
Abstract
Child and adolescent psychiatry has an opportunity to adapt alongside the advancements in medical knowledge, post-graduate training, epidemiological realities and clinical service models. Here, we are guided by the mental health needs of our community’s young and their families in our review of child and adolescent psychiatry training in Australia and New Zealand. We recognise that training must respond to clinical demand and service reform while ensuring a range of clinical and educational experiences to deliver expectable competencies in order to produce child and adolescent psychiatrists that meet the communities’ needs now and in the future. We argue that training programmes be subject to rigorous evaluation by embedding continuing cycles of improvement including regular review and international bench marking.
Child and adolescent psychiatry (CAP) began as the first subspeciality group of the Royal Australian and New Zealand College of Psychiatrists (RANZCP) concurrent with the formation of the College in 1964 (Rubinstein and Rubinstein, 1996). A recent revision of RANZCP training (Figure 1) has coincided with major shifts in child and adolescent mental health service design in addition to escalating clinical demand. Here, we examine such developments and benchmark training against international standards and experience (Deschamps et al., 2020; Deschamps and Jacobs, 2020; Jacobs et al., 2018).
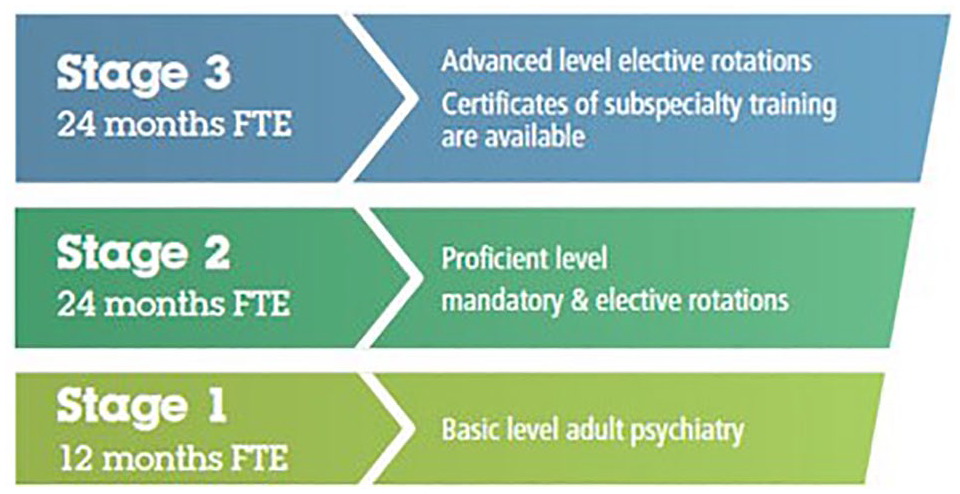
Training structures and governance in Australia and New Zealand.
What the community needs from CAP
Child and adolescent mental health needs in Australian and New Zealand (ANZ) are not adequately met. Australian community survey data show that one in seven children and adolescents have experienced a recent mental health disorder (Lawrence et al., 2015). Not all cases need direct clinical care from a CAP. However, only 48.9% of these children and 65.1% of adolescents accessed any clinical care (i.e. helpline, school counsellor or clinical service). Further demonstrating the high levels of unmet need, only one quarter of the 2.1% of children and young people with severe mental illness saw either a general or child and adolescent psychiatrist (Figure 2; Lawrence et al., 2015; RANZCP, Faculty of Child and Adolescent Psychiatry, 2019). This unacceptable treatment gap is similar in New Zealand (Ramage et al., 2005).

Clinical training experience in Australia and New Zealand.
The stepped-care response to this challenge is limited by a lack of access to CAPs for primary healthcare providers and paediatricians (Paton et al., 2021). Moreover, training in this consultative and educational role for CAP is currently de-prioritised relative to acute care service provision (Figure 2). Within the public sector, where most training in ANZ occurs, increasing mental health presentations of adolescents to emergency departments is dominating service delivery and, subsequently, the clinical experience for trainees (Hiscock et al., 2018; Perera et al., 2018). We argue that training experiences are disproportionately determined by crisis-oriented service demands relative to College curriculum or broader community needs which indicate the need to train CAPs with a broader set of competencies. In particular, training experiences with children (0–12 years) are dwindling.
