigation of the direction of effect, we consider that the findings are consistent with caregiver burden theory [2, 3] and previous research [19–21, 25, 26]. The most appropriate interpretation is that men with partners who have a post-partum mental illness are at increased risk for having poor psychological health themselves.
A key new finding of this study is that consideration of the specific types of psychological problems is important; men with partners who have PPD are particularly at increased risk for certain types of psychological syndromes. For example, rates of anxiety disorder did not differ significantly between the two groups. Although previous post-partum studies reported cases of anxiety in male partners [20, 26], these studies did not analyse between-group differences of psychological syndromes separately. Further, non-specific psychological impairment (GHQ) was significantly different between the groups and in the expected direction; yet there was no difference in the prevalence of men with general affective problems (Psych6, SPHERE). The SPHERE subscale explores symptoms specific to depression and anxiety, suggesting that a between-group difference was only found using a measure of pervasive psychological distress.
Although all parents are susceptible to fatigue in the postnatal period because of changes in routines, particularly sleeping patterns, an interesting new finding of this study is that men are more affected by severe fatigue if they have a depressed partner. Fatigue is often symptomatic of other psychological disturbances such as depression, but it has also been found to have an independent effect on functioning and wellbeing [45]. Hagen [46] found that the severity of depression in one spouse was associated with increased childcare in the partner, suggesting that more index group men may be fatigued than comparison group men because they experience more burdens, such as providing additional childcare.
Although there are high rates of comorbidity in general populations, particularly combinations of depression, anxiety and alcohol abuse disorders [23, 24, 27, 28], with the exception of Matthey
There have been appeals for men to be more supportive and involved parents, particularly when their partners have PPD [49]. However, the results of this study suggest that a clinically important proportion of these men may not be able to adequately support their partner because they are not well themselves. With current perinatal health care overwhelmingly focused on women or the mother–infant relationship [50], this study highlights the need for fathers' mental health to be considered by health professionals. Indeed, as men are generally more reluctant than women to seek professional assistance for psychological difficulties [24], routinely assessing men's mental health in the postnatal period would lead to the identification of problems that otherwise go undetected. From a family systems perspective, appropriate interventions for men may result in benefits for both men and their female partners because ‘healthy’ men may provide better care and support, a factor known to protect women from PPD [51]. Further, as maternal PPD is associated with a variety of adverse child outcomes (for a review see Murray and Cooper [52]), this would therefore also be crucially beneficial to the developing infant, particularly as negative child effects may be moderated by the availability of a psychologically healthy father [53, 54].
As the psychological health of men in the postnatal period may influence the health and wellbeing of all members of the family, clinical trials exploring both the short- and long-term effectiveness of different interventions for distressed men and their families are required. Brief interpersonal therapies for maternal PPD have been found to be beneficial for both women [55–57] and their infants [58], but only at the time of administration [55, 58]. Considering the level of couple morbidity evident in this study, perhaps one of the factors hindering sustained benefits of psychotherapies is that many women are living with a partner who has undetected and untreated post-partum psychological distress. Finally, longitudinal studies are required to explore aetiological mechanisms of men's poor psychological health, including an investigation of the relationship between maternal and paternal psychological distress.
Footnotes
Acknowledgements
The study was supported by a research grant from the Wellington Medical Research Foundation. Thanks to those who assisted with recruitment and all who took part in the study.