
Abstract
The impact upon child and adolescent refugees who have experienced organized violence or war has been subject of discussion in recent years. Several studies have investigated the psychological sequelae of traumatic war experiences of refugees [1]. Post-traumatic, depressive and anxiety symptoms as well as psychosomatic complaints, have been reported most frequently [2–6]. Investigations in groups of children from Bosnia revealed an additive effect of children's amount and type of war experiences on trauma reactions, but psychological and behavioural maladjustment was associated with both violent and non-violent acts of war [2], [7]. Furthermore, the capacity for children to cope with the atrocities of war are related to parental well-being especially maternal mental health [8] and adverse life experiences in the postwar period. Studies of coping and resilience among child refugees have demonstrated the consequences of continued stress in the context of their current life situation (e.g. cultural differences, residing in a refugee accommodation, physical health problems) [1]. Hodes [9] described that different studies concerning child refugees from South-East Asia and former Yugoslavia living mainly in the US indicate that severe psychiatric disorder is present within 40–50% of the examined children. The need for developing appropriate and effective psychosocial treatment programs for these children and adolescents as well as for adults has been repeatedly expressed [5], [10], but until now empirically tested interventions are sparse [1].
Single case reports indicate that a combination of social, educational and therapeutic interventions is important for the treatment of refugee children, as well as combining individual and group sessions [11]. Goenjian et al. [12] offered a brief trauma and grief focusing psychotherapy to adolescents who had been exposed to the 1988 earthquake in Armenia. A follow-up investigation 3 years later found significant improvement in post-traumatic symptoms in treated subjects compared with significant worsening in the control group, the latter also showed significantly worsened depressive symptoms while adolescents given psychotherapy showed no change in severity of depressive symptoms. In a pilot study Snodgrass et al. [13] introduced a 3 month stress intervention model in the form of a university course to eight Vietnamese refugees living in the US (mean age 19.3 years). Weekly sessions included information, relaxation and cognitive techniques (e.g. thought stopping) as well as role-modelling. A significant reduction of post-traumatic stress symptoms was found in the therapy group but not in the control group. Furthermore, symptom change was found in improved sleep, ability to relax when thinking of traumatic events, and improvement in decision making. Dybdahl [14] offered a psychosocial intervention program and basic medical care to mothers in war-torn Bosnia and Herzegovina and evaluated the effects on their children (mean age 5.5 years), in comparison to a control group, who received medical care only. The program consisted of weekly group meetings for 5 months lead by specially trained preschool teachers, focusing on promoting good mother–child interactions and coping with problems, as well as psychoeducation about trauma and trauma reactions. Results indicate positive effects of the intervention on the children in various areas such as happiness, cognitive performance, conduct problems and weight gain, though most effects (excluding the weight gain), did not reach statistical significance.
Other therapy programs with war traumatized chil-dren/refugees have not been evaluated with standardized instruments but are still a valid source of gathering information about possible applicable techniques. Mainly creative techniques were used in a primary mental health program with Guatemalan refugee children in Mexico whose parents had to flee political persecution. Techniques included painting, sociodrama and role playing as well as collectively created stories around topics of exile and return or related to everyday life in the camps [15]. Positive effects on the children where reported. Shy children became more active and social interactions between children improved. A program with war traumatized children in Bosnia utilized structured group sessions with topics such as trust, war, future, and farewell [16]. In addition to group discussions the following techniques were applied: drawing, communication and movement games, psychomotoric activities, relaxation, verbalizing, fantasy journeys. Psychological symptoms of depression and anxiety, apathy and aggression were diminished, children gained more self-confidence, initiative and joy and to some extent conflict was reduced and school performance improved. The authors of the last three mentioned studies emphasize the training of local personnel such as teachers to maximize the availability of psychosocial programs in war-torn countries and refugee camps with limited personal and financial resources.
