
Abstract
Background:
With a healthcare system burdened by symptomatic and mental-health related conditions, the placebo effect may represent a useful clinical tool. First, however, there is a need to broaden research attention and investigate placebo effects outside laboratories and beyond experimental pain. This study investigated the effectiveness of a take-home placebo treatment in the short-term alleviation of stress, anxiety and symptoms of depression in a non-patient population.
Method:
A sample of 77 participants was randomized to either the ‘oxytocin’ treatment group (n = 22), the ‘serotonin’ treatment group (n = 22) or the wait-list control group (n = 33). The two treatment groups were given an ‘anti-stress treatment spray’ (placebo) to self-administer for 3 days, and completed online measures of perceived stress (Perceived Stress Scale-10), anxiety (Cognitive Somatic Anxiety Questionnaire) and symptoms of depression (Centre for Epidemiological Studies – Depression) before and after the 3-day protocol.
Results:
Both the ‘serotonin’ and ‘oxytocin’ treatment sprays were effective in reducing symptoms of depression; however, only those in the ‘oxytocin’ group reported less stress and anxiety as compared with controls. Overall, the ‘oxytocin’ was perceived as more effective.
Conclusion:
Placebo effects can be translated to a real-life setting in the short-term reduction of stress, anxiety and symptoms of depression in a non-patient population. In treating psychological distress, placebos may be useful addition to the treatment repertoire. The information given with treatment may also be an important consideration for practitioners.
Introduction
Psychiatric and psychologically influenced conditions represent a significant healthcare burden (Barsky et al., 2005; Milczarek et al., 2009; Nimnuan et al., 2001; World Health Organization, 2001). Treating ailments such as stress, anxiety and depression can be difficult, not only because they are pervasive and debilitating (Ferrari et al., 2013; Santini et al., 2015), but because standard-care pharmacological approaches may not always be optimal or effective. For example, in some cases, antidepressants may not deliver benefits over no-treatment in the long term (Hughes and Cohen, 2009), and there can be negative effects associated with long-term medication use (Cascade et al., 2009; Hu et al., 2004).
The placebo phenomenon has shown that the act of administering treatment, regardless of its properties, can deliver health benefits (Benedetti, 2002, 2013). An individual’s expectations, the therapeutic ritual and the psychosocial context of treatment (Colloca and Miller, 2011b; Kaptchuk, 2011; Miller and Kaptchuk, 2008) can generate positive changes in the absence of pharmacological agents. Thus, placebos could be a clinically useful tool; however, before the power of the placebo can be harnessed in mental-health contexts, further research is needed.
One issue to be overcome is that placebo effects are not often directly investigated in depressed and anxious patients because of the ethical issues inherent to deceiving vulnerable populations (Benedetti, 2009). Despite this challenge, research shows that in the treatment of depression, placebos used adjunctively with supportive care sessions can be just as effective as ‘active’ medications (Leuchter et al., 2014); and meta-analyses of clinical depression trials report limited benefits of antidepressants over placebos for people who are mildly to moderately depressed (Kirsch, 2010; Rief et al., 2009). Furthermore, placebo responses in clinical trials for anxiety disorders can be up to 60%, with long lasting and clinically relevant effects observed in some trials (Schedlowski et al., 2015).
However, the absence of direct placebo investigations in this area means one cannot be sure of the efficacy of stand-alone placebo treatments. Changes in depressive symptoms occur naturally, meaning the use of a no-treatment (or wait-list) control group is a vital component of determining a treatment’s efficacy (Rief et al., 2011). That is, like drug trials that use placebo control arms to determine the relative efficacy of a pharmacological agent, the efficacy of a placebo treatment also needs to be specifically tested, ideally against a ‘no-treatment’ control.
Another issue hindering the translation of the placebo effect for clinical utility is the predominance of research carried out in laboratories. Such research offers experimental control and the ability to implement rigorous protocols, but represents a relatively artificial environment. Placebos have been shown to reduce acute stress and anxiety in lab settings (Colloca et al., 2004; Darragh et al., 2014; Petrovic et al., 2005); however, in the real-world, depressed, stressed or anxious patients are required to self-administer treatments around their daily activities and amidst the natural fluctuations in the demands and challenges of life. As a consequence, effects seen in laboratory-based placebo experiments when acute noxious stimuli are induced and then alleviated with placebo treatments may not extend to real-life settings.
