
Abstract
Introduction
Serotonin syndrome (SS) is a drug-induced constellation of various clinical features that result from excess central serotonergic tone. The clinical features range from barely perceptible to life-threatening conditions.
Cases
We describe four patients with acute headache (four days to three weeks) who were receiving serotonergic drugs for other indications. There was a temporal relation between the administration of the serotonergic drugs and the development of the headaches. All four patients fulfilled the Hunter Serotonin Toxicity Criteria for SS. In parallel, two patients fulfilled the Sternbach’s criteria for SS. Discontinuation of the serotonergic drugs and the administration of cyprohepatadine led to complete improvement in three to seven days in all four patients.
Discussion
A review of the literature suggests that some overlaps exist in the pathophysiology between SS and headache disorders, including medication-overuse headache. The overlap is also in the management. The drugs found to be effective in SS (cyproheptadine, chlorpromazine, olanzapine, etc.) are also known to have positive effects on some headache disorders.
Conclusion
Physicians should consider the diagnosis of SS in patients with new onset or worsening headache after the addition of serotonergic drugs, especially in the presence of objective signs on examination suggestive of the disorder such as tremor, fever, hyperreflexia, diaphoresis or tachycardia.
Introduction
Serotonin syndrome (SS) is an iatrogenic, drug-induced constellation of various clinical features. It is often described as a clinical triad of neuromuscular hyperactivity, autonomic hyperactivity and altered mental status. However, the clinical features may range from barely perceptible to lethal. The syndrome may be missed because of its protean manifestations. SS in its mild form may be easily overlooked by the majority of clinicians and patients. Clinicians and patients may dismiss mild symptoms such as tremor, diarrhea or hypertension as inconsequential or unrelated to drug therapy (1).
Headache as a symptom is not a part of clinical features in any diagnostic criteria. However, headache is described as one of the accompanying features in a few patients with SS (2). Herein, we describe four patients (collected over one year) with SS in whom headache was the presenting or prominent feature.
Case series
Case 1
A 22-year-old man presented with a two-week history of headache. The headache was continuous since the onset, nonthrobbing, holocephalic and mild for most of the time. However, occasional exacerbations occurred, escalating to moderate to severe intensity for a few (two to six) hours. The exacerbations did not get worse with his routine physical activities. The patient denied the presence of nausea, vomiting, photophobia, phonophobia, auras or cranial autonomic features. There was no significant prior history of headache. The patient was receiving tramadol/acetaminophen combination (37.5/325 mg three times daily (tid)) for two weeks for a right ankle sprain. The headache started one to two days after initiation of the drug. Physical and neurological examinations revealed tachycardia (118 beats/minute), mydriasis, mild postural tremor of both hands and generalized hyperreflexia. Routine biochemical investigations (including thyroid profiles) were normal. Magnetic resonance imaging (MRI) of the brain was reported as normal. Cerebrospinal fluid (CSF) examination revealed no abnormality.
The patient fulfilled the Hunter Serotonin Toxicity Criteria for SS (3). Tramadol was discontinued, and cyproheptadine was started at a dose of 8 mg tid. Within 10 hours of the administration of cyproheptadine, the headache started to improve. After 72 hours, the headaches, tremor and hyperreflexia resolved completely. Cyproheptadine was continued for another three days. In the next three months of follow-up, the patient was symptom free.
Case 2
A 34-year-old male was under the supervision of a psychiatrist for anxiety and depression. He received various combinations of drugs in the last 12 months. The patient had been receiving paroxetine (25 mg/daily) and clonazepam (0.5 mg daily) for four to five weeks. The patient reported to our outpatient clinic for near-daily headache lasting for two to three weeks. It was described as holocephalic, pressing and as mild to moderate for most of the time. The patient denied the presence of nausea, vomiting, photophobia, phonophobia or any cranial autonomic features. There was no significant past history of headache.
Physical and neurological examinations revealed tachycardia (122 beats/minute), raised blood pressure (156/94 mmHg) and postural tremor of both hands. Both lower extremities were rigid and hyperreflexic, with five-beat, inducible ill-sustained ankle clonus. Routine hematological and biochemical investigations (including thyroid profiles) were normal. MRI brain and CSF examination revealed no abnormality.