Despite the above mentioned programs there is still a paucity of explorative outcome studies in resourceorientated psychosocial intervention programs for refugees among school children and adolescents. The development of our program was aimed at addressing the general need of child refugees for psychosocial support, in the sense of a resource-orientated intervention that can be carried out within a limited period of time and could be helpful despite diversity of psychosocial problems and cultural backgrounds. Next to the effects of war on the well-being of the children their current life situation (e.g. residing in a refugee accommodation) also was considered. The combination of different treatment modalities including an integration of parental figures within the program has been designed to account for age, intellectual and developmental diversities of the participants. The program was established to provide basic help in alleviating emotional distress and improving psychosocial functioning. Therefore the present study had the following major goals:
To examine the relationship between the number of traumatic events and the degree of the psychological disturbances. To implement and evaluate the effectiveness of a newly designed short-term psychosocial treatment program among children and adolescents.
It was hypothesized that the intervention has positive effects on the participants with regard to the reduction of emotional distress and an improvement of the degree in overall psychosocial functioning.
Method
Procedure and subjects
The present investigation is a prospective experimental study with a pre- and post-test design without the use of a control group. Participants were recruited from a refugee accommodation in Germany which hosted refugees who had fled the Kosovo-conflict in 1998/99. All families with children in the age from 10 to 18 years were informed about the study in advance during a formal meeting in the refugee accommodation. After a complete explanation of the study was given to the adolescents and their caretakers, written informed consent was obtained from both. All procedures were approved by the Ethics Committee of the University Clinic. Evaluations took place in the nearby University Clinic for Child and Adolescent Psychiatry prior to treatment and following the intervention. The treatment program itself was organized in the refugee accommodation area during the 12 weeks from May to July 2000. Diagnostic and evaluation sessions were lead by a child psychiatrist. Therapeutic sessions were conducted by a specially trained medical student. A translator of Kosovo-Albanian ethnicity was present in every session.
Program description
The program was carried out over a duration of 12 weeks. Participants took part in two information sessions, two diagnostic/evaluation sessions, six group sessions, two to four individual sessions and one family session. One session was also held with each child's parents. Core aspects in the presented model are: the combination of individual, family, and group sessions; a trauma- and grief focusing therapy; verbalizing; relaxation techniques; the use of creative techniques such as painting, playing, acting, and fantasy journeys (guided imagery); group discussions, and psychoeducation about trauma and trauma reactions (focused on parents). Apart from the traumatic experiences and their consequences, current problems were addressed concerning life as a refugee, family, future and return. The structured group sessions in which all participants took part together formed a core element of the therapy. Every session had a topic, for example ‘Grief and sorrow about lost ones’, ‘My way between the cultures’, ‘The future: dreams and realities’. The sessions consisted of two parts: During the first part various activities and discussions addressing the topic took place, whereas the second part offered a time of calmness and relaxation: After a body-relaxation-preparation a fantasy story related to the topic of the day was read out to them (both in German and their mother tongue). The duration of these group sessions varied from two to three hours. More detailed information about structure and content of the various sessions is given in the manual to the program [17].
Instruments
Participants were assessed by means of structured clinical interviews conducted by the child psychiatrist (supervising physician) using standardized questionnaires to evaluate post-traumatic symptomatology, depression and anxiety, and overall psychosocial functioning. Psychiatric diagnoses according to the DSM-IV [18] were assessed both before and after the intervention with the German version [19] of the semistructured diagnostic interview of the Schedule for Affective Disorders and Schizophrenia for School-Age Children – Present and Lifetime Version (K-SADS-PL) [20], [21].
Traumatic experiences and psychological symptoms were assessed prior to the intervention. A Kosovo-Albanian translator was present during the interviews. All written questionnaires have been translated into Albanian. Traumatic experiences and post-traumatic symptomatology of the participants have been assessed using the Harvard Trauma Questionnaire (HTQ) [22]. This self-report instrument has been applied in a cross-cultural context and evaluations have demonstrated good psychometric properties [22–24]. This 16-item checklist collect different traumatic experiences with four answer categories: (i) experienced; (ii) witnessed; (iii) heard about; and (iv) none. The total trauma score (HTQ Trauma Index) is the sum of all answers given in the categories 1–3, multiple answers are possible. Post-traumatic symptomatology (intrusion, avoidance, arousal) and symptoms arising in relation to traumatic experiences (shame, survivor guilt, feelings of hostility towards oneself) was measured by a 30-item-checklist with four answering categories from ‘Not at all’ (score = 1) to ‘Extreme’ (score = 4). The symptom score of the HTQ post-traumatic stress disorder (HTQ PTSD) is the sum of scores to all answered items in each area of symptomatology, divided by the number of answered items.