Defining the role of the CAP and determining workforce requirements to meet community needs must guide training imperatives (RANZCP, Faculty of Child and Adolescent Psychiatry, 2018, 2019). Clarifying the role of CAPs, beginning with medical expertise in child and adolescent mental illness and extending to collaboration, leadership and advocacy helps identify the required competencies for training (RANZCP, Faculty of Child and Adolescent Psychiatry, 2018). Projections of the number of CAPs for adequate service provision throughout ANZ indicate a large shortfall now and into the future (RANZCP, Faculty of Child and Adolescent Psychiatry, 2019). Fortunately, applicant demand exceeds supply and, therefore, workforce challenges could be alleviated by increasing the number of training positions.
Leadership and governance of training
The conceptual design and accreditation of training is a College responsibility. However, in practice, the funding and delivery of clinical services where training positions are located is the purview of the healthcare services themselves. Greater clinical demand, particularly in emergency departments, creates tensions between training imperatives and clinical services. These tensions are somewhat balanced – in terms of ensuring that trainees have a sufficiently broad experience – by the psychiatrists who direct and supervise training locally, in addition to College accreditation processes. Compounding the influence of crisis-oriented care demands, most training occurs in state-funded clinical services that provide for only the small percentage of the population with the most severe problems (Figure 2). On international comparison, we argue, our training is heavily influenced by service provision, skewing it to high acuity care of adolescents. We suggest a greater need for the College to ensure that training is determined by the curriculum, designed to meet broad future community needs and that this is assured by greater monitoring, evaluation and accreditation of training. Increased cooperation between policy makers, funding agencies, health services and training providers is required to balance resources for immediate service needs against training and workforce development requirements. This requires greater College leadership.
We submit that College mechanisms for oversight and accreditation of CAP training have eroded. The design of CAP training, a College responsibility, has no requisite peer-review or cyclical evaluation framework. Advanced CAP training implementation – the responsibility of clinical services, College Training Committees and local Directors of Advanced Training – similarly evades adequate evaluation. This diminution of governance has allowed a disconnect between international best practice, evidence-based training and real-world implementation to arrive at a major risk to trainees and consumers. Enhanced review and credentialing processes are required to ensure that ANZ trainees have access to international best-practice training.
Balancing generalist against subspecialist training
The mental health needs of children and adolescents are predominantly met by people other than CAPs. This includes general psychiatrists. Conversely, many CAPs provide care to adult patients. In part, this emerges from embedding subspeciality training within general psychiatry training, an arrangement that reflects the emphasis in ANZ on producing general psychiatrists. This structure differs from many nations where CAP and adult psychiatry are separate medical specialities. In the United Kingdom, a hybrid model shares ANZ’s joint initial 3-year basic psychiatry training before a 3-year separate specialist advanced training in CAP leading to separate specialist recognition (Table 1).
Global benchmarks of child and adolescent psychiatry training.
