
Abstract
Growth of the antidepressant market and widespread use of the illicit drug ecstasy (methylenedioxymethamphetamine; MDMA) creates a need to delineate the potential harms associated with the concomitant use of ecstasy and serotonergic pharmaceutical drugs. One such harm is serotonin syndrome. The study aimed to synthesize the risk of serotonin syndrome associated with the concomitant use of ecstasy and other serotonergic substances in a clinically relevant hierarchy for psychiatrists and other medical practitioners. An extensive online database search was carried out of the literature on serotonin syndrome, in relation to illicit drugs and simultaneous use of other substances. Numerous licit and illicit substances implicated in serotonin syndrome, when used with ecstasy, have potential for increased toxicity and are presented in a resulting hierarchy of risk. Substances that inhibit serotonin re-uptake are less likely to lead to life-threatening elevations in serotonin when used with ecstasy. High doses or repeated use of stimulants such as methamphetamine and cocaine with ecstasy increase the risk of serotonin syndrome; as does the use of pharmaceutical amphetamine and ecstasy. Serotonin precursors also influence the course of serotonin syndrome when used with ecstasy. Substances that inhibit monoamine oxidase are most likely to lead to serious increases in serotonin when used with ecstasy. Findings highlight the importance of screening for the use of ecstasy and other serotonergic substances when prescribing antidepressant drugs.
Over the last few decades there has been a remarkable increase in the number of people treated with depression and, in most developed countries, a great expansion of the antidepressant market [1, 2]. Coincidently, use of the illicit drug ecstasy (3,4-methylenedioxymethamphetamine; MDMA) has become more widespread [3], especially among young people [4]. This changing pattern of pharmaceutical and illicit drug use creates a need to delineate more clearly the potential harms that can arise from the concomitant use of ecstasy and other serotonergic drugs or substances. The potentially life-threatening interactions have serious ramifications for people using antidepressants therapeutically who may incidentally use ecstasy. Subsequently, there is scope for psychiatrists and other medical practitioners to be better informed of the associated health risks.
Much of the recent literature on ecstasy relates to emerging evidence of long-term neurotoxicity among heavier ecstasy users [5–12] and debate over whether the substantial ecstasy-related neurotoxicity demonstrated in animal models can occur in humans [5, 13–16]. This has partly overshadowed consideration of serotonin syndrome, one of the acute, potentially serious negative health effects of ecstasy use [17–22].
Serotonin syndrome is a drug-induced toxic state caused by an excess of serotonin within the central nervous system [23]. It is characterized by a cluster of autonomic signs, neuromuscular changes and altered mental status [24]. The most likely clinical presentation of serotonin syndrome is one of rapid onset, usually within 24 h of the introduction of a serotonergic substance [25]. The serotonin release induced by MDMA is mostly responsible for the behavioural and physiological effects experienced by ecstasy users. To a lesser extent, MDMA also inhibits the re-uptake of serotonin and other neurotransmitters such as dopamine [20]. MDMA has clinically relevant serotonergic potency [26], and a large dose can release large amounts of serotonin in the synaptic cleft, with a subsequent 80% loss of brain serotonin within four hours of intravenous use [16]. Persons with serotonin syndrome related to the use of illicit drugs such as ecstasy usually present to emergency departments with more advanced symptoms. This is because some of the early, mild signs of serotonin syndrome are generally perceived by many ecstasy users as being within the range of normal drug reactions [20].
Typically, the serotonin-toxic person is hypervigilant or agitated, with tremor and exaggerated reflexes. Muscle spasms tend to start in the lower limbs and become generalized as toxicity increases; fever, sweating, dilated pupils, rapid heart rate and rapid breathing also become more evident as serotonin syndrome progresses. Other symptoms may include shaking, shivering and clenched jaw. Fixed rigidity develops in severe cases that can impair breathing and lead to raised levels of carbon dioxide in the blood. Confusion, rigidity and body temperature >38.5°C indicate life-threatening toxicity [24, 26].
