
Abstract
Keywords
Diagnostic stability is the degree to which diagnosis remains constant at subsequent patient assessments [1]. It is one of the five validating criteria suggested by Robins and Guze for verification of psychiatric syndromes [2]. Clinicians observe the patient's phenomenology over a period of time and integrate multiple sources of information before reaching a diagnosis. Following the introduction of DSM-III [3] and ICD-10 [4], operationalized criteria were introduced for making psychiatric diagnoses. However, the stability of these diagnoses is subject to various influences such as changes in the patient's clinical state, response to treatment, emergence of previously unrevealed relevant information or reinterpretation of gathered data [5].
Diagnostic stability is a problem, especially in patients with first-episode psychosis (FEP) due to fluctuating symptomatology, unclear mood symptoms and concomitant substance abuse [6]. This has led to many patients receiving non-specific diagnoses that change during the course of follow up [7]. Previous studies that examined diagnostic stability prospectively have found that schizophrenia is the most stable initial diagnosis (approx. 90.0%) followed by affective psychosis (80.0%), while other psychotic disorders such as schizophreniform disorder, schizoaffective disorder and psychotic disorder not otherwise specified (NOS) are the least stable initial diagnoses [5, 8, 9]. More recently, Schimmelmann et al. reported similar findings from a naturalistic study on diagnostic stability in FEP in which 59.1% of the patients had concomitant substance use that could have contributed to fluctuating symptomatology and inconsistency in diagnoses [10].
Other than two studies that were done in India [11] and Iran [12], all other studies in the extant literature on diagnostic stability of FEP have been done in the West. Sociocultural factors have been found to exert an influence on various aspects of psychopathology and management including symptom profile, diagnosis and outcome [13, 14].
In the present study we sought to determine the diagnostic stability in a population of FEP patients in Singapore. Sociodemographic and other factors were analysed to determine the factors that predicted a change in the diagnosis during the period of follow up.
Methods
The study sample consisted of 154 subjects who presented with FEP to the Early Psychosis Intervention Programme (EPIP) in Singapore. Singapore is an island state in South East Asia with a population of 3.4 million in which the majority of the population is Chinese (77.7%), followed by Malay (14.2%), Indian (7.2%), and others (1.2%). EPIP, a nationwide programme, was launched in 2001 at the Institute of Mental Health and Woodbridge Hospital, the only state psychiatric hospital in Singapore. These patients fulfilled the following criteria: (i) age between 18 and 40 years, (ii) first-episode psychotic disorder with no prior or minimal treatment (i.e. <1 week of antipsychotic medication); and (iii) no current history of substance abuse. The programme has an early component and a clinical component that provides psychiatric assessment and multidisciplinary management [15]. The 154 subjects (out of a cohort of 244 patients) included in the study consisted of patients with FEP consecutively accepted to EPIP and with an intact follow-up period of at least 2 years. Of the 90 patients (36.8%) who did not complete the 2 year follow up, four (4.4) died, 76 (84.4%) defaulted and 10 (11.2%) did not complete the required assessments.
The subjects were diagnosed using the Structural Clinical Interviews for DSM-IV (SCID–clinical version) at the first contact (baseline) and at the end of 2 years. Baseline clinical diagnoses were made by four experienced psychiatrists who were trained in the use of the SCID–clinical version. Training was conducted using the SCID diagnostic manual and training programme; interrater reliability was determined by 100% agreement on the diagnosis. Discharge clinical diagnoses at 24 months were based on repeat assessments, interview and various sources of information including consultations with the treatment team by the consultant psychiatrist, who was not blinded to the original diagnosis while performing the assessment. Duration of untreated psychosis (DUP) was operationalized as time in months between onset of psychotic symptoms (delusions, hallucinations, disorganized behaviour) and the time when a definitive diagnosis and treatment were established. Patients and the primary caregivers were interviewed by two of the investigators and asked to date the onset of psychotic symptoms and the DUP was estimated after combining information from the interviews and case records. In most cases, there was consensus among the patients and the primary caregivers as to the time of onset of psychotic symptoms, but in cases in which there was disagreement we favoured the patient's report of onset of symptoms over that of the caregivers.
