
Abstract
Many children and adolescents experience mental disorders during their development. For example, Sawyer et al. estimated that the prevalence of mental health problems among children in Australia was 14% (for brevity the term ‘children’ will be used to refer to ‘children and adolescents’) [1]. The World Health Organization estimated that 10–20% of children experience one or more mental disorders and identified mental disorders as a major contributor to the ‘global burden of disease’ [2].
Epidemiological studies have shown that general practitioners and paediatricians are the medical professionals most commonly consulted to obtain help for childhood mental health problems [1, 3, 4]. Consistent with this pattern, several studies have reported that children attending general practitioners have a high prevalence of mental health problems [5–8]. For example, Kramer and Garralda reported that 38% of 136 adolescents aged 13–16 years who attended a general practice in London had experienced a psychiatric disorder in the previous year [7]. In the USA, Lavigne et al. reported that 21% of 3860 children aged 2–5 years who attended paediatric practices in Chicago had a mental disorder [8].
The key role that general practitioners play in assessing and treating childhood mental health problems poses a challenge for undergraduate medical teaching programmes because a substantial number of medical graduates choose a career in this area [9–12]. For example, in Australia, 42% of the 386 medical students who graduated between 1980 and 1995 at Monash University were working in general practice in 2003 [12]. Similarly, in the USA, 44% of medical graduates in 2002 chose a residency in primary care specialties, including internal medicine, family medicine, and paediatrics [9].
The shortage of child psychiatrists in Australia and many other countries requires general practitioners and paediatricians to take responsibility for assessment and management of childhood mental health problems [13–16]. In light of this, it is concerning that both groups appear to have difficulty recognizing and managing mental health problems [17–21]. For example, in a national audit of general practices in Australia, Hickie et al. found that general practitioners did not recognize mental disorders in 56% of patients identified as having a mental disorder by means of a self-report questionnaire [18]. Similarly, Dulcan et al. found that paediatricians in the Pittsburgh metropolitan area, USA, identified only 17% of the 52 children who received an independent psychiatric diagnosis [17].
Previous surveys of undergraduate child psychiatry teaching have reported that, on average, undergraduate child and adolescent psychiatry teaching programmes occupied a very small proportion of the total time available for teaching at medical schools. Furthermore, there was great variation in the time allocated to teaching child psychiatry in individual medical schools (0–439 h) [22–27]. In most countries only a small number of child psychiatrists have academic appointments and child psychiatry programmes are developed and taught by a small number of teaching staff at each medical school [unpublished data, 2007]. Although further opportunities exist at a postgraduate level for teaching child psychiatry, teaching at an undergraduate level provides a key opportunity to develop initial skills and positive attitudes in future medical practitioners.
The aim of the present study was to identify the goals, content, and time allocated for undergraduate child psychiatry teaching in Australian medical schools. To the best of our knowledge this is the first survey specifically designed to describe child psychiatry teaching at a national level in Australian medical schools.
Methods
From November 2006 to March 2007, all 15 medical schools in Australia were contacted by email and telephone. At this initial contact the member of staff responsible for the child psychiatry teaching programme in each school was identified. Subsequently, this person was contacted and asked to participate in a telephone survey. The participants included five professors in child psychiatry, one associate professor in child psychiatry, one associate professor in paediatrics, one senior lecturer in child psychiatry, one senior lecturer in paediatrics, one lecturer in psychiatry, and two coordinators of teaching programmes in paediatrics (within which the child psychiatry teaching was delivered).
A structured questionnaire was designed by the authors specifically for use in this survey. The questionnaire asked participants to identify their school's teaching objectives, the relationship between child psychiatry teaching and other medical undergraduate teaching programmes, the teaching methods used and the number of hours each teaching method was utilized, the discipline and academic title of teachers, the time allocated for clinical placements in child psychiatry, the number of child psychiatry staff in the school, and the methods used to assess students’ knowledge of child psychiatry. This content was based on a review of previous relevant publications [28] and discussions with staff responsible for teaching child psychiatry in Australia and overseas. Participants were also asked to identify the number of hours they considered was required for teaching child psychiatry, the barriers they experienced in teaching child psychiatry, and potential solutions to overcome these barriers. Finally, participants ranked eight objectives in order of importance for child psychiatry teaching programmes using an 8-point response scale on which 1 was labelled ‘lowest priority’ and 8 was labelled ‘highest priority’. These objectives were identified from a review of previous studies in this area [unpublished data, 2007].