The patient fulfilled the Hunter toxicity criteria for SS (3). We stopped paroxetine. Cyproheptadine was started at a dose of 8 mg tid. Within 24 hours, the headache started to improve. After one week of the treatment with cyproheptadine, the headaches, tremor, rigidity and hyperreflexia resolved completely. Cyproheptadine was continued for another week. In the next three months of follow-up, the patient was symptom free.
Case 3
A 36-year-old female patient presented with a four-day history of headache. The headache was holocephalic, of pressing type and continuous since onset. The headache fluctuated from moderate to severe in intensity. The patient occasionally felt nausea, photophobia and phonophobia with the exacerbations of the headache. There was no significant prior history of headache. She had been taking tramadol/acetaminophen combination (37.5/325 mg) twice a day and fluoxetine (20 mg) for the last seven days for low back pain. The clinical examination revealed tachycardia (118 beats/minute), mydriasis, postural tremor and hyperreflexia. The body temperature was mildly elevated (37.8℃). Routine hematological and biochemical investigations were normal. MRI brain revealed no abnormality.
The patient fulfilled both Sternbach’s and Hunter toxicity criteria for SS (2,3). All medications were discontinued, and cyproheptadine was administered at a dose of 8 mg tid. Within six hours of the administration of the first dose, the headache started to improve. The headache subsided completely in 48 hours. Abnormal physical examinations (mydriasis, postural tremor and hyperreflexia) returned to normal in 72 hours. Cyproheptadine was continued for another four days. In the next two months of follow-up, the patient was symptom free.
Case 4
A 46-year-old man had a long-standing history of chronic low back pain. He had been receiving fluoxetine (40 mg daily) and tramadol/acetaminophen combination (37.5/325) for the previous four weeks. Ondansetron (8 mg two times daily) was added for the development of nausea and vomiting five days earlier.
The patient was referred to our neurology outpatient clinic for evaluation of headache, restlessness and disturbed sleep of four days’ duration. The headache had been continuous since the onset. The headache started gradually and became severe in about three to four days. It was described as holocephalic and throbbing in character. The patient had nausea and vomiting before the development of headache (for which he was on ondansetron). The nausea and vomiting reduced in intensity and frequency. There was no significant prior history of headache or history of trauma to the head.
The physical and neurological examinations revealed tachycardia (126 beats/minute), mildly elevated temperature (37.6℃), mydriasis, postural hand tremor, rigidity in both lower limbs and ill-sustained clonus (three to five beats). Meningeal signs were not noted. Routine hematological and biochemical investigations were normal. MRI brain and CSF examination revealed no abnormality.
The patient fulfilled both Sternbach’s and Hunter toxicity criteria for SS. All three drugs were discontinued and cyproheptadine was started (8 mg tid). The symptoms started to improve after 36 hours and subsided completely within three days. Cyproheptadine was continued for another three days. He remained headache free after 10 weeks of follow-up.
Discussion
SS is an underdiagnosed condition. Less severe cases are highly underdiagnosed (1). Earlier diagnostic criteria emphasized the mental status changes for SS (2,4). These criteria have been criticized for not including the wider spectrum of clinical features. For this reason, some authors advocate using the term “serotonin toxicity” to include milder cases (3). All four of our cases fulfilled the Hunter Serotonin Toxicity Criteria. All four patients had tremors and hyperreflexia/inducible ill-sustained clonus. In parallel, two patients (Cases 3 and 4) also fulfilled the Sternbach criteria for SS.
Patients with SS usually present within six hours after the initial use of a serotonergic drug (1). However, mild manifestations may present with more prolonged course (with subacute/chronic onset) (1). In three of our patients (Cases 1, 3 and 4), the onset of headache was acute and there was a clear temporal relation between the administration of the drug(s) and the development of clinical features suggestive of SS. In Case 2, symptoms suggestive of SS started three to four weeks after the administration of serotonergic drugs. In Case 4, the patient was already on fluoxetine and tramadol/acetaminophen combination for four weeks. The addition of ondansetron led to the development of SS. All patients were receiving multiple medications. Each of these medications has been reported to cause SS (1).