Information (i.e. sociodemographic data, assessment with rating scales at baseline, during treatment and at 2 years) was recorded in standardized case notes, and extracted and stored in an electronic database routinely. As part of their routine assessment, the patients in the programme were assessed with the Positive and Negative Syndrome Scale (PANSS) [16] and Global Assessment of Functioning Scale (GAF) [17]. Number of hospitalizations and days of hospitalization were retrieved from the hospital inpatient database. Stability was determined as the consistency between diagnoses at the time of first contact and at 2 year follow up.
Data analysis
Subjects were grouped into the following diagnostic categories: affective psychosis (bipolar and major depressive disorders with psychotic symptoms), schizophrenia spectrum disorders (schizophrenia, schizophreniform disorder and schizoaffective disorder) and other non-affective psychosis (delusional disorder, psychosis NOS and brief psychotic disorder). Two measures of stability were determined for each diagnosis. The first was ‘prospective consistency’, which is the proportion of individuals in a category at initial assessment who retained the same diagnosis at the end of 2 years; this would correspond to the positive predictive value. The second measure, ‘retrospective consistency’, was the proportion of individuals in a 24 month category who previously received the same diagnosis (conceptually similar to sensitivity) [5].
Sociodemographic and clinical data were compared between the stable and unstable groups. Statistical analysis was carried out using SPSS for Windows, version 10.1 (SPSS, Chicago, IL, USA). Standard descriptive statistics were used to analyse the characteristics of subjects. χ 2 test and Kruskall–Wallis test were used to test for significant differences between groups. A stepwise logistic regression was performed to assess predictors of shift.
Results
The 154 subjects who completed the 2 year follow up, were predominantly Chinese (79.9%), single (71%) and had at least secondary level education (82%). The age of the subjects ranged from 18 to 41 years with a mean±SD of 28.4±6.6 years. Both genders were well represented with 51% being male, and the majority (97.4%) were living with family or friends at the point of entry. The mean±SD DUP was 22.4±35.3 months, the median DUP was 10.5 months. The baseline mean±SD PANSS score was 64.0±16.3 and the mean±SD GAF score was 41.1±15.7.
There were no differences in gender, age, or age of onset of illness between those who completed the 2 year assessment and those who did not. Of those 90 patients who did not have a 2 year assessment, 75% had a schizophrenia spectrum disorder diagnosis at the initial assessment, 7.5% a diagnosis of affective psychosis and 17.5% were suffering from other psychosis.
The overall consistency was 57.1%. The prospective consistency for schizophrenia was 87%, 12% for schizophreniform disorder, 55% for affective psychosis and 31% for brief psychotic disorder (the four most prevalent diagnoses at baseline). The retrospective consistency for schizophrenia was 63.2%, 40% for schizophreniform disorder, 57.1% for brief psychosis and 42.8% for affective psychosis (Table 1).