Symptoms of depression and anxiety were assessed by the parent version of the Diagnostic System for Psychological Disorders (DISYPS-KJ), a diagnostic system for mental disorders in childhood and adolescence developed by Döpfner and Lehmkuhl [25]. Symptoms of depression are assessed on a 29-item-checklist; symptoms of anxiety on a 31-item-checklist. Both correspond to DSM-IV criteria. Four answer categories range from ‘Not at all’ (score = 0) to ‘Extremely’ (score = 3). The mean symptom score can be interpreted as following: 0.0–0.5 not at all; 0.5–1.5 minor; 1.5–2.5 moderate; 2.5–3.0 major.
The German version [26] of the Children's Global Assessment Scale (CGAS) [27] was used to assess the overall psychosocial functioning of the child prior to traumatization, directly after the traumatization, prior to and after the intervention has been completed. An expert rating was made by the supervising physician in child psychiatry using information gathered from the parents and children. To overcome the difficulty that the physician was not blind to the information that the investigated children had been in treatment it has been made an effort to rely on the statements of the parents and the children during the interview and not on the personal impression of the physician. Clinical studies have reported substantial interrater reliabilities and retest stability of the CGAS [28], [29]. The child is rated on a scale from 1 to 100, with 100 being the maximum in global psychological functioning. A cut-off score of 70 generally represents the critical point between normality and need for therapeutic treatment. Being a responder or non-responder to the therapeutic intervention was defined by an increase of at least 10 points of the CGAS score.
Statistical analysis
Data analyses consisted of descriptive statistics (mean and standard deviations) and inferential procedures to examine the change in symptomatology and associations between the number of traumatic experiences and symptomatology. Change of symptomatology for instruments with two measurements (pre – post) was assessed with t-tests for paired samples, associations were assessed with Pearson correlations. If the normality assumption was violated (checked with the Kolmogorov-Smirnoff-Test), the non-parametric equivalents were used (Wilcoxon matched pairs signed-ranks test and Spearman rankcorrelation). For more than two measures in time (CGAS) a random effect regression was calculated to assess changes. Calculations were done with the statistic software package Stata 8.
Results
Out of 13 potential participants 10 young refugees agreed to participate in the treatment program. Of the three non-participants two adolescents declined and in one case the parents refused the participation of their child. The participating 10 young refugees aged between 10 and 16 years (mean = 13.3, SD = 2.0) at pretreatment evaluation, residing with their families in a refugee accommodation. Their average length of stay in Germany was 12.2 (SD = 3.2) months at the time of the pretreatment evaluation. The sample consisted of 3 girls and 6 boys of Kosovo-Albanian ethnicity, one girl was Roma (European gypsy). All children taking part completed the intervention program and were all included in the statistical analysis. Despite the heterogenity of age and clinical symptomatology of the participating adolescents the manualized program could be carried out without difficulties. Even though the parents of two patients (case 5 and 6) were less compliant during the psychiatric evaluations their children were adaequateley engaged in the program.
Table 1 summarizes the ages, gender, trauma severity scores, psychiatric diagnoses and symptomatology for all individual subjects at baseline and post-treatment evaluation. Results of the HTQ demonstrated that participants varied concerning the extent of traumatic experiences. The total trauma score (HTQ Trauma Index) was in a range between 5 and 42 (mean = 21.50, SD = 10.91). The different types of traumatic experiences were more homogeneous: 80% of the children experienced lack of shelter, combat, and other frightening situations related to war and persecution, whereas the murder of family members was reported less frequently (20%). None of the children had been tortured, seriously injured or raped. HTQ trauma severity index score correlated significantly with the degree of self-reported (HTQ) PTSD symptoms (r = 0.897, p = 0.0004), depressive symptomatology (r = 0.686, p = 0.029), and degree of overall psychosocial functioning (r = −0.66, p = 0.038). Initially assessed anxiety symptoms were not significantly correlated with the trauma index score (r = 0.56, p = 0.093).