In cases in which symptoms become severe, transfer to an intensive care unit is recommended [26]. Management is mainly supportive and can include hydration, antihypertensive drugs and anticonvulsants. Cases of severe, late-stage serotonin syndrome may require intubation, cooling, neuromuscular relaxants and serotonin antagonists to reduce hyperpyrexia [26].
This review synthesizes the known risk of serotonin syndrome associated with the concomitant use of ecstasy and other serotonergic substances in a clinically relevant hierarchy for psychiatrists and other medical practitioners.
Method
We conducted a review of all available peer-reviewed and grey literature (non peer-reviewed research reports) up to 2006. Online databases searched included Embase, CINAHL, Medline and PubMed. Search terms included, but were not limited to: ecstasy (MDMA) and other widely used illicit drugs; serotonin syndrome/toxicity; monoamine oxidase inhibitors (MAOIs); selective serotonin re-uptake inhibitors (SSRIs); tricyclic antidepressants (TCAs); reversible inhibitors of monoamine oxidase (RIMAs); serotonin–noradrenaline re-uptake inhibitors (SNRIs); and other known serotonergic pharmaceuticals and supplements. A minority of search terms were sourced from websites related to ecstasy use. Known serotonergic substances were categorized as ‘less risk’, ‘intermediate risk’ or ‘high risk’ of serotonin syndrome when used with ecstasy according to the proportion of agreement between studies. Due to the very varied nature of the studies reviewed, comment on the methodological quality of each study has not specifically been made. In addition, when appropriate, national medical and pharmacological experts were consulted.
Results
Hierarchy of risk
Numerous substances have been implicated in serotonin syndrome including several illicit drugs, antidepressants, opioid analgesics, migraine medication and herbal products [23, 27–30]. When used with ecstasy, these substances have a potential for increased toxicity and are presented in a resulting hierarchy of risk (Table 1).
Serotonergic substances and the risk of serotonin syndrome from concomitant use with ecstasy
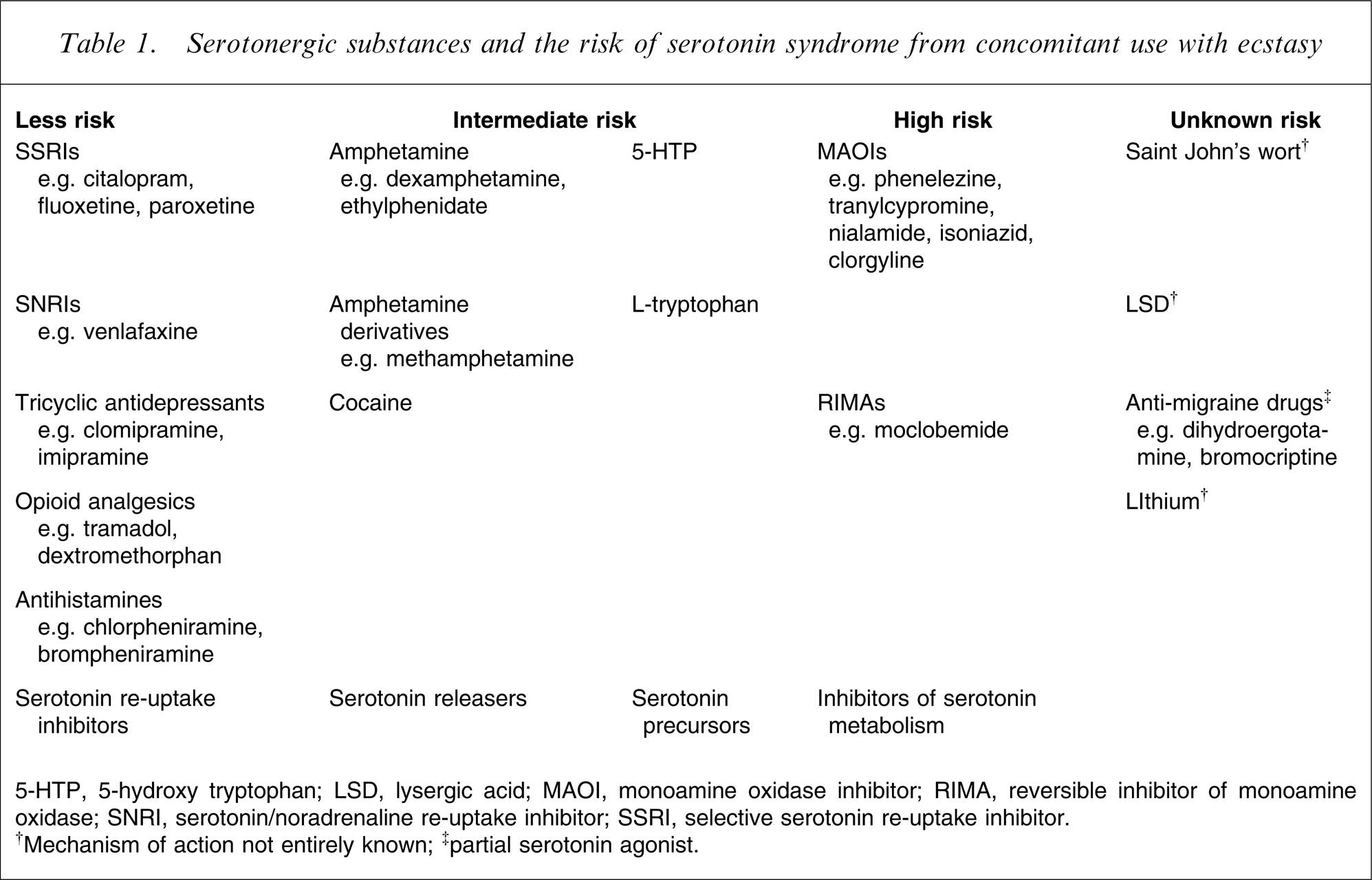