Cross-tabulation of initial and 24 month diagnosis in EPIP subjects
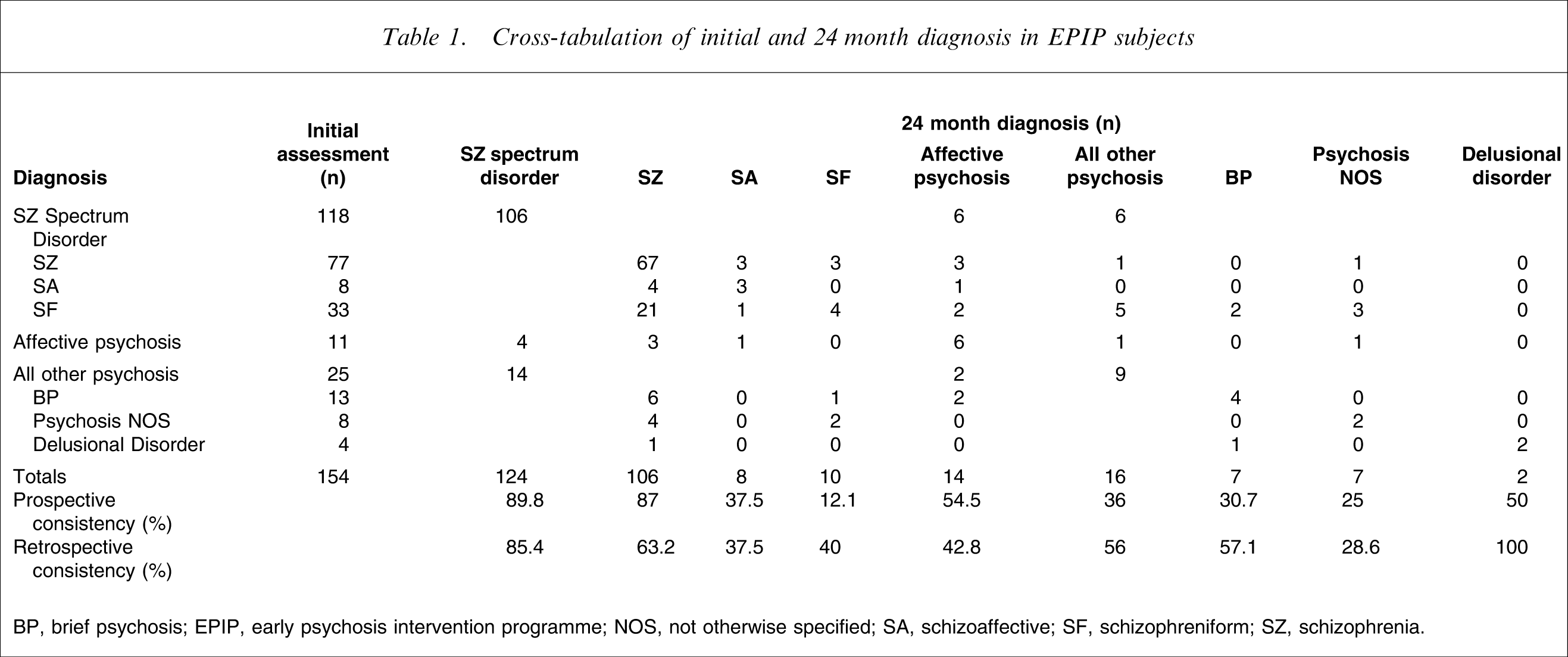
BP, brief psychosis; EPIP, early psychosis intervention programme; NOS, not otherwise specified; SA, schizoaffective; SF, schizophreniform; SZ, schizophrenia
One hundred and six patients (90%) received a schizophrenia spectrum disorder diagnosis at the initial assessment as well as at the end of the 2 year follow-up period. This represents 77% of the patients seen initially and 81% of the patients seen at 2 years with a diagnosis of schizophrenia spectrum disorder. The shift into schizophrenia spectrum disorder was the most frequent diagnostic change (n = 18). The initial diagnoses of these patients were brief psychosis (n = 7), psychosis NOS (n = 6), affective psychosis (n = 4) and delusion disorder (n = 1).
There were no significant differences between the stable and unstable diagnostic groups (Table 2) with regard to sociodemographic characteristics. Subjects in the stable schizophrenia spectrum disorder group had the longest length of hospitalization, and the groups differed significantly in terms of hospitalization days. There were no significant differences in the PANSS score or the GAF total score between the groups at baseline or at 2 years, but the GAF disability scores at 2 years were significantly different among the groups (p = 0.05, Kruskall Wallis test), those with schizophrenia spectrum disorder had the lowest GAF disability scores, while those with stable other psychosis had the highest scores at 2 year follow up.