There have been relatively few studies investigating the effectiveness of placebo treatments when they are ‘prescribed’ and taken home for use over several days. One study using such a protocol demonstrated clinically significant improvements in irritable bowel syndrome (Kaptchuk et al., 2010); however, it is not known whether this finding is translatable to mental-health conditions. Thus, in order to expand knowledge in this area without jeopardizing the wellbeing of a vulnerable patient sample, this study aimed to investigate the effectiveness of a take-home placebo treatment for the short-term alleviation of stress, anxiety and symptoms of depression in a physically healthy, non-patient population.
Method
Design, randomization and blinding
This was a randomized, controlled, non-laboratory study. All participants were randomized into one of three groups: a wait-list control group or one of two ‘treatment’ groups. Randomization to group was conducted by the lead researcher immediately prior to the participant’s appointment with the research assistant (RA). The two treatment groups received ‘anti-stress’ intranasal treatment sprays to self-administer for 3 days. Both treatment sprays were placebos and contained only sterile saline (5%), but were described as two different ‘compounds’: one which stimulated the body to produce oxytocin and the other to produce serotonin (see Procedures). Two different treatments were offered as part of a larger research study investigating personality predictors of responding to treatment descriptions.
The RA who met with participants was not blind to group; however, all baseline and outcome measures were completed by participants via an online survey (i.e. not in the presence of the RA).
Participants
To recruit a sample with sub-clinical levels of psychological distress (stress, anxiety and depressive symptoms), advertisements requesting healthy volunteers experiencing mild to moderate daily stress were placed around a hospital research department and on a university intranet. Of 238 who expressed interest, 109 (46%) returned the screening questionnaire. Of these, 93 met inclusion criteria of being 18–65 years of age, no diagnosed psychological conditions in the past 5 years, no medications (except those for acne and birth control) and no chronic illness (diabetes, multiple sclerosis, cancer, rheumatoid arthritis, fibromyalgia, chronic fatigue syndrome, organ transplant, lupus, auto-immune or respiratory conditions). Of the 93 eligible participants, 90 completed the first questionnaire assessing demographics and personality. Of these 90, six could not be contacted to schedule an appointment, one did not appear for their appointment and two withdrew from the study. Of the 81 that initiated the treatment protocol, two did not complete the daily measures and two withdrew because of adverse reactions attributed to the intranasal spray. The final sample size was 77, with 33 participants in wait-list control, 22 in the ‘serotonin’ group and 22 in the ‘oxytocin’ group.
The university’s review board (The University of Auckland’s Human Participants Ethics Committee) approved the study (UAHPEC ref: 010757) and participants provided written consent after reading a detailed description of the study and the procedures involved. All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Procedure
After completing screening, consent and an online personality survey (reported elsewhere), participants were scheduled for one 15-minute session with the RA. The RA gave a brief overview of the study, explaining how participants would receive an ‘anti-stress’ treatment to reduce the symptoms and experience of stress and anxiety. After the RA checked exclusion criteria, they informed participants to which of the three groups (Treatment S, Treatment O or wait-list control) they had been allocated.
The Treatment S (‘serotonin’) group was told the spray contained a compound designed to increase levels of serotonin in their system and that serotonin helps regulate stress responses by suppressing negative stress hormones and generating positive moods. The Treatment O (‘oxytocin’) group was told their spray contained a compound designed to increase levels of oxytocin in their system, and that oxytocin is a hormone that helps regulate stress responses by promoting social engagement and generating feelings of trust and connectedness. The control group was advised that for 5 days, they would complete the online forms only and then commence the treatment protocol with their choice of either the serotonin or the oxytocin treatment sprays.
This information was re-iterated within a brief (2 minute) video. After the RA demonstrated how to use the intranasal spray and explained how to complete the daily online measures, participants were given their treatment pack. This pack included the appropriate intranasal spray and written instructions that re-iterated all the verbal information provided.
Summary of protocol
After their appointment (Day 1), all participants were sent a link to the first questionnaire, which assessed baseline (pre-treatment) perceived stress, anxiety and depressive symptoms. On Days 2, 3 and 4, they completed a symptom report sheet assessing the experience of general stress-related symptoms. On Day 5, they again completed the measures of stress, anxiety and depressive symptoms (post-treatment measures). Adherence to the regime was assessed by self-report measures during the three treatment days, as well as on the final day.