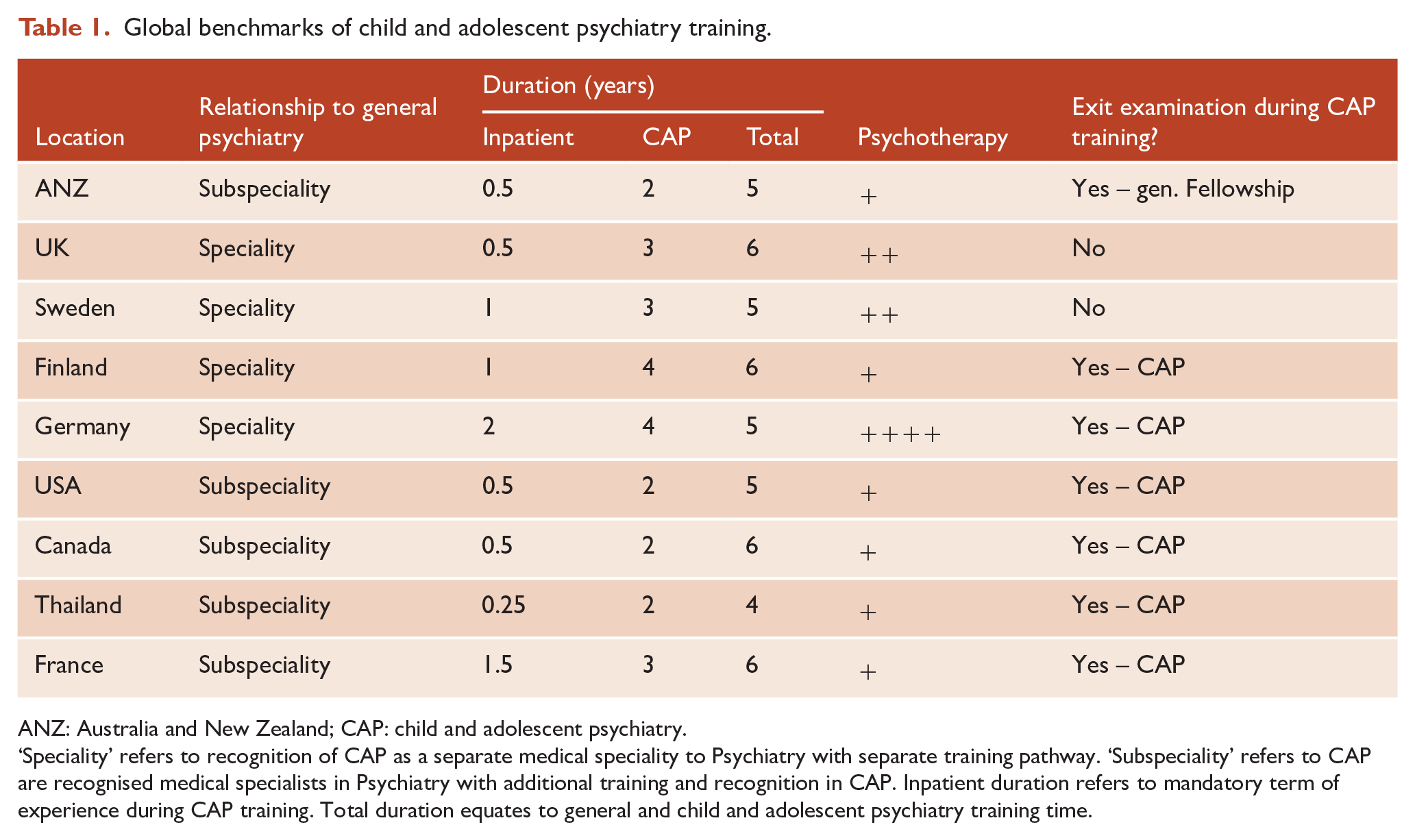
ANZ: Australia and New Zealand; CAP: child and adolescent psychiatry.
‘Speciality’ refers to recognition of CAP as a separate medical speciality to Psychiatry with separate training pathway. ‘Subspeciality’ refers to CAP are recognised medical specialists in Psychiatry with additional training and recognition in CAP. Inpatient duration refers to mandatory term of experience during CAP training. Total duration equates to general and child and adolescent psychiatry training time.
Embedding subspeciality training within general psychiatry training requires a balancing of the community need for a general psychiatry workforce with competencies in CAP, against the development of a specialist CAP workforce. On one hand, the College ensures that all psychiatrists gain CAP training experience. On the other hand, the College also supports even greater subspecialisation through dual Advanced Certificate training in CAP combined with consultation-liaison, forensic or addiction subspecialities. Considering the diversity of our community and psychiatric profession, finding a necessary balance between a general versus subspeciality psychiatric workforce is challenging.
Clinical competence requires training time and a broad range of educational and training experiences. The balance between generalist and subspecialisation requirements has major implications for subspecialist CAP training, particularly the duration of subspecialist child and adolescent training. The European recommended minimum standard for CAP training is 3 years duration, in addition to general psychiatry training (European Union of Medical Specialists (UEMS), 2014; Table 1). An argument could be made to increase CAP subspeciality training time in ANZ, either by increasing total training time from 5 to 6 years or by reducing time in general psychiatry training from 3 to 2 years.
