
Abstract
People with schizophrenia have a shorter life expectancy compared to the general population and suffer from a variety of physical disorders including obesity, diabetes mellitus, hypertension and coronary heart disease [1–3]. The prevalence of overweight/obesity ranges between 40% and 62% in people with schizophrenia [4], and there are similar rates for bipolar disorder [5]. Obesity is associated with an increased risk for diabetes, hypertension and coronary heart disease beside other disorders such as cancer, osteoarthritis and gall bladder disease [6]. Metabolic syndrome (MetS) is a cluster of metabolic dysfunctions including central obesity, hypertension, glucose and lipid abnormalities. Those with the syndrome have a two- to threefold increase in cardiovascular mortality and a twofold increase in all-cause mortality [7]. Most studies reported prevalence rates of MetS in schizophrenia and bipolar disorder at around 40% [8–11]. This rate is twice the rate of occurrence in the general population [12].
Psychiatric rehabilitation is the application of medical, psychological, social, educational, and vocational measures for individuals with a mental disorder to support them to achieve their highest possible level of functional ability and quality of life. Good physical health is also a realistic goal for people with mental illness [13]. Maintenance of optimal physical health is an important component necessary for the patients to engage in the rehabilitation process and to achieve expected outcomes. Obesity and metabolic disorders occurring at high rates could hinder rehabilitation. Obesity has been strongly implicated in disability suffered by people with mental disorder [14] and in their quality of life [15]. It can have important effects on an individual's self-image, adjustment in the community, adherence to prescribed medication and ability to participate in rehabilitation process [2]. Metabolic disorders such as diabetes can add to the burden of disability and suffering of people with a psychiatric impairment. Diabetic symptoms and diabetic complications are associated with increased disability in mobility, self-care and higher functioning [16]. Depression and anxiety are commonly associated with obesity, diabetes and ischaemic heart disorder [17–19]. These comorbid disorders add to the disability of people with a psychosis and a metabolic disorder.
Consensus guidelines are now in place to screen and monitor for metabolic disorders in people on antipsychotic medications [3, 20]. These recommendations were incorporated into clinical practice in a psychiatric rehabilitation service. The findings of the clinical audit are reported and discussed in this paper.
Method
This report is based on an audit of clinical and laboratory assessments for obesity and MetS conducted in patients with a diagnosis of a psychotic disorder who were attending the Psychiatric Rehabilitation Service of Hunter New England Area Health Service, New South Wales, Australia. Patients were either in the hospital-based programme at Morisset hospital or in a community-based rehabilitation centres at Cardiff and Maitland. The number of patients in these centres at the time of study was 353 (91 patients in the hospital-based programme and 262 patients in the community-based programme). Only patients on an antipsychotic drug were targeted for evaluation. Three patients in the hospital and 26 patients in the community programme were not taking any antipsychotic drug. The size of the population selected for the clinical audit was 324.
Informed consent was not sought because the assessments were part of clinical management protocol at the service. All patients who could be examined by the authors and who could complete the laboratory tests were assessed. Patients not willing to undergo the physical or laboratory evaluation were not assessed. There was no bias towards selecting overweight or obese individuals for the audit. The authors or a clinical nurse measured patient height, weight, waist circumference and blood pressure. The venous blood sample was drawn after overnight fasting and processed in an accredited clinical laboratory. Information on demography, diagnosis, duration of illness and treatment was taken from the medical case records. Patients detected to have features of MetS were referred to their general practitioners for appropriate medical management. We followed up the referral to ensure that contact with the general practitioner occurred.
Approval was obtained from the Hunter New England Research Ethics Unit to publish this paper. Care was taken to prepare the manuscript in such a way that it did not identify any patient directly or indirectly and in accordance with the NSW Health Records and Information Privacy Act, 2002.