5-HTP, 5-hydroxy tryptophan; LSD, lysergic acid; MAOI, monoamine oxidase inhibitor; RIMA, reversible inhibitor of monoamine oxidase; SNRI, serotonin/noradrenaline re-uptake inhibitor; SSRI, selective serotonin re-uptake inhibitor.
†Mechanism of action not entirely known; ‡partial serotonin agonist.
Less risk
Substances that inhibit serotonin re-uptake are not likely to increase serotonin to life-threatening levels if used with ecstasy [23, 26, 31]. These substances include SSRI antidepressants (e.g. citalopram, fluoxetine, paroxetine), the SNRI venlafaxine, tricyclic antidepressants (e.g. clomipramine, imipramine), opioid analgesics (e.g. tramadol, dextromethorphan) and antihistamines (e.g. chlorpheniramine, brompheniramine). These drugs differ from other serotonergic drugs in that they compete with MDMA at the serotonin receptor site and, therefore, diminish the effects of MDMA [23, 31].
Controlled studies have found that the physiological and subjective effects of ecstasy are substantially reduced in participants given citalopram [32, 33]. Results from animal experiments also show that some SSRIs block the MDMA-induced release of serotonin [31, 34–36]. Interestingly, additional evidence from animal models suggests that some SSRIs may protect against the long-lasting neurotoxic effects of MDMA [36–38]. Whether this is the case in humans is yet to be determined.
Bupropion, initially used in the treatment of depression and now a widely used short-term aid to smoking cessation, is devoid of clinically significant serotonergic effects [39], and therefore concomitant use with ecstasy is unlikely to increase the risk of serotonin syndrome.
Intermediate risk
Because the severity of serotonin syndrome depends on the type of substance ingested and also the quantity [23], the use of ecstasy, a potent releaser of serotonin, with other serotonin releasers or precursors (a substance that gives rise to serotonin after a metabolic process), is likely to lead to a greater risk of serious serotonin syndrome. High doses or repeated use of ecstasy and its analogues intensifies serotonin release [40]. In addition, serious serotonergic symptoms have been reported more frequently when ecstasy is used in combination with amphetamine and cocaine [41].