The overlap in training of, and service provision by, general and subspecialist psychiatrists is paralleled by that of emerging subspeciality areas of practice for youth psychiatrists and perinatal and infant psychiatrists (Figure 3). If the College endorses Faculty status and subspeciality training for these groups, then the overlapping populations, concepts and professional roles will need distillation (Figure 3) (Macmillan et al., 2021). With creative collaboration at developmental junctures, such an advance would enable subspecialities to learn from each other and provide an integrated clinical system for children and young people and their families. Neglect of this collaborative opportunity will invite training and practice silos in addition to diminished competencies at developmental transition points. An increasing number of Child and Adolescent Mental Health Services (CAMHS) and training programmes in Australia have indeed already shifted into Child and Youth Mental Health Services (CYMHS) by including young adult patients (18–24 years), though this is not the case in New Zealand. CYMHS and CAMHS have also expanded to encompass infant mental health services. The full impact of these clinical service system changes on CAP training is yet to be evaluated.
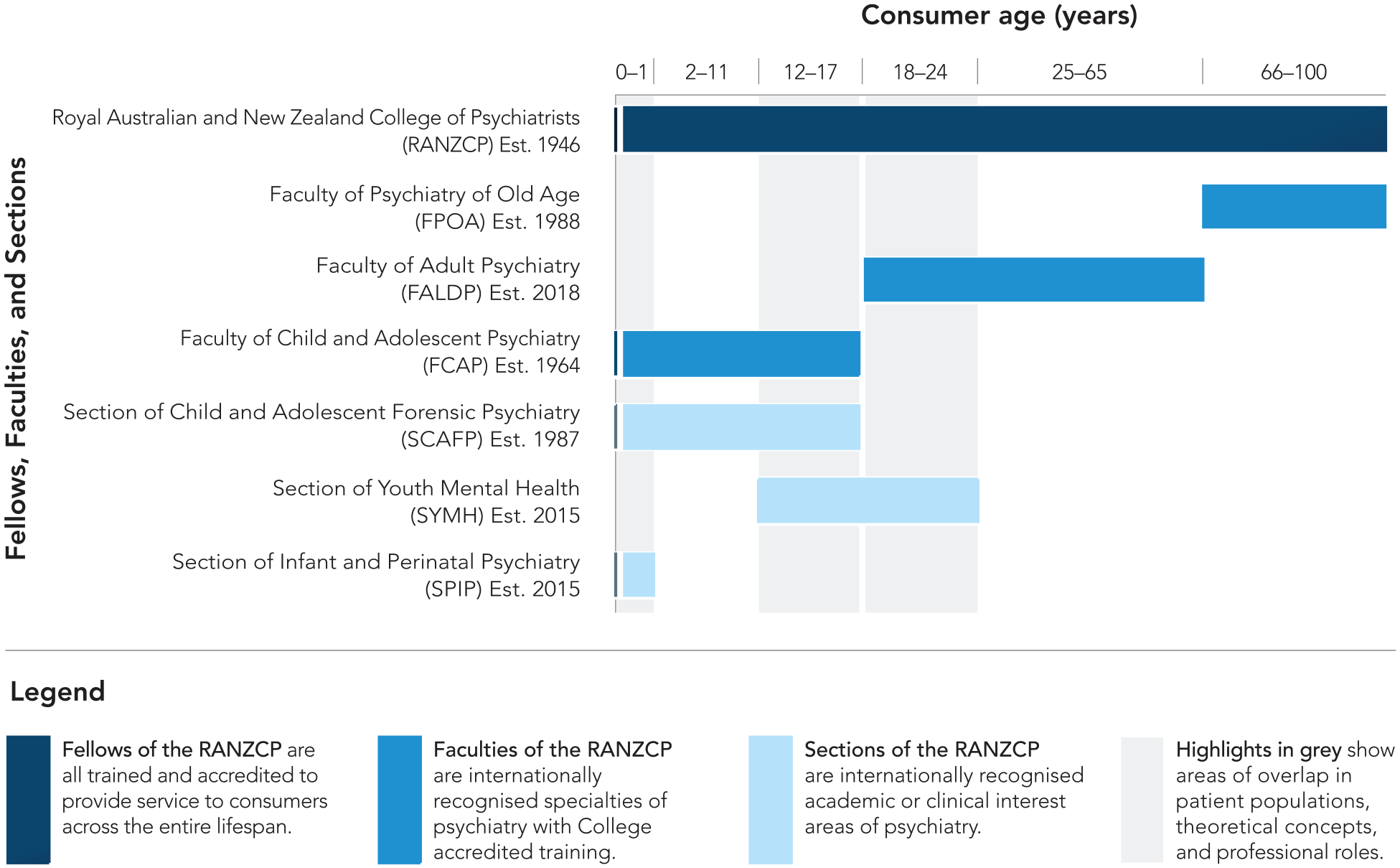
Developmental divisions of psychiatrists in Australia and New Zealand.