The questionnaire was mailed to participants to allow them time to gather relevant information. Their responses were then obtained during a telephone interview with each participant.
Results
Twelve medical schools participated in the survey (response rate: 80%). The three schools that did not participate had only just been established and were in the early stages of developing teaching programmes. Of those that participated, five schools (42%) had a 6 year undergraduate medical programme, four (33%) had a 5 year programme, and three (25%) had a 4 year programme.
Teaching objectives
All 12 medical schools provided some teaching in areas relevant to child psychiatry. Seven schools (58%) had written objectives for teaching in this area. The most common objectives were (i) knowledge about management and treatment of child psychiatric disorders; (ii) knowledge about child psychiatric disorders; (iii) skills to perform an assessment interview with children and families; (iv) knowledge about the relationship between psychosocial and physical problems; and (v) knowledge about principles of child development.
In four schools (33%), child psychiatry was taught in the paediatric programme, in two schools (17%) in the general psychiatry programme, and in three schools (25%) it was taught in both the paediatric and general psychiatry programmes. In one school (8%) it was taught in a ‘human lifespan development’ programme. This school also offered a 67 h elective in child psychiatry that included clinical teaching.
Time allocated for teaching
Time assigned for child psychiatry teaching programmes ranged between 4 and 12 h, with the exception of one school, which allocated 46 h for child psychiatry teaching. There was little difference in the amount of time assigned for child psychiatry teaching in medical schools with courses lasting 4 years, 5 years, and 6 years.
Teaching methods
Lectures were the most common teaching format, being utilized in 11 schools (92%; Table 1). The remaining school used a problem-based learning approach involving seminars and live observation of interviews with children or families. Among the schools using lectures, content included (i) child development, and health from childhood to adulthood; (ii) assessing children and families; (iii) paediatric psychopharmacology; (iv) attention deficit/hyperactivity disorder; (v) cognitive behavioural approaches in paediatrics; and (vi) autism.
Teaching methods used by medical schools (n = 12)
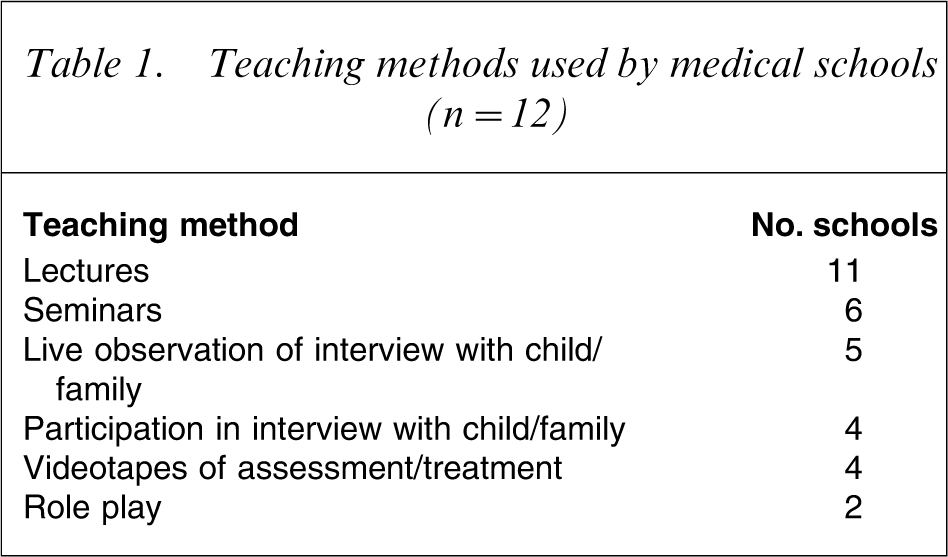
Seminars and live observations of interviews with children or families were the second most common teaching method, being used by six schools (50%) and five schools (42%), respectively. Only four schools (33%) provided specific teaching in the context of student interviews with children or families, while two schools (17%) used role play (Table 1).
Teaching staff
In nine schools (75%) teaching was provided by child psychiatrists. The teaching of child psychiatry was also done by general psychiatrists, clinical psychologists, and paediatricians. In the remaining three schools (25%) no child psychiatrists participated in the teaching programme.
