
Abstract
Historically, eating disorders (EDs) were considered rare in non-Western societies. Consequently research interest about EDs in these societies and information about potential cross-cultural differences has emerged only relatively recently [1]. Being a member of a non-Western ethnic group was thought to confer some degree of protection [2, 3], although other hypotheses for the reported lower prevalence have included referral bias [4–6], social stigma in some non-Western societies [7] and a reluctance to consult Western-based physicians over traditionally based practitioners [8, 9].
The heightened interest in the cultural context of EDs has included speculation about different risk factors in non-Western cultures [10, 11], cultural variation in the expression of symptoms [12, 13], and whether outcomes differ in Western and non-Western societies [14]. Generally there has been little evidence for major differences in psychopathology, with studies showing no [4, 12, 13] or few differences [10, 15, 16]. Lee et al. considered fear of fatness to be a relatively recent reason for food refusal offered by people with anorexia nervosa (AN) in the Western world, and used this to explain why non-Western patients may be less likely to present with this core symptom [14]. More recently, a typography for atypical cases in Chinese patients has been proposed [17]. But with increasing exposure to Western dietary and beauty values, fear of fatness could become more common. That is, any differences may dissipate. Nevertheless at this stage body image dissatisfaction among Hong Kong women, for example, may not be as critical a risk factor for EDs [18].
Whatever the differences, if they do indeed exist, it is nonetheless plausible that classic features of EDs may have a different meaning in different cultural contexts and, in turn, different strengths of associations with ED psychopathology. That is, what is deemed as pathology directly associated with an ED in Western settings may in fact be due to reasons unrelated to the ED in non-Western settings [19, 20].
Psychological control, culture and eating and body image disturbances
It has been proposed that when ED patients in non-Western countries present without shape and weight concerns, issues of self-control may be the primary motivator instead [21]. A core construct associated with EDs is that of psychological control, and there is considerable clinical and empirical evidence to support this association in general (see [22] for a conceptual review). Control has been argued to be important in the aetiology [23, 24], maintenance [21], and treatment approaches [25] of EDs. The empirical evidence consistently supports a profile among those with an ED that includes overreliance on particular means by which to gain control, and reduced overall control [26, 27].
Importantly, there is reason to believe that what is a normal ‘control profile’ may differ between cultural settings. Marks noted that what has previously been considered normal (and thus leading to a treatment bias towards attaining specific control goals) may be influenced by the Western cultural value of personal autonomy [28]. In short, norms for psychological control may be culture dependent. For example, Japanese culture emphasizes external control, while European Americans reported greater internal control, as do those in Hispanic cultures [28]. Along the same lines, people from East Asian cultures are perhaps less likely to see matters in isolation; accordingly, a sense of personal control is less important. Ji et al. explained the difference in control preferences between East Asian and European societies in terms of the agricultural heritage of China lending itself to a collective society while the hunting and herding heritage of Europe favours autonomy and a looser social structure [29]. Chan provides additional empirical evidence of the East Asian culture valuing and endorsing external control [30].
Further, in terms of forming self-identity, Hong Kong adolescents seem concerned with ability and competence rather than other personal control aspects of identity [31]. Instead, in that culture there is an emphasis on external control, implying that an individual should work hard on their immediate task and fate would take care of the rest. Levels of acculturation also affect expression of control, and this provides a powerful argument for studying control issues in the primary cultural setting of that group rather than one in which they have relocated into. For example, first-generation Japanese students in the USA scored more highly on external control while their third- or later generation peer group scored more highly on internal control [28].
Compounding the Western bias [26] in understanding healthy psychological control styles has been the traditional reliance on constructs such as locus of control [32]. Invariably, the accompanying assumption is that a lack of active or internal control orientation in an individual is undesirable.
Bringing these tracts of research together, there is good reason to speculate that any reportedly strong association between EDs and particular issues of psychological control may be influenced by culture. This has been only partially tested in non-Western groups and to date has not yet been tested in clinical groups in two different countries alongside their non-ED peer group. Kempa and Thomas suggested that ethnic minority individuals may draw a sense of control from eating attitudes and behaviours when facing racism and oppression and the consequential sense of powerlessness [6]. In Hong Kong, Lee et al. investigated the relationship between psychological control and outcome in women with AN [33]. Participants classified as having a good outcome had significantly higher overall sense of control, positive sense of control and specific sense of control compared to patients categorized as having a poor outcome. In general, the control profile of Hong Kong women with AN was consistent with other research in that greater eating pathology is associated with a greater desire