Results
Patient population
We had complete assessments of 221 patients at the time of this report. Seventy-eight patients were assessed at the inpatient rehabilitation unit and 143 at the community-based services. The duration of hospitalization exceeded 6 months for 83% of patients (65/78). A substantial number of patients (37/78, 47.4%) assessed were in the hospital for ≥2 years, mainly in the long-term clinical support and medium secure units of the hospital. There were 172 male (77.8%) and 49 female (22.2%) subjects. There was no significant difference in gender distribution between the hospital and community patients (male = 84.6% and 77.6% respectively). The mean age was 37.9 years (SD = 10.4). There was no significant difference in the mean age of the hospitalized patients (mean = 38.0 years, SD = 12.1) and those in the community (mean = 38.0 years, SD = 9.4). A majority of patients (129, 60%) were in the age range 30–50 years. Most patients (205, 93%) had a diagnosis of schizophrenia or schizoaffective disorder. Bipolar affective disorder was diagnosed in nine (4%) and other psychoses in seven (3%). Duration of illness of at least 5 years was a criterion for acceptance into the rehabilitation programme. Nearly two-thirds of patients had the psychosis for >10 years. First-generation antipsychotics (FGAs) were prescribed for 47 patients and second-generation antipsychotics (SGAs) for 203 patients; 29 patients (13% of the total) were on both classes of drugs. Haloperidol and zuclopenthixol decanoate were the most frequently used FGAs (36/47). The others received either long-acting injectable form of flupenthixol (n = 8) or chlorpromazine (n = 3). Clozapine was the most common SGA prescribed (127/221, 58%). Forty-five patients were receiving only clozapine. The other SGAs prescribed (alone or in combination with other drugs) and the number of patients receiving them was as follows: olanzapine, n = 26; quetiapine, n = 22; risperidone, n = 36;, amisulpride, n = 43; and aripiprazole, n = 3. Mood stabilizers (lithium and sodium valproate) were prescribed along with antipsychotic drugs to 70 patients (32%). Antidepressants were prescribed for 40 patients (18%). The information on the exact duration of treatment with each of the drugs was not available for the study.
Body mass index
The mean body mass index (BMI) was 32.2 (SD = 6.6). The mean BMI in female subjects (35.1, SD = 6.8) was significantly higher than in male subjects (31.4, SD = 6.3; t = 3.62, p < 0.01). It was below normal (≤18.5) in one patient (0.5%) and normal in 26 patients (12%). Sixty-four patients (29%) were overweight with BMI 25–29.9, and 130 (59%) were obese with BMI ≥ 30. Among the obese 27 (12% of the total) were extremely obese, with BMI ≥ 40. There was no significant difference in the proportion of people who were overweight/obese in the hospital (87.2%) and community (87.3%).
Metabolic syndrome
The mean value and gender differences in waist circumference, blood pressure, fasting level of glucose triglyceride and high-density lipoprotein (HDL) cholesterol is presented in Table 1. Female subjects had a significantly larger mean waist circumference and higher level of HDL cholesterol while male subjects had higher mean systolic blood pressure, glucose and triglyceride levels.
Metabolic syndrome criteria
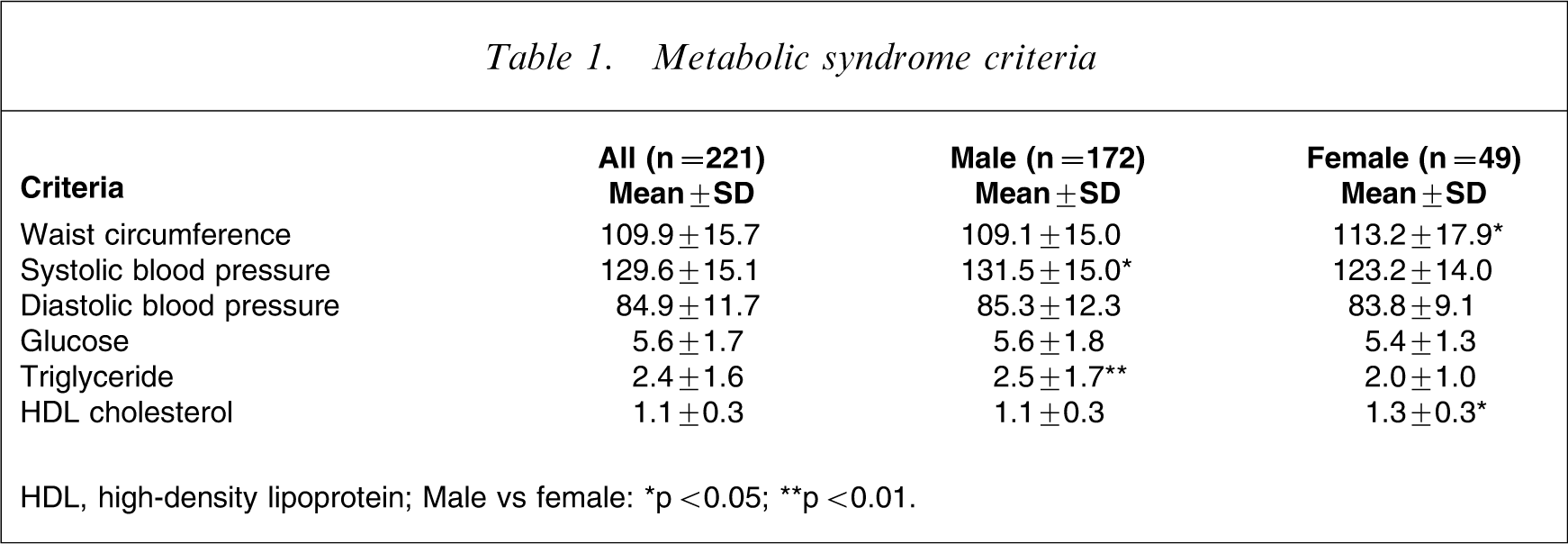
HDL, high-density lipoprotein.