Age, gender, traumatic experiences, psychiatric syndromes and symptoms of adolescent Kosovo-Albanian refugees (n = 10)
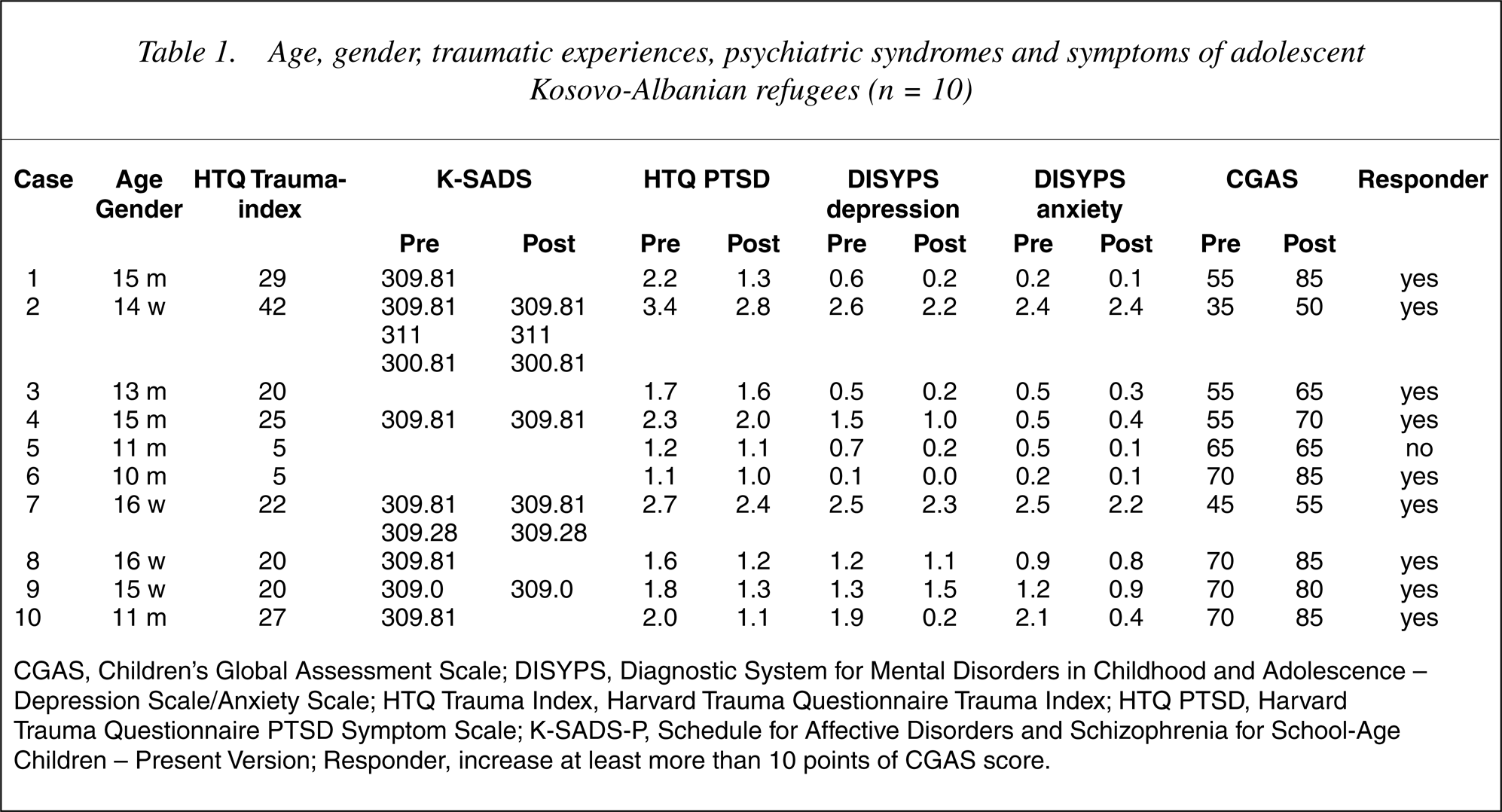
CGAS, Children's Global Assessment Scale; DISYPS, Diagnostic System for Mental Disorders in Childhood and Adolescence – Depression Scale/Anxiety Scale; HTQ Trauma Index, Harvard Trauma Questionnaire Trauma Index; HTQ PTSD, Harvard Trauma Questionnaire PTSD Symptom Scale; K-SADS-P, Schedule for Affective Disorders and Schizophrenia for School-Age Children – Present Version; Responder, increase at least more than 10 points of CGAS score.