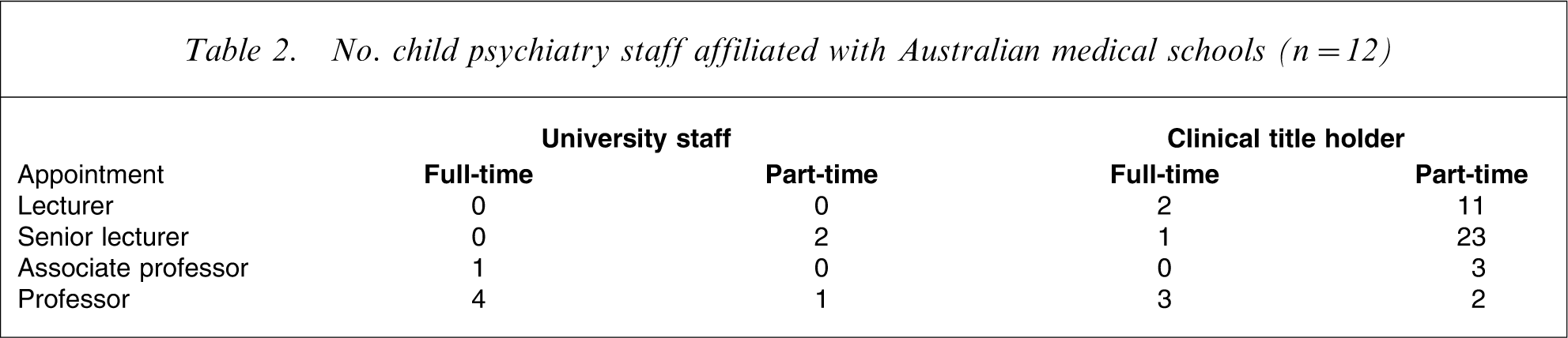
The number of academic staff and clinical title holders is shown in Table 2. Ten schools (83%) had child psychiatrists appointed as academic staff or as clinical title holders. However, only 9% of the child psychiatry staff affiliated with medical schools had full-time academic appointments. The majority of child psychiatrists (70%) associated with medical schools were clinical title holders appointed at the lecturer or senior lecturer level (Table 2). Two schools (17%) did not have any child psychiatrists on their staff.
No. child psychiatry staff affiliated with Australian medical schools (n = 12)
Clinical placements
Only four schools (33%) provided all students with a clinical placement in child psychiatry. These placements ranged in length from 0.5 days to 2 weeks. Another six schools (50%) reported that some students (2–50% of all students) were given a placement in child psychiatry, varying in duration from 4 h to 8 weeks. Two schools (17%) did not offer a clinical placement or an elective in child psychiatry. However, both these schools reported that students undertook a 2 week placement in paediatrics that contained some child psychiatry elements.
Assessment of child psychiatry knowledge and skills
Child psychiatry was assessed by some form of examination in all schools. This was always undertaken in conjunction with other disciplines, most commonly paediatrics. A range of assessment methods were used, including clinical examination (e.g. objective structured clinical examinations, OSCEs), multiple choice questions, case reports, essays, and written examination.
Priorities for teaching objectives
Participants were asked to assign priority scores to each of eight teaching objectives (Table 3). On average, the objectives ‘skills to assess families and children’ and ‘knowledge about normal development’ were given the highest priority. The objectives ‘knowledge of the services available, how to use psychiatry consultation, and how to make a referral’ and ‘skills to recognize factors that may be influencing the presentation, course, or compliance with treatment’ were assigned the lowest priority.