For each day of the protocol, links to the online forms were emailed with the instructions to complete the forms at the end of the day. Once the 5-day protocol had been completed, the treatment group participants were thanked for their participation. The control group was informed that they could now commence taking the treatment. Upon completion of the protocol, all participants received $20 in vouchers and were entered into a draw to win an I-PAD.
Measures
Prior to the laboratory session, participants completed an online questionnaire assessing general health (doctor visits in the last 12 months, perceived general health, height and weight to calculate body mass index [BMI]), basic demographics (age, sex, ethnicity) and personality traits. The personality data are outside the scope of this paper and will be reported elsewhere.
Stress
The Perceived Stress Scale (PSS) (Cohen et al., 1983) is a 10-item questionnaire designed to measure the extent to which participants perceive their lives to be stressful. Participants are asked to indicate on a 5-point scale how often (‘never’ to ‘very often’) they have thought or felt in certain ways in the last month. Scores were coded so that higher values indicated higher perceived stress. Internal consistency for the PSS was good on Day 1 (α = 0.80) and Day 5 (α = 0.86)
Depressive symptoms
The Centre for Epidemiological Studies Depression Scale (CES-D) (Radloff, 1977) assesses depressive symptoms in the general population. Participants rated how often they experienced symptoms of depression in the last week on a scale from 0 ‘rarely/none of the time’ (<1 day) day to 3 ‘most/all of the time’ (5–7 days). Internal consistency for the CES-D was good on Day 1 (α = 0.89) and on Day 5 (α = 0.90)
Anxiety symptoms
The Cognitive Somatic Anxiety Questionnaire (CSAQ) (Schwartz et al., 1978) assesses both somatic and cognitive aspects of anxiety. Participants rate from 1 (not at all) to 5 (very much so) how much in the last week they had experienced somatic symptoms of anxiety (e.g. ‘I had diarrhoea’ and ‘my heart raced’) as well as anxiety-related thoughts (e.g. ‘I worried too much over something that doesn’t really matter’). Internal consistency for the CSAQ was good on both Days 1 and 5 (αs = 0.85)
Daily stress symptoms
On Days 2, 3 and 4, participants completed a measure of stress symptoms. This 16-item scale was developed for the study and asked how much participants had experienced symptoms of stress during the day, from 0 ‘not at all’ to 7 ‘extremely’. For example, feeling ‘stressed out’, heart pounding or racing, felt sad or down and inability to concentrate. The scale was designed to measure symptoms of stress, depression and anxiety during the 3 days that the other measures were not administered. The internal consistency of the scale was good for all 3 days (Cronbach’s α = 0.90, 0.91 and 0.92).
Dosage and adherence
On Days 2, 3 and 4, those in the treatment groups completed a self-report measure of dosage: ‘how many times did you administer the spray today’ and ‘how many pumps of the spray in total did you administer today’. On Day 5, they completed a measure of overall dosage and adherence: they were asked to rate on a scale from 0 to 6: to what extent did you follow the recommended dose; and how many times did you forget a dose? They were also asked to indicate how many days did you administer the treatment spray (0–3); and on average how many times a day did you administer the treatment spray.
Perceived effectiveness
On the final day of the protocol, participants were asked to rate from 1 (‘not at all’) to 10 (‘very much so’) how much did the anti-stress treatment: reduce stress/reduce feelings of irritability/reduce the impact of life pressures/reduce feelings of tenseness and frustration / reduce symptoms of stress. Using this same scale, participants also rated how much the treatment reduced stress by increasing feelings of social engagement and reduced negative stress-related moods. These two items were consistent with experimental suggestions provided regarding the effects of the oxytocin and serotonin treatments respectively.
Results
Analytic approach
One-way analyses of covariances (ANCOVAs) were conducted to test for baseline between-group differences. Two-tailed tests for significance were set at 0.05 and pairwise comparisons were corrected with Fisher’s least significant difference test LSD. Three one-way ANCOVAs were carried out to compare differences between the treatment vs control groups in their levels of stress, anxiety and symptoms of depression on Day 5, while controlling for Day 1 scores, and age, given the baseline difference between the serotonin and control group in mean age (Table 1). To compare the three groups in terms of changes in symptoms of depression, anxiety and stress pre to post treatment, the mean change score for each outcome variable was calculated (Day 5 minus Day 1 so that a negative value indicates a reduction in symptoms). Stress symptoms during the three treatment days were compared across the three groups by taking an average of reported symptoms. Means and standard errors were used to calculate 95% confidence intervals (CI) [lower limit, upper limit].