The pharmaceutical stimulants dexamphetamine and methylphenidate, frequently used in the treatment of attention deficit disorders, are relatively potent releasers of serotonin with some inhibitory effects on serotonin re-uptake [29, 42], as is the amphetamine derivative methamphetamine, commonly known as speed, base or crystal. Amphetamine and MDMA have clinically relevant serotonergic potency [23], and simultaneous use is also likely to increase the risk of serotonin syndrome [43].
The illicit drug cocaine, in addition to enhancing levels of the neurotransmitters dopamine and noradrenaline, is a releaser of serotonin [28, 44–46]. The serotonergic effects of cocaine suggest it may strongly influence the course of serotonin syndrome [25, 28], and possibly even more so if used with ecstasy [43].
The serotonin precursor 5-hydroxy tryptophan (5-HTP) is available as a dietary supplement, extracted from the plant Griffonia simplicifolia [47], and is used as an adjunct in the treatment of depression [48]. A review by Juhl found no reported human cases of serotonin syndrome induced by 5-HTP [49]. Fatalities from serotonin syndrome associated with 5-HTP overdose have, however, occurred in animals [50]. Nevertheless, 5-HTP has demonstrated serotonergic potency [28, 48], and its use with ecstasy is, in theory, likely to precipitate serotonin syndrome.
The serotonin precursor L-tryptophan was once widely used in the treatment of depression and sleep disorders, but now is rarely prescribed. L-tryptophan has demonstrated serotonergic potency [23, 28, 30, 51], and the risk of serotonin syndrome is likely to increase if it is combined with ecstasy, especially if used beforehand.
High risk
The use of ecstasy with MAOI antidepressants such as phenelezine and tranylcypromine, other MAOIs (e.g. nialamide, isoniazid, clorgyline) and the RIMA antidepressant moclobemide is likely to lead to serious increases in serotonin [17, 26]. Moclobemide and MAOIs reduce or prevent the enzyme monoamine oxidase from breaking down various neurotransmitters including serotonin.
Cases of serotonin syndrome from ecstasy interactions with phenelzine have been reported as early as 1987 [22, 52]. The use of ecstasy in combination with moclobemide can give rise to fatalities and a handful of cases have been documented [17]. Further evidence that moclobemide increases the likelihood of severe serotonin syndrome when used with ecstasy comes from animal studies [53]. The long half-life of some MAOIs (e.g. phenelezine, tranylcypromine) means that someone could still be susceptible to interactions with ecstasy up to 2 weeks after they have stopped using this drug class [26, 28].
In a recent Australian study of ecstasy users, approximately one in 25 reported deliberately combining ecstasy and moclobemide [54]. This was regarded by participants as a way to enhance the effects of ecstasy or to ease the recovery period. The study also found that the deliberate use of antidepressants with ecstasy was associated with a greater likelihood of reporting potentially serious effects such as muscle rigidity, nystagmus, dizziness, headache and profuse sweating [55].
Unknown risk
The herbal extract Saint John's wort has serotonergic properties, is typically used in the treatment of depression [56, 57], and has been implicated in serotonin syndrome [28, 58]. The mechanism of action of Saint John's wort, however, has not yet been clearly delineated [28, 29, 59–62]. There is, therefore, potential for interaction between Saint John's wort and other serotonergic agents [59], including ecstasy, which could increase the likelihood of serotonin syndrome.
Lysergic acid (LSD) is structurally similar to serotonin and this characteristic contributes to its serotonergic potency. The precise mechanism of action of LSD is uncertain, but it is thought to have agonistic and antagonistic effects on serotonin [63, 64]. LSD has been implicated in serotonin syndrome but whether it can precipitate symptoms severe enough to be life threatening is yet to be established [27, 29, 65]. The full extent of interaction of LSD with serotonergic agents, including ecstasy and other illicit drugs, is largely unknown.