Mean priority for teaching objectives (n = 12)
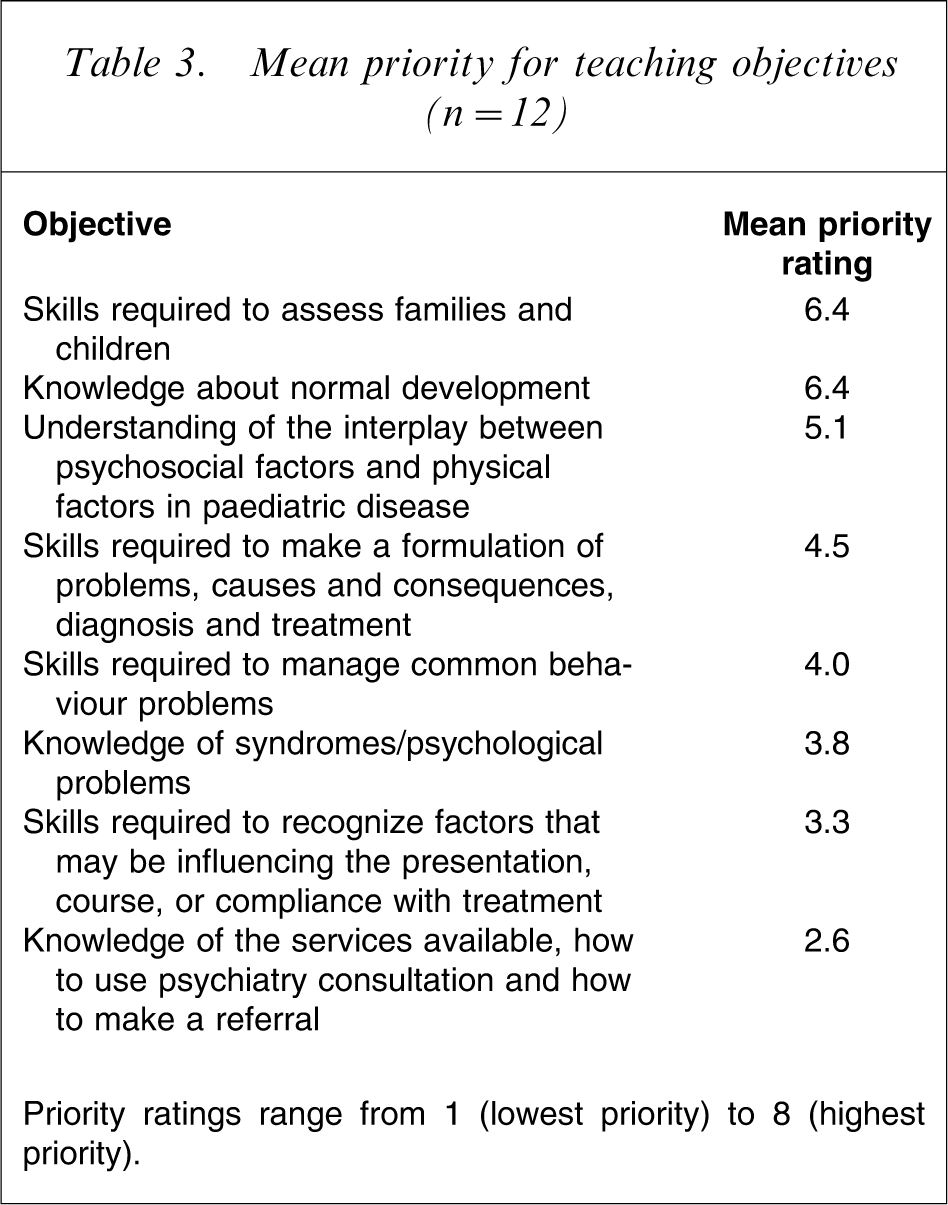
Priority ratings range from 1 (lowest priority) to 8 (highest priority).
Participants were also asked what they considered to be the minimum number of hours that should be provided for child and adolescent psychiatry. On average, they reported that 31 h (range, 5–80 h) were needed to teach child and adolescent psychiatry.
Barriers
Nine participants (75%) identified the lack of academic child psychiatrists in Australia as a barrier to teaching child psychiatry. Seven participants (58%) reported that difficulty fitting the subject into the medical curriculum was a barrier. Reasons given for this were the limited time assigned for teaching child psychiatry, poor cooperation between disciplines, and/or lack of recognition and interest in the speciality of child psychiatry. Three participants (25%) reported that lack of access to patients was a barrier to teaching in the specialty.
Proposed solutions
Three approaches were identified to overcome barriers to child psychiatry teaching. Four participants (33%) suggested that greater effort should be made to advocate for recognition of the importance of child psychiatry teaching in medical school teaching programmes. Two participants (17%) suggested that child psychiatry teaching programmes need to be made more attractive for medical students. Finally, two participants (17%) suggested that greater effort should be made to coordinate child psychiatry curriculum development at a national level.
Discussion
This is the first survey of child psychiatry teaching programmes provided in medical schools in Australia. The only previous survey of psychiatry teaching in Australia focused on general psychiatry teaching programmes [28].