Tests for baseline differences between the groups in demographic, health and outcome variables; as well as tests for placebo effects on outcome variables and 95% confidence intervals calculated with mean and standard error.
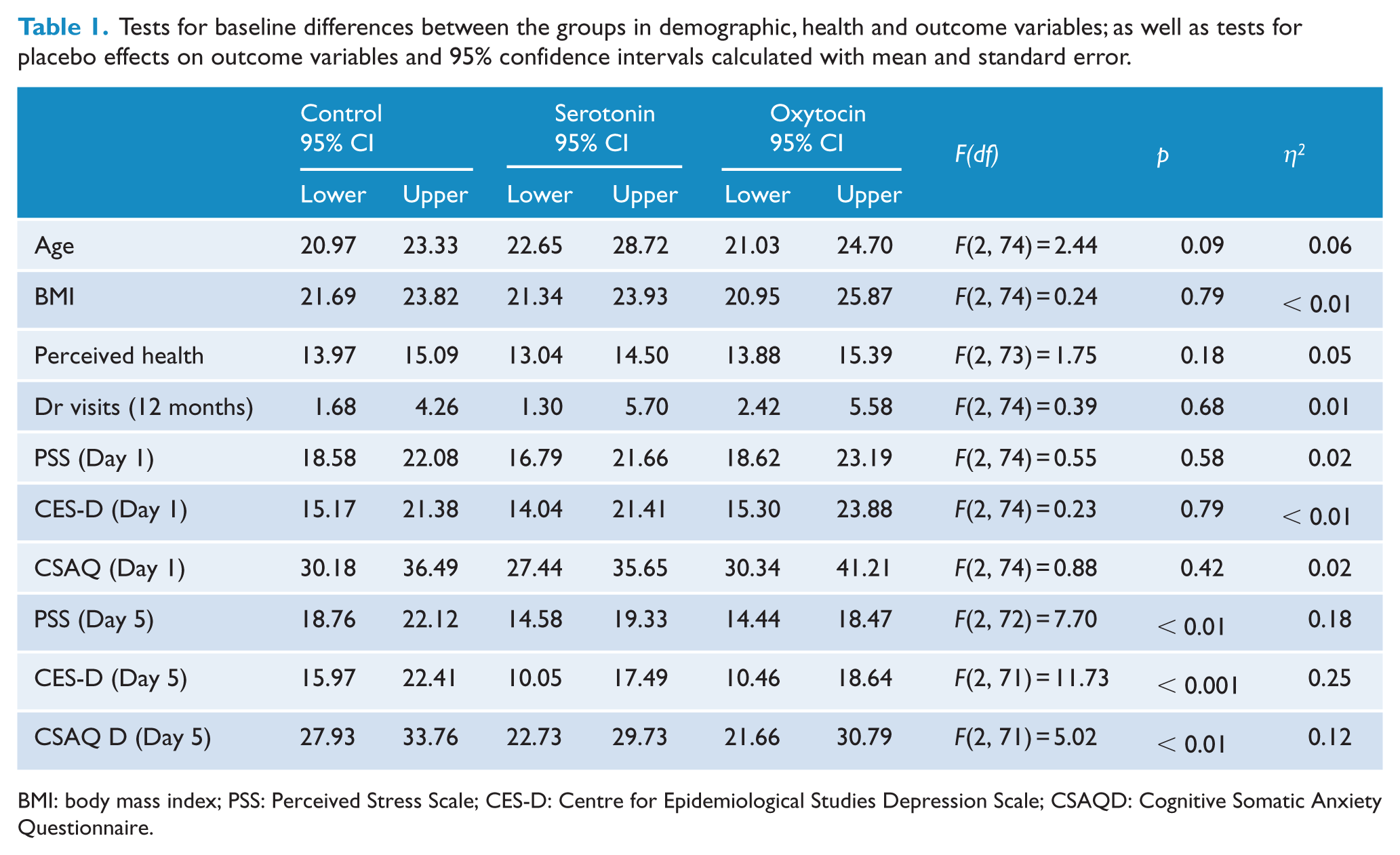
BMI: body mass index; PSS: Perceived Stress Scale; CES-D: Centre for Epidemiological Studies Depression Scale; CSAQD: Cognitive Somatic Anxiety Questionnaire.