Male vs female: ∗p < 0.05; ∗∗p < 0.01.
The International Diabetes Federation (IDF) definition of MetS [21] was adopted to diagnose MetS in the patient population. Applying this definition, 150 patients (67.9%) were diagnosed with MetS. The prevalence was 70.3% (121/172) among male and 59.2% among female subjects (29/49). This was not significant. There was no significant difference in the prevalence of MetS between hospitalized patients (54/78, 69.2%) and patients living in the community (96/143, 67.1%). Medical treatment history data available for 165 patients showed that 22 patients (13.3%) were on treatment for diabetes mellitus, 23 (13.9%) for hypertension and 15 (6.8%) on statin therapy for lipid abnormality at the time of the study.
Central obesity, as measured by waist circumference, was recorded in 156 patients (70.6%). This feature is a mandatory criterion for diagnosis of MetS using IDF criteria. Thirty-nine (17.6%) fulfilled at least one of the other four IDF criteria while 71.9% fulfilled at least two of them. In the total population studies only five patients (2%) did not have any feature of MetS. Based on available medical history, we found that 104 of 125 patients (83.2%) who fulfilled the blood pressure criterion of MetS were not on any treatment for hypertension. The percentage of patients not on medical treatment for an abnormal glucose was 63.9% (39/61) and for lipid abnormality, 81.7% (67/82). None of the patients was on any formal diet-monitoring programme or lifestyle change intervention aimed at weight control at the time of the study.
Table 2 shows the prevalence of MetS associated with the type of antipsychotic drug used at the time of study. The difference between types of drug was not significant although the highest prevalence was in patients on more than one SGA (78.8%).
Type of antipsychotic drug and prevalence of metabolic syndrome
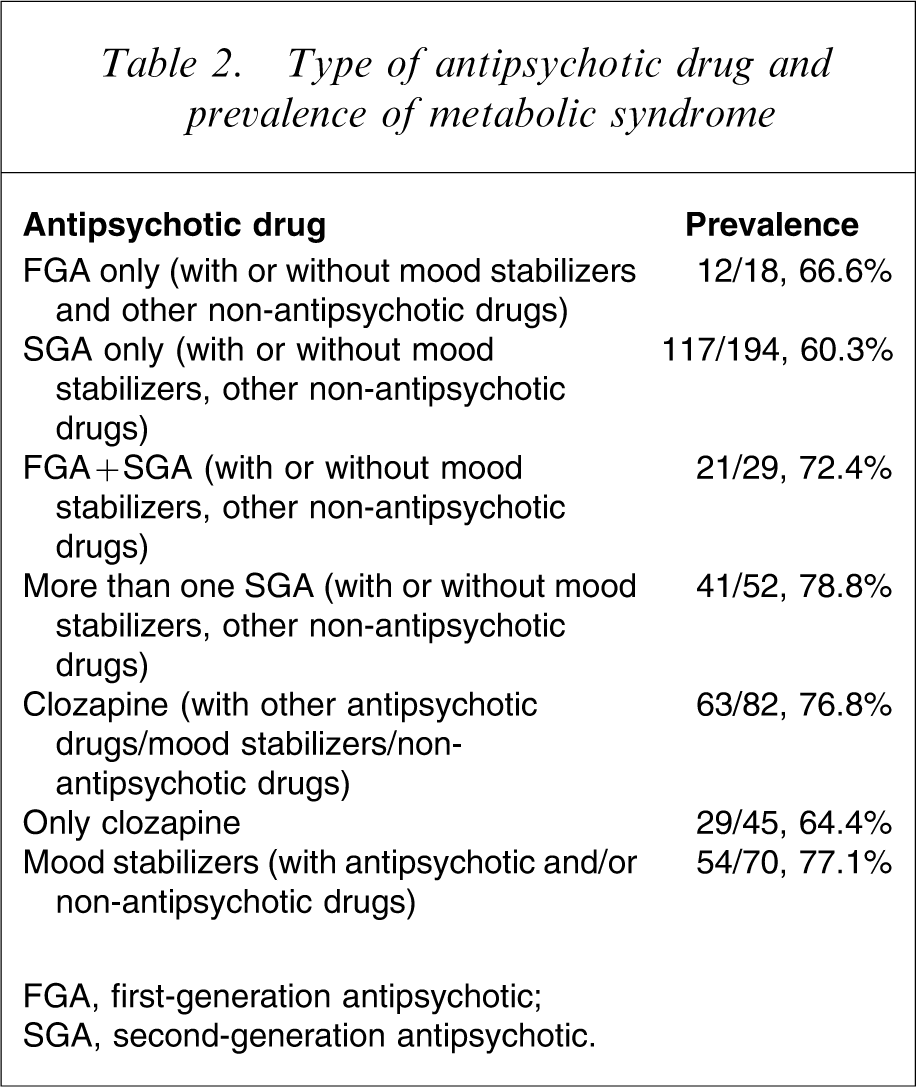
FGA, first-generation antipsychotic; SGA, second-generation antipsychotic.
Discussion
Study population
We needed to consider the nature of the patient population in interpretation of our findings. Most of them had a diagnosis of schizophrenia or schizoaffective disorder. A large number were on antipsychotic drug treatment for >5 years. While 91% of patients were currently taking SGAs, more than half were on clozapine.
Prevalence of obesity and metabolic syndrome
The prevalence of overweight/obesity (88%) and MetS (68%) in the present study was higher than that commonly reported in the literature [4]. The present study group was made up of a significant number of hospitalized patients. We did not observe any significant difference in the prevalence of MetS between patients in the hospital and the community. Hence the present findings can be considered relevant to the majority of the Australian patient population with chronic psychosis who are in the community. However, the results could not be applied to the people in the acute or subacute phase of a psychotic disorder.