There were three key findings from the survey. First, although all participating medical schools provided some teaching relevant to child psychiatry, the number of hours allocated to teaching in this area was very small. Lectures and seminars were the most common teaching methods used in teaching programmes. Second, only 9% of child psychiatrists affiliated with medical schools had a full-time academic appointment. The vast majority of child psychiatrists held clinical titles, most commonly at the level of lecturer or senior lecturer. Finally, with the exception of two schools that offered no clinical placements in child psychiatry, most schools offered some access to clinical placements in the discipline. However, in several schools these placements were available only for very short periods of time and/or for limited numbers of students.
The amount of teaching provided in child psychiatry to undergraduate medical students is not consistent with the large public health problem posed by child and adolescent mental disorders. These disorders have now been identified as being among the most common health problems experienced by children and adolescents in the community [2]. During the last decade, an increasing number of new effective interventions have been developed to treat children and adolescents with these disorders [29, 30]. Given the key role that general practitioners play in the assessment and management of children with these disorders, it is essential that they receive appropriate training at both the undergraduate and postgraduate level.
The lack of child psychiatrists with full-time academic appointments in Australian medical schools is a significant barrier to the development of strong teaching and research programmes in this discipline. It is striking that 85% of child psychiatrists with university appointments are clinical title holders, with the vast majority having appointments at the lecturer or senior lecturer level. Until more child psychiatrists with relevant experience are recruited to senior full-time academic appointments in Australian medical schools, it will be very difficult for the discipline to develop strong teaching and research programmes in this country. In turn, this will limit the teaching provided to undergraduate students, which is needed to ensure that the medical profession can play an effective role in helping to reduce the number of child and adolescent mental disorders in the community.
The findings from the survey are similar to those of previous surveys of undergraduate child and adolescent psychiatry programmes in England, Japan, USA, Europe, and Canada [22–27]. However, the teaching time of 4–12 h allocated in most Australian medical schools was less than that reported in other countries. For example in Canada, an average of 26 h was utilized for child psychiatry teaching, while in European medical schools, an average of 20 h is allocated for teaching in this area [24, 26]. Only limited information is available about the time allocated to teaching of other subspecialty psychiatry areas in Australia. O'Connor et al. reported that on average, the total time available for clinical teaching in psychiatry across 12 universities was 353 h, of which 8 h was allocated to alcohol and drug programmes, 4 h to old age psychiatry and, consistent with the findings from the present study, 12 h to child psychiatry [28].
While the benefits of teaching methods that encourage an active role for students have been widely acknowledged [31, 32], lectures and seminars remain the most commonly used child psychiatry teaching methods in Australian medical schools. In the present study, only six medical schools (50%) provided all students with the opportunity to participate in assessment interviews with children. In some schools this occurred as part of a specific teaching programme, while in others it was available during clinical placements. Of concern was the finding that some medical schools provide no clinical placements or electives in child psychiatry.
The strengths of the survey are its high participation rate and the use of direct interviews with key informants knowledgeable about the child psychiatry teaching programmes. Limitations include the lack of detail about the content of specific child psychiatry teaching programmes. To keep the project to manageable proportions, the survey focused on the amount of time provided for child psychiatry teaching in medical school programmes. However, it is important to note that this does not provide information about the quality and effectiveness of teaching programmes. It is also important to recognize that the survey focused specifically on child psychiatry teaching programmes. It is possible that additional teaching relevant to child psychiatry is provided in other teaching programmes, particularly those that utilize problem-based learning.
In conclusion, the limited child psychiatry teaching provided to medical students is concerning given the high rates of mental health problems among children and adolescents in the community, the lack of specialist child psychiatry services, and the key role that general practitioners and other primary care health providers play in the assessment and management of child and adolescent mental disorders. The priority given to undergraduate child psychiatry teaching in medical schools needs to be consistent with the size of the public health problem posed by child and adolescent mental disorders. However, it will be very difficult for the small number of people responsible for child psychiatry teaching programmes at each university to overcome these problems if they work independently from each other. There is a need for child psychiatry teaching staff to better coordinate their activities at a national level when setting teaching goals, designing curricula, developing teaching resources, and advocating for undergraduate child psychiatry teaching.
Footnotes
Acknowledgements
This study has been funded by the Australian Rotary Health Research Fund. The authors also wish to thank Prue McEvoy (University of Adelaide) for her help with the present study and the medical schools that participated in the survey.