Sample characteristics
Participants were aged from 19 to 50 years of age (mean [M] = 24 years, standard deviation [SD] = 5.92 years); predominantly female (70%); with New Zealand (NZ) Europeans making up the largest ethnic group (53%) with Asian (including Indian, Sri Lankan and Pakistani participants) the next largest group (40%) and the remainder describing themselves as ‘other’ (7%). There were no sex or ethnicity differences between the groups (p > 0.05).
Placebo effects
Results revealed a main effect of group for depressive symptoms, anxiety scores and perceived stress (Table 1) with lower scores on Day 5 in the two treatment groups as compared with controls. In comparing change scores, those in the control group had (on average) a slight increase in depressive symptoms over time 95% CI [−0.82, 2.82], whereas both the serotonin group [−5.73, −2.17] and the oxytocin group [−7.27, −2.84] had a decrease. Symptoms of anxiety decreased in the control group 95% CI [−5.53, 0.27], but more so in the oxytocin group [−13.20, −5.90], and marginally so in the serotonin group [−7.30, −3.34]. Similarly, perceived stress decreased in the oxytocin group 95% CI [−6.82, −2.09], as compared to the control group control group [−1.37, 1.68], but the serotonin group’s reduction group [−4.10, −0.44] was only marginally greater than the control groups. differences in average daily stress symptoms during the 3-day protocol (Days 2, 3 and 4), while controlling for age. There was a marginal main effect of group, F(2, 70) = 3.09, p = 0.05. In comparing the three groups, there was no difference between the serotonin group 95% CI [1.87, 2.63], and the oxytocin group [1.88, 2.63], but the control group’s scores were marginally higher [2.47, 3.10] than the two treatment groups.
Treatment adherence and perceived effectiveness
Independent samples t-tests (two-tailed with significance set at 0.05) revealed a difference between the two treatment groups in perceived effectiveness. Those taking ‘oxytocin’ reported it more effective than ‘serotonin’ (Table 2). Further, compared with ‘serotonin’, taking ‘oxytocin’ increased feelings of social engagement (as per the suggestive instruction) whereas ‘serotonin’ failed to significantly reduce negative stress-related moods (as per the suggestive instruction).
Results of independent sample t-tests comparing the serotonin and oxytocin groups in adherence to the regime, as well as the perceived effectiveness of the treatment, with 95% confidence intervals calculated with the mean and standard error.
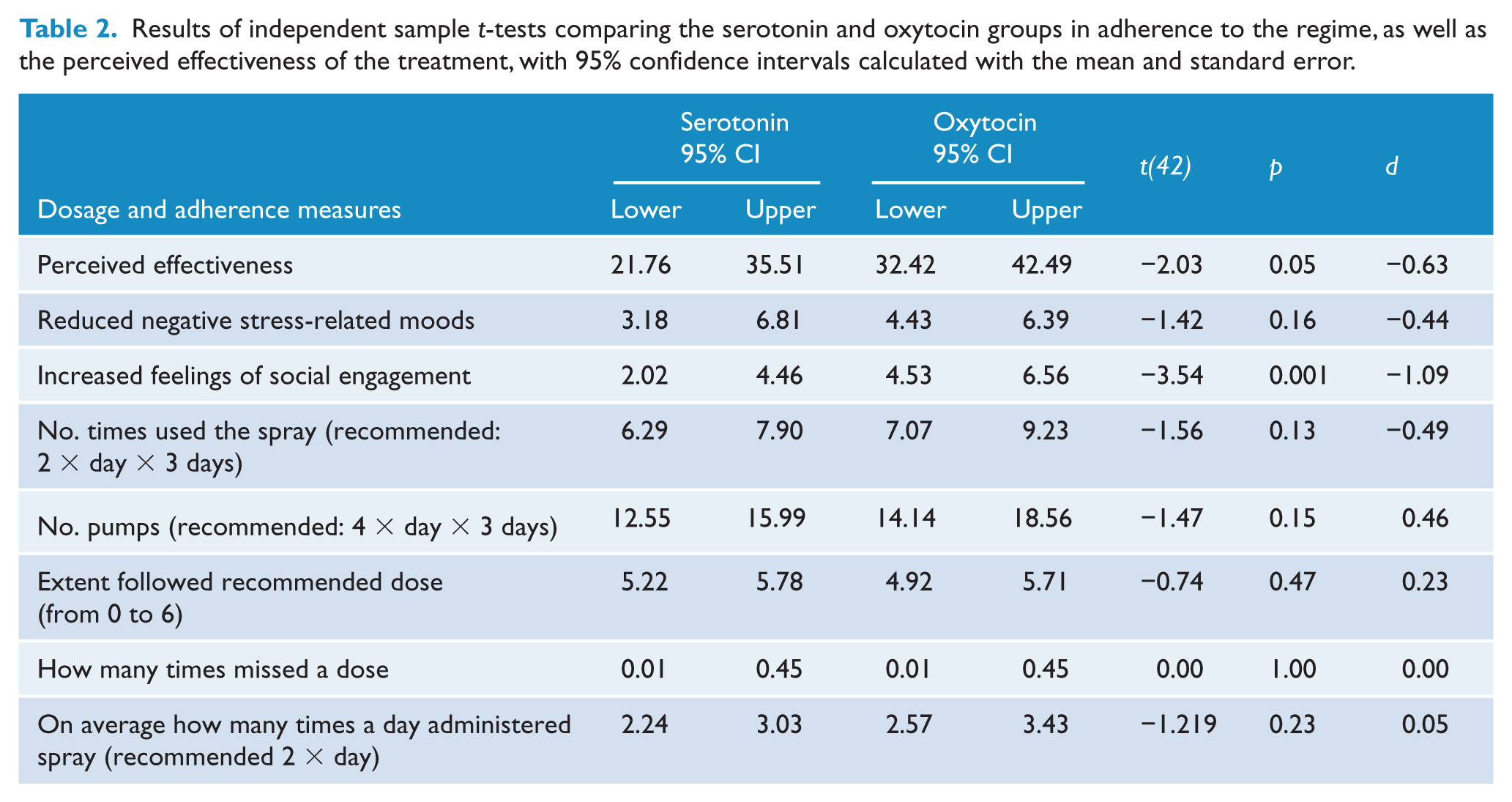