The rates of obesity and MetS observed in the present study were much higher than those recorded in the Australian general adult population. The prevalence of obesity (59%) in the present patient population was nearly threefold the rate (20.8%) reported among Australian adults [22]. Similarly, the prevalence of MetS among the present patients on antipsychotic medication was more than double the rate of 29.1% observed among Australian adults [23].
Clozapine was more frequently associated with obesity and MetS than other antipsychotic drugs [24, 25]. Antipsychotic polypharmacy was associated with higher rates of MetS and lipid markers of insulin resistance [26]. Some of the reasons for the high rates of obesity and MetS noted in the present study could be the frequent use of clozapine and polypharmacy in the form of more than one antipsychotic or a combination of mood stabilizer with an antipsychotic. However, it is difficult to comment on the relationship between emergence of obesity and MetS and use of any particular drug or class of drug in the present study because of the cross-sectional nature of data.
Diet preference and sedentary life style have often been implicated in the occurrence of MetS [27]. We did not collect information on the dietary intake and energy expenditure and hence were not in a position to comment on the relevance of these two factors to the high rates of obesity and MetS observed.
Management of metabolic syndrome
One of the significant observations made in the present study was the high rate of non-treatment of existing metabolic disorders in the population. We believe that the main reason was non-detection. There was also a worrying possibility that excess weight gain and metabolic disorders were detected at a previous assessment but not followed up. We did not explore these issues in the present study. Studies have shown that there was a high likelihood that metabolic disorders were untreated in patients with schizophrenia [2, 28]. The National Health Priorities Area Action Council commissioned programmes to ensure that the physical health needs of those with specific mental illnesses such as schizophrenia are identified [3]. Treatment of obesity and metabolic disorders should be individualized and include ongoing monitoring, active engagement and education of patients and carers, therapeutic lifestyle change that include healthier food choices and engagement in increased physical activity, and active medical treatment for the metabolic disorders that go along with appropriate antipsychotic drug choice [6, 20, 29, 30].
Conclusion
A large proportion of patients with chronic severe mental disorders in a psychiatric rehabilitation programme suffered from metabolic disorders. These were often undetected and untreated. Detection, monitoring and appropriate treatment of obesity and metabolic disorders should be a component of an assertive care management programme to reduce morbidity and mortality and improve rehabilitation outcomes.