Subject sociodemographic and clinical characteristics by diagnostic group (mean±SD)
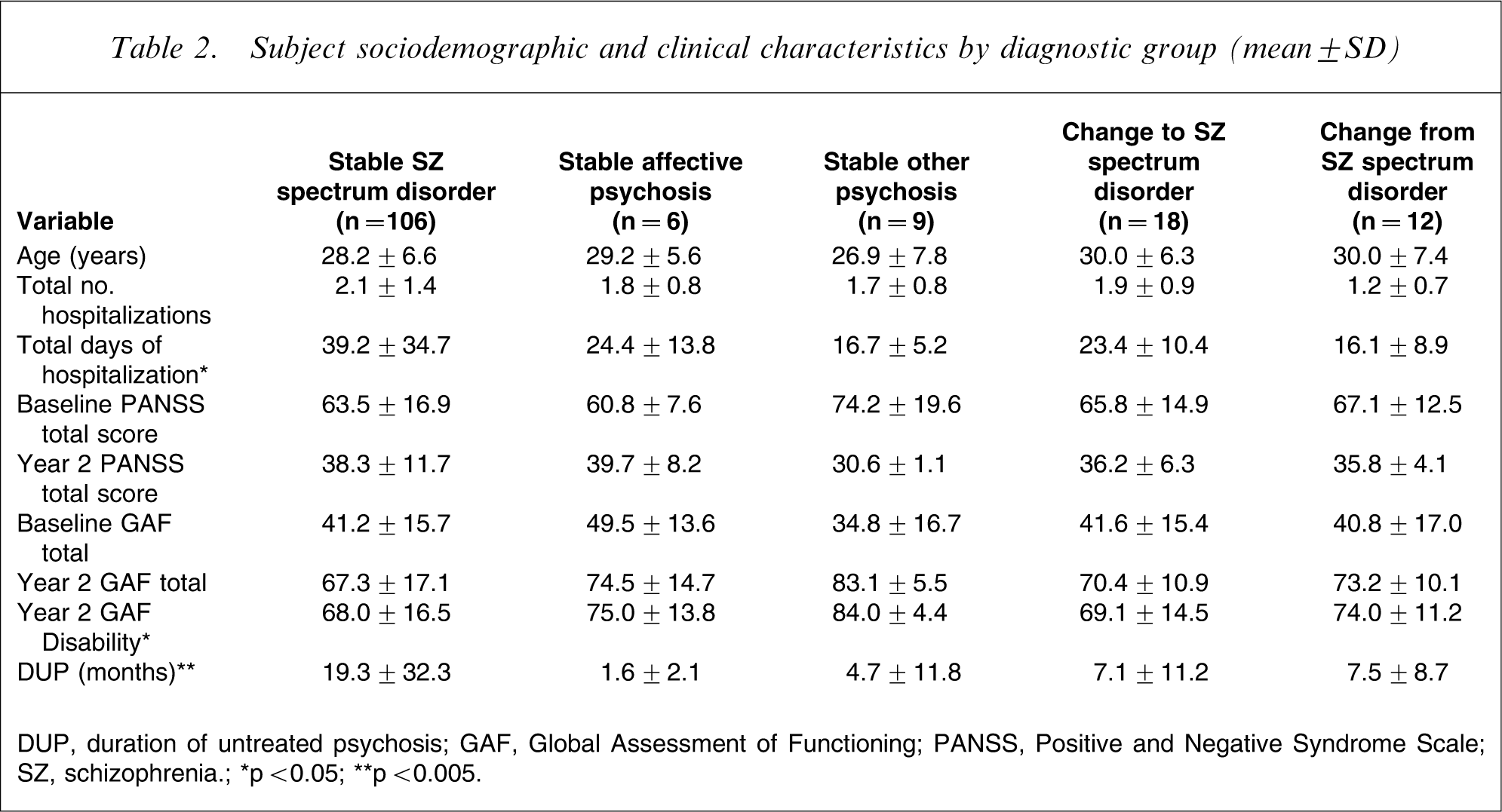
DUP, duration of untreated psychosis; GAF, Global Assessment of Functioning; PANSS, Positive and Negative Syndrome Scale; SZ, schizophrenia.
∗p<0.05; ∗∗p<0.005.
On performing a logistic regression, using age, gender, marital status, employment status, education, baseline PANSS and GAF scores and DUP to assess predictors of shift, we found the DUP to be the only significant predictor (p = 0.001, odds ratio = 1.075, 95% confidence interval = 1.03–1.12).