Headache was one of the accompanying features in two patients in Sternbach’s review of the literature (2). In a few other case series, the prevalence of headache in patients with SS was about 4% (4). In Richard et al.’s observation (5), one patient (with a past history of headache) showed worsening of headache (with diaphoresis) after a few weeks of the administration of an antidepressant. Symptoms improved after the discontinuation of fluoxetine. This case highlights that headache may be a prominent feature in patient with SS. Terao and Hikichi (6) reported a 65-year-old female with SS who had dysarthria, tremor and headache caused by paroxetine. Discontinuation of paroxetine led to the improvement of the symptoms. Alnwick (7) reported a 42-year-old female patient who was on an antidepressant for a long period. Over the years, she developed chronic headache. Later on, she had pain in other parts of the body with various other clinical features. A diagnosis of fibromyalgia was made. However, a careful examination suggested a possibility of SS. Discontinuation of the offending drugs led to complete improvement. This case highlights that even chronic headache (and chronic pain) may be part of the symptom complex of SS.
To the best of our literature search, headache as a presenting feature of SS has not been reported in the past.
Drug-induced headache may be associated with other symptoms such as dizziness, fatigue, drowsiness or agitation, tremors and insomnia (8). These features are common in patients with SS. Therefore, we speculate that in a subset of patients, drug-induced headache may be caused by SS.
Prevalence or incidence of clinical features suggestive of serotonin syndrome (according to the Hunter Serotonin Toxicity Criteria) as side effects of the drugs used by our patients.
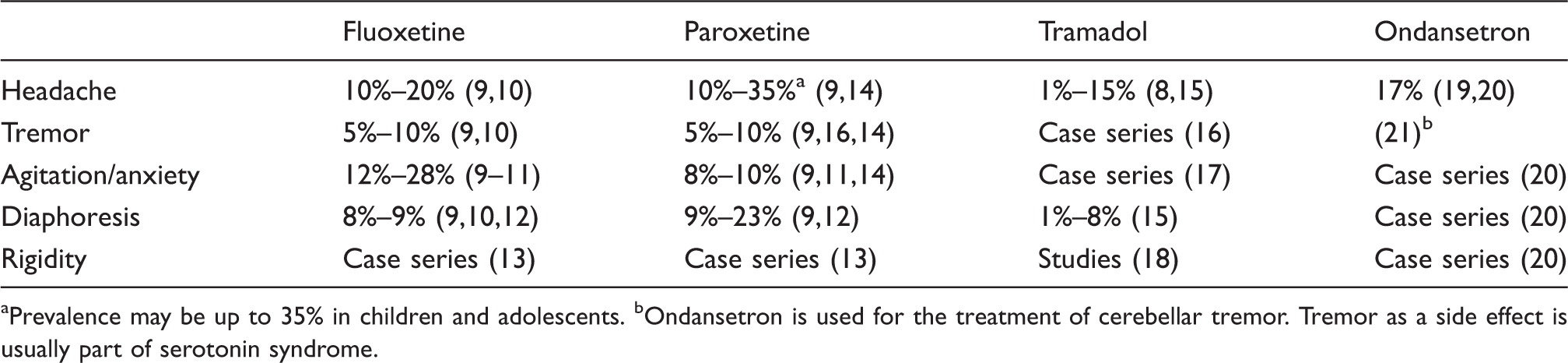
Prevalence may be up to 35% in children and adolescents. bOndansetron is used for the treatment of cerebellar tremor. Tremor as a side effect is usually part of serotonin syndrome.
Tremor, agitation and excessive sweating were quite common as side effects of selective serotonin reuptake inhibitors (SSRIs) (fluoxetine and paroxetine) (Table 1). These symptoms, as side effects, were also noted with tramadol and ondansetron. These side effects were not considered as a part of SS in these patients. However, a possibility of SS exists as these patients were not subjected to examination for deep tendon reflex or clonus. SSRIs (fluoxetine and paroxetine) and opioid analgesics (tramadol) are useful in patients with headache disorders. However, these drugs may cause headache, and headache has been observed as a side effect in patients in whom these drugs were used for an indication other than headache (Table 1). Headache as a side effect was frequent with all four of these drugs. Therefore, we speculate that in a subset of patients, drug-induced headache may be part of the symptom complex of SS, as both headache and symptoms suggestive of SS are common side effects to serotonergic drugs.
Several drugs that can cause SS are frequently used in migraine and other headache disorders. Therefore, if the headache is related to SS, worsening of headache should be observed in these patients. However, review of the literature did not suggest such observations. Nevertheless, headache is one of the side effects of these drugs in patients in whom these drugs are used for an indication other than headache (8–10). Therefore, prospective study is required to confirm such observations.