Anti-migraine drugs such as dihydroergotamine and bromocriptine are partial serotonin agonists and stimulate serotonin receptors [23]. These drugs have not demonstrated any clinically relevant serotonergic potency [26, 66], and the risk of serotonin syndrome from their use with other serotonergic agents, including ecstasy, is presented as more of a theoretical concern.
Relatively little is known about the mechanism of action of lithium, a drug commonly used in the treatment of depression and bipolar affective disorder, but it is thought to act as a partial serotonin agonist [28]. Lithium may potentially contribute to serotonin syndrome, but whether it has clinically relevant serotonergic potency has not yet been established [26].
Discussion
Since the late 1980s only a handful of case reports of ecstasy-induced morbidity and mortality that fit the diagnostic criteria for serotonin syndrome have been described in the literature [17, 18]. Although it seems that the incidence of ecstasy-related fatalities can be described as low compared to the likely frequency of the drug's use [67–70], the extent of acute, non-fatal consequences of ecstasy use is more difficult to estimate. This is because less serious cases are not usually published and ecstasy users who are experiencing distress access a range of medical, health and support services in a variety of settings [68, 71]. Although fatalities from serotonin syndrome associated with overdose of ecstasy alone are relatively rare, when ecstasy is used together with other serotonergic drugs or substances the potential for serious toxicity is greater.
Based on available evidence, this paper synthesizes the associated risk in a hierarchy that is clinically relevant for psychiatrists and other medical practitioners. Substances that inhibit serotonin re-uptake (e.g. SSRIs, SNRIs, TCAs) are less likely to lead to life-threatening elevations in serotonin when used with ecstasy. In contrast, high doses or repeated use of stimulants such as methamphetamine and cocaine with ecstasy intensify serotonin release and increase the risk of serotonin syndrome; as does the use of pharmaceutical amphetamine and ecstasy. The serotonin precursors 5-HTP and L-tryptophan are also expected to influence the course of serotonin syndrome when used with ecstasy. Substances that inhibit monoamine oxidase (e.g. MOAIs, RIMAs) are most likely to lead to serious increases in serotonin when used with ecstasy. Comparatively little is known about the interactions between ecstasy and Saint John's wort, LSD, anti-migraine drugs and lithium. The consequences of these interactions for people using antidepressants therapeutically who may incidentally use ecstasy are potentially serious. Unfortunately, there is evidence that the involvement of medical practitioners in screening for illicit drug use is limited [72–75].
Emerging evidence that a range of serotonergic pharmaceutical drugs and supplements are deliberately combined with ecstasy to achieve a specific effect [19, 55, 76–81], in some cases with serious consequences [17, 55], is of great concern. Anecdotal information from websites related to ecstasy use suggests this practice is not uncommon [82, 83]. The licit substances reported to be deliberately combined with ecstasy include SSRIs, MAOIs, 5-HTP, Saint John's wort and pharmaceutical amphetamine [55, 78]. Evidence of this emerging practice suggests that further exploration of the associated risks is necessary. A further health concern is that ecstasy users tend to use other illicit drugs that have serotonergic potency on the occasions they use ecstasy. Research continues to show that in addition to alcohol and cannabis, the serotonergic stimulants amphetamine and cocaine are also frequently combined with ecstasy [77, 84–87].
Implications for intervention
The potential interactions between ecstasy, other illicit drugs and pharmaceutical medications remains a largely underresearched area. There is a need to more clearly define strategies that will inform users of the consequences of using ecstasy with antidepressants and other drugs or substances that act on serotonin. Findings highlight the importance of screening for the use of ecstasy and other serotonergic substances when prescribing antidepressant drugs. Serotonin syndrome is a potentially serious but preventable condition. A comprehensive response requires early identification and ongoing support of patients who present with symptoms of illicit drug use, particularly ecstasy-related depression. Psychiatrists and medical practitioners are well placed to respond to people with mental health problems related to illicit drug use. Consequently, there is scope for developing materials that may help to improve the screening of patients who are prescribed antidepressant drugs and other serotonergic pharmaceuticals.
Footnotes
Acknowledgements
This paper originated from a study funded by the Australian Government Department of Health and Ageing.