While non-significant, there was an overall trend for the oxytocin group to self-administer a greater number of dosages (Table 2). There were no significant correlations among adherence, dosage and outcomes (ps > 0.05).
The control group was permitted to select their choice of the two treatments to commence upon completion of the wait-list protocol. A significantly greater proportion (χ2 = 8.76, p < 0.01) chose to take ‘serotonin’ (n = 25) than ‘oxytocin’ (n = 8).
Discussion
This study investigated the effectiveness of a take-home placebo treatment in the alleviation of mild to moderate psychological distress. Findings revealed that in a non-patient population, placebos can be effective in a naturalistic setting and that a self-administered placebo treatment can reduce the symptoms of stress, anxiety and depression across a short time frame. Both the serotonin and oxytocin placebo treatment groups had fewer depressive symptoms after the treatment protocol and reported fewer symptoms of stress during the 3 days of use, compared with the control group. However, only the oxytocin group reported less perceived stress and fewer symptoms of anxiety after the treatment, as compared with the control group.
The ‘oxytocin’ was also subjectively rated as more effective overall. Prior work has shown that a patient’s belief in the effectiveness of their treatment is an important part of their actual effectiveness (McRae et al., 2004). At face value however, ‘serotonin’ was a more attractive option, as the preferred treatment choice for the wait-list controls.
A possible explanation for this might be the buffering qualities of perceived social support. Participants in the oxytocin group were told it would stimulate feelings of social engagement and, indeed, this group reported greater feelings of social engagement after the treatment. Perceived social support can ameliorate symptoms of anxiety (Dour et al., 2014) and attenuate the impact of stressors in laboratory contexts (Thorsteinsson and James, 1999). Social support may be a buffer that prevents stress leading to depression (Asberg et al., 2008), and social networks and social connectedness have been repeatedly linked to better outcomes in depression (Santini et al., 2015; Smith and Christakis, 2008). Self-administering ‘oxytocin’ may thus have created a greater subjective experience of being socially engaged or, more speculatively, prompted participants to actually be more socially engaged. Whether from a perceived or actual increase in social engagement, participants appear to have experienced benefits.