At time of pretreatment evaluation seven of the 10 children fulfilled the diagnostic criteria for a psychiatric disorder according to DSM-IV (see Table 1): One for adjustment disorder with depressed mood (309.0); four for PTSD (309.81); one for PTSD, depressive disorder NOS (311), and undifferentiated somatoform disorder (300.81); and one for PTSD and adjustment disorder with mixed anxiety and depressed mood (309.28). At follow-up, the PTSD diagnosis persisted in three of the six children with PTSD at baseline. One child, who did have an adjustment disorder with depressed mood at baseline, met diagnostic criteria at follow-up again for this disorder. The degree of post-traumatic, depressive and anxiety symptoms at baseline varied from none to moderate between participants but revealed that some children suffered from emotional distress. After the intervention mean PTSD symptom severity score declined significantly (t-test, p = 0.018), as well as the symptom scores of depression (Wilcoxon, p = 0.014) and anxiety (Wilcoxon, p = 0.006). With regard to the CGAS score at baseline and at follow-up, 9 of 10 subjects showed an increase of at least 10 points indicating a substantial gain in psychosocial functioning.
The course of the overall psychosocial functioning from premorbid to post-treatment situation as assessed by the CGAS score is summarized in Table 2. During the period before concluding the pretreatment evaluations no significant change of the CGAS score was found (p = 0.258). After the intervention a substantial increase of the CGAS score was found (p < 0.001), but the post-treatment score was still lower than the pretrauma CGAS score (p < 0.001). The CGAS score prior to traumatization correlated significantly with the improvement in psychological functioning during the intervention (r = 0.673, p = 0.033).
Course of the global psychosocial functioning assessed with the Child Global Assessment Scale (CGAS)†
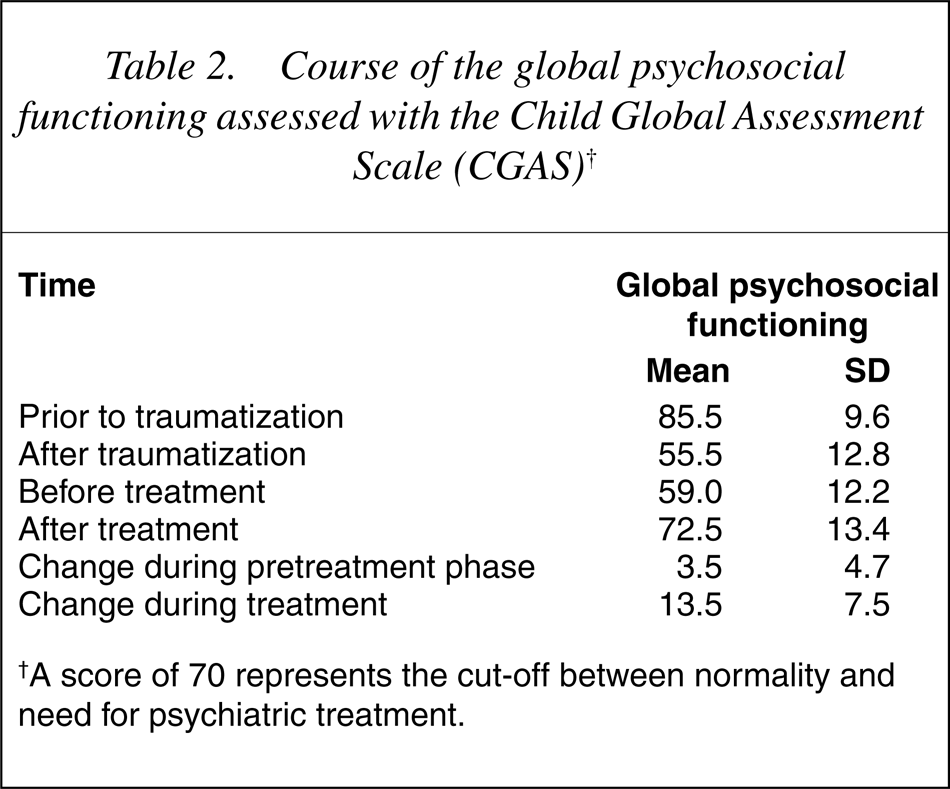
†A score of 70 represents the cut-off between normality and need for psychiatric treatment.