Serotonin, SS and headache: Pathological correlation
Serotonin is a neurotransmitter (5-hydroxtryptamine (5-HT)) found in many tissues, including in the central nervous system. Serotonin receptors are classified into seven families (5-HT1 to 5-HT7). The 5-HT2A receptor is the main receptor implicated in serotonin toxicity (1,22). The 5-HT1A receptor may also contribute substantially to the development of serotonin toxicity (1). Three of our patients were on SSRIs, which induce serotonin toxicity by inhibiting the reuptake of serotonin. Three patients were on tramadol. Tramadol can cause SS as it is also a weak serotonin reuptake inhibitor. Case 4 was receiving fluoxetine, tramadol and ondansetron. SS developed after the addition of ondansetron. Each of these drugs can cause SS independently. Ondanserton is a 5-HT3 antagonist. It is proposed that blockade of the 5-HT3 receptor results in increased synaptic concentration of serotonin at the unblocked 5-HT2A and 5-HT1A (23,24). Moreover, ondansetron (and tramadol) are metabolized by cytochrome P 450. Fluoxetine and other SSRIs are potent blockers of cytochrome P 450, resulting in deceleration of both ondansetron and tramadol metabolism.
The interrelationship between headache and SS is usually described in relation to the side effects of triptans, and a few case reports hint that SS can be caused by triptans (usually in combination with SSRIs). However, an American Headache Society (AHS) position paper suggests that there is insufficient data/information to determine the risk of SS with triptans (25). Triptans are agonists at the 5-HT1B/1D/1F receptor subtypes, with weak affinity for 5-HT1A receptors and no activity at the 5-HT2 receptors. Triptans appear unlikely to cause SS based on their biological actions.
Available evidence shows that serotonin, when released at higher concentration, binds to 5-HT2A receptors and induces a migraine attack (22). Upregulation of 5-HT2A receptors may be a mechanism for the development of chronic daily headache (22,26). A role of these receptors has been observed even in patients with medication-overuse headache (27). An increase in density of 5-HT2A has been demonstrated in platelets in patients with analgesic-overuse headache. After the drug withdrawal, the receptors’ density was decreased and the headache became less frequent (28). Srikiatkhachorn et al. (29) suggest that activation of 5-HT2A receptors leads to an enhancement of nitric oxide (NO) production in the trigeminovascular pathway. NO may trigger a headache attack.
These all suggest that activation of 5-HT receptors (especially 5-HT2A) is a common pathophysiology both in SS and headache disorders (including medication-overuse headache). Various observations have demonstrated that drugs with the property of blockading 5-HT2A receptors have a positive response in SS as well as in various headache disorders. Cyproheptadine, chlorpromazine and olanzapine (drugs with the property of blockading 5-HT2A receptors) have shown good efficacy in SS and headache disorders (1,30–32). These drugs (cyproheptadine, chlorpromazine and olanzapine) all have many other pharmacological properties (antidopaminergic, antihistaminic, etc.). Therefore, a possibility also exists that these may act in different ways (other than blockading 5-HT2A).
Taken together, there are some overlaps in the pathophysiology and management between SS and headache disorders. Therefore, a possibility of headache as an isolated or prominent feature exists in patients with SS, and our clinical observation (headache as a presenting feature of SS) is in accordance with the known pathophysiology of SS and headache disorders.
We suggest that patients with acute/subacute onset headache (who are on serotonergic drugs) should be examined for tremor, hyperreflexia, mydriasis and other features of SS. Discontinuation of the offending drug and the administration of cyproheptadine for a few days may be sufficient for such patients. It is hoped that these cases may serve as a catalyst for further studies to clarify the issue. It would be interesting to compare the clinical features of SS in patients with and without prior primary headaches. It will bring some insight to the interrelation between SS and headaches.
Limitations of the study
This is a case series and a possibility of unrecognized selection bias exists. Moreover, the prevalence of headache disorders is very common in the general population. Therefore, a possibility of coincidence also exists.
Clinical implications
Serotonin syndrome (SS) is an underdiagnosed iatrogenic drug-induced clinical syndrome. We describe four patients in whom headache was a presenting feature of SS. Early diagnosis in such patients will prevent unnecessary investigations and treatment.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.