Discussion
The overall consistency of diagnosis between baseline and 24 month follow up was 57.1%. A total of 88 of the 154 patients received the same diagnosis at both evaluations. Consistent with the findings of other prospective studies [1, 5], the diagnoses with the best prospective consistency were schizophrenia (87.0%) and affective psychosis (54.5%); all other psychoses were less stable with a prospective consistency of 36.0%. The diagnoses receiving the largest influx at 2 year follow up were schizophrenia (n = 39) and affective psychosis (n = 8).
In a similar study on FEP patients by Whitty et al., patients whose diagnoses changed at follow up were found to have a significantly shorter DUP and were more likely to present with a lifetime history of alcohol or substance abuse [18]. The present subjects did not suffer from comorbid substance use; substance abuse is not very prevalent in this population in Singapore [19] and current substance abuse is an exclusion criteria for this programme. However, the present overall consistency was lower than that of Whitty et al. (75.0%) [18]. Other studies have, however, reported that the best pretreatment predictor of shift towards schizophrenia spectrum disorder is a lack of lifetime substance use disorder [5].
In the present patients too, a shorter DUP was a predictor of change in diagnoses at 2 year follow up. This is mainly because we were seeing patients with very short DUP, that is, earlier in the course of their illness. The DSM places an emphasis on the duration of symptoms for making a diagnosis; a diagnosis of brief psychotic disorder is to be given for episodes <1 month duration, schizophreniform disorder for episodes >1 month and <6 months, and schizophrenia for episodes ≥6 months. Because early intervention programmes around the world focus on getting patients into treatment programmes as early as possible, future diagnostic systems should take into account other diagnostic markers such as cognitive impairment or premorbid functioning. Thus, the variability of diagnostic stability across studies is confounded by the diagnostic system used [9], sample selection (FEP patients with short DUP vs chronic psychosis), as well as longitudinal diagnosis based on personal observation, patient and family information gathered over different time frames [20].
Diagnostic instability is also an important issue because of the implications for service planning and resource allocations [18]. Patients with schizophrenia would require different medical and psychosocial treatments as compared to patients with other psychoses. First-contact rates are often an underestimation of the true rates. In the present study there was a significant difference in the days of hospitalization among the different subgroups (Table 2); this indicates that the patient diagnoses determine the resources as well as service planning for any programme.
There were some limitations in the present study. The raters of the 2 year SCID were not blind to baseline SCID. This may have increased the diagnostic stability. Second, there were relatively few patients in some of the diagnostic groups, which limits any definitive conclusions. A third limitation was that 17.5% of those lost to follow up were suffering from other psychosis. Patients in the present study with a 2 year follow up and a baseline diagnosis of other psychosis had the lowest prospective consistency; thus this group may have been diagnostically more unstable. Some of the shifts in diagnoses were unexpected, such as one baseline schizophrenia shifting to psychoses NOS and two from schizophreniform disorder to brief psychotic episode. In all three cases, the case records were retrieved and reviewed by the team and it was concluded that the psychiatrists had erred in their 2 year diagnoses. The strengths of the present study are that the cohort consisted of almost entirely of drug-naïve patients with first contact with treatment, rather than being a first hospital admission sample with no comorbid substance abuse, and were all diagnosed using SCID both at the onset and after 2 years of follow up. Patients in this 2 year period met regularly with both their psychiatrist and their case managers, and were engaged in groups as well as structured activities and vocational training conducted by the staff. Families were involved in groups as well as individual counselling sessions. This increased contact with both patient and families may enhance longitudinal diagnostic assessments [10].
Physicians should be cognizant of the fact that FEP patients diagnosed as having other disorders may during the course of their illness shift to schizophrenia spectrum disorders; this shift has implications not only for pharmacotherapy but also for psychosocial interventions and prognosis [21]. It is imperative that these patients stay actively engaged with the services and have a reevaluation of diagnosis over the course of illness with standardized assessments [22]. Studies have shown that information on diagnoses and treatment is one of the most important elements perceived by patients and families of a good treatment programme [23]. Clinicians, researchers and patients should therefore be informed that although certain diagnoses such as schizophrenia and bipolar disorder are relatively stable, others could change over the course of the illness.
Footnotes
Acknowledgements
This project was supported by an Institutional Block Grant Received from the National Medical Research Council, Singapore.