A peculiar challenge for ANZ trainees is the position of general psychiatry Fellowship summative requirements – ‘exit’ exams – within subspeciality CAP training. These demanding hurdles, some with a pass rate less than 50%, appear to interfere with subspeciality competency acquisition and deter prospective trainees. As was the case in ANZ before 2012, international programmes requiring general psychiatry exams conduct them prior to, or early after, commencing subspeciality training (Table 1). Some countries do have CAP exit exams and although the European Union of Medical Specialists (UEMS) is exploring a standardised CAP exam, this is not the case in ANZ.
Training content: psychotherapy and education courses
The CAP curriculum in ANZ is consistent with programmes internationally. However, one contentious element is psychotherapy training, critiqued by some as inadequate and by others as excessive. Many CAPs in private practice in Australia deliver psychotherapy, something uncommon in New Zealand. A range of psychotherapy training experiences across age-groups and modalities (e.g. dynamic, structured and dyadic/family) are mandated (RANZCP, 2020). However, there are variable levels of training and expertise required internationally. The European guidelines provide benchmarking for psychotherapy training in CAP programmes (UEMS, 2014). Perhaps, at best, our current training imbues a general understanding of various psychotherapies, their indications and limitations, allowing CAPs to function as clinical leaders. We should also consider how training dovetails with continuing professional development and greater competence in psychotherapy might be developed after graduation.
Internationally, all known subspeciality CAP training programmes use a formal education course (FEC). The structure and nature of FECs in ANZ are broadly informed, but not monitored, by a College syllabus, and vary greatly. Larger training programmes typically provide structured courses relative to the more flexible arrangements of smaller programmes. The emergence of web-based training facilitates accessible education in regional areas. However, face-to-face courses have united trainees and facilitated relationships with senior colleagues to promote collegiality and professional identity (Chandran et al., 2019). The benefits of both modalities will become clearer with experience.
Training in academic CAP
Academic CAP output from ANZ compares well internationally (Scott et al., 2018; Werry et al., 1991). To continue this, we must recruit and support graduating CAPs into academic careers (Thabrew et al., 2017). Academic CAPs are our eyes to a future that is uncertain and requires adaptability and innovation. Trainees can spend 12 of their total 24 months of CAP training in research. However, the low uptake of this option reflects limitations of funding, along with the challenge of addressing the requisite training experiences in the remaining year. Current training structures including the FEC and College-wide Scholarly Project thesis could be leveraged to provide greater exposure to academic CAP. Internationally, many FECs are formally delivered or supported by university departments. Developing similar arrangements in ANZ could enhance FECs, general CAP academic literacy and facilitate academic career pathways.
Conclusion and recommendations
Subspeciality CAP training in ANZ has many strengths. The challenges we identify include the evolving service design, training experiences dominated by high acuity presentations and impact of generalist examinations on subspecialist training. The diminution of College governance and accreditation processes has left the impact of these factors relatively unaddressed. We therefore recommend that the College, including the Faculty of CAP, undertake the following initiatives relative to subspeciality CAP training:
A review of the impact of the 2012 Fellowship programme.
Enhance the integration with university divisions of psychiatry.
Develop formal processes to ensure that curriculum design undergoes cyclical peer review and international benchmarking.
Strengthen training oversight and accreditation procedures for implementation in clinical services.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.