Discussion
Results revealed that all participants had suffered from traumatizing experiences related to war and persecution, but that the degree of traumatization varied between the children. The number of traumatic experiences as assessed by the HTQ were highly associated with the severity of post-traumatic and depressive symptoms and additionally with the impairment of global psychosocial functioning after traumatization. These findings of a relationship between the extent of traumatic experiences and psychological distress reflect the findings of earlier studies on this topic [2], [7]. The degree of anxiety symptoms were not significantly related with the number of traumatizing experiences. Our findings of a minor to moderate level of depression and anxiety in most of the children are compatible with former studies [2], [8]. The level of 70% of psychiatric disorders in our sample lies between that described by Hodes [9] within such populations (40–50%), and those documented in the study of Goldstein et al. [30], who found a prevalence rate of 94% of PTSD within war traumatized children from Bosnia. These findings strongly document the need for developing appropriate and effective psychosocial treatment programs for child and adolescent refugees, especially due to the fact that the present study included refugee children from a refugee accommodation without a preselection of psychological symptomatology.
Even though no control group has been used an effect could be attributed to the treatment program since no change of the degree of psychosocial functioning has been observed over the 12-month period before starting treatment. Parents and children both reported that the children's status had improved after the intervention. Single case analyses of the participants indicate that these improvements concerned various areas of psychological well-being such as improved sleep, ability to relax, handling of traumatic memories, and social interactions within the refugee community, and with family and friends. Children reported that the feeling of togetherness and of being cared for within the group was very important for their well-being. This setting seems to meet the children's request of working on the traumatic experiences privately during the individual sessions, but additionally being to be able to share experiences and grief with others and the family thus getting to know other positions in dealing with these experiences. These findings stress Yule's [31] statement about the treatment of war affected children that ‘group approaches seem to be very therapeutic for many children but not all problems can be solved in the group (p. 701).’ The fantasy journeys together with the relaxation exercises were greatly appreciated by the children. They reported that their sleep improved on the days they listened to these stories and they enjoyed to be able to escape into worlds other than the harsh reality of the refugee accommodation.
The results of the study indicate that basic help was provided and that as hypothesized the intervention had positive effects on the participants with regard to reduction of the emotional distress and improvement in the degree of global psychological functioning. It has to be emphasized that this intervention cannot replace a professional psychotherapy for extremely traumatized and multimorbid children, such as case 2 and 7 of the subjects in this study.
The absence of a control group is a weak point of the study, which limits the differentiation between treatment effects and spontaneous improvement over time. Because of the limited number of potential participants a control group could not be established. Another limitation of this study is that the psychiatrist conducting the CGAS assessment was not blind to the pretreatment psychiatric evaluation. This fact may have influenced the objectivity of the post-treatment assessment. Furthermore, both the small sample size and the fact that due to economic reasons the treatment program has been carried out by only one person make it difficult to generalize the findings. Therefore replications of this study are needed. It is not possible to distinguish how strong the treatment effect is related to the person leading the treatment or to the program itself. A follow-up could not be conducted due to the fact that 6 of the 10 children went back to their home country within a period of 6 weeks after cessation of the intervention.
Future studies will have to investigate whether the program can be taught to, and carried out by professionals from related professions (teachers, social workers) as demonstrated by Wintsch [16], to guarantee a broad and cost-effective applicability. Generalizability and longterm effects should also be a focus of future studies. The authors strongly recommend future research in this field, as child and adolescent refugees all over the world are in great need for appropriate psychosocial treatment addressing their requirements, but to date there is not enough evidence of which treatment programs are more effective both psychologically and economically.
Footnotes
Acknowledgements
We thank Tefik Ramadani for functioning as translator during the study. Financial support was provided by the Wilhelm Bitter Foundation and the Dieter Radaj Foundation, Germany.