This study demonstrated that a placebo treatment can be effective in the short-term alleviation of psychological distress as compared with a natural history (wait-list) control group. This finding may be important in interpreting results from clinical drug trials for depression or anxiety, but also helps overcomes prior criticisms of placebo research. That is, meta-analytic reviews have suggested that at least in some areas, placebo effects are minimal, or can be attributed to natural illness fluctuations or progression (Hrobjartsson and Gotzsche, 2010). While it is possible that the placebo vs control difference was, in part, bolstered by an increase in distress within the control group due to the delay before ‘treatment’, inspection of the raw scores reveals only a small increase in stress and depressive symptoms and a small decrease in symptoms of anxiety.
In considering the clinical applicability of this study, findings are limited by the use of a non-patient sample; however, the baseline depression scores were high, with the average across the whole sample above the standard screening cut-off point of 16 (Radloff, 1977). In specifically recruiting a sample of individuals experiencing life stressors, the observed high baseline scores of depressive symptomology are not surprising. Together, this increases confidence that these findings offer clinical utility, and at least might be applicable to mildly depressed students, who are known to experience higher rates of moderate psychological distress (Cvetkovski et al., 2012).
More broadly, the question of how to transfer placebo effects into clinical contexts represents a substantial ethical and practical hurdle (Colloca and Miller, 2011a; Miller et al., 2005). Findings from this report indicate that placebos can generate short-term improvements in symptoms of distress, which offers another way in which placebo effects might be leveraged. That is, with a delay before most anxiety and depression medications take effect, placebos could be used as an interim treatment so that patients experience some form of immediate relief. Equally, when a drug washout phase is required between medications, a placebo could be used as a stop-gap measure, so that patients do not feel abandoned or despairing while waiting for a new medication to take effect.
Findings also imply that placebos could be useful for assisting with the short-term treatment of sub-clinical levels of stress, depression and anxiety in primary care. In this study, the verbal suggestion focused on the stress-reducing properties of the treatment spray, but it had the effect of reducing overall psychological distress and, in particular, depressive symptoms. There are clear overlaps between perceived (or psychological) stress, anxiety and depression (Asberg et al., 2008), with chronic stress and a dysregulated physiological stress system a factor in the development of depression (Gold, 2015). This finding suggests that for individuals feeling challenged by life stressors, targeting the experience of stress may have the flow-on effect of alleviating depressive symptomology.
One key challenge that remains before placebo treatments can be ethically used in patient samples is the issue of deception (Colloca and Miller, 2011a; Miller et al., 2005). One way to overcome this considerable hurdle is with the use of open-placebo studies, in which the nature of the treatment (a placebo) is explained, but in such a way that there is still an expectation of benefit. For example, a prior study demonstrated clinically significant improvements in IBS symptomology after participants were told they had been given an inert substance, but that the treatment has ‘been shown in rigorous clinical testing to produce significant improvement in IBS symptoms through mind-body self-healing processes’ (Kaptchuk et al., 2010: 2). It seems reasonable to suspect that similar benefits might be obtained for the mental-health outcomes evaluated in this report.
In treating psychological distress in the longer term, the administration of open-placebo treatments could perhaps be integrated into a treatment plan in such a way as to encourage self-directed action by patients. Describing to patients how placebos work, such as stimulating the brain to release neurotransmitters (Pacheco-Lopez et al., 2006) and activating endogenous healing processes (Finniss and Benedetti, 2005), may be a useful way to explain how supposedly ‘inert’ treatments can exert real effects on health outcomes; and could highlight the role a patient plays in improving their condition. Further work using open-placebo designs is needed to explore how physicians and clinicians can ethically and optimally offer placebos to patients as a treatment option.
Limitations to this study include the use of a healthy, mostly young, non-patient population, which limits the generalizability and applicability of findings. Findings are also limited by the short time frame. It is not known whether effects would be the same for a longer treatment period, or how they might be maintained over time. Future research could aim to replicate findings in a patient population and across a longer time period.
Conclusion
Overall, findings suggest that placebo effects can be translated to a real-life setting in the reduction of moderate stress and symptoms of anxiety and depression, at least in the short term. With a healthcare system that is plagued by overtaxed resources and over-medicated individuals, new ways to treat psychological distress while minimizing iatrogenic harm are needed. The placebo effect may represent a health tool that could be harnessed for clinical benefit in mental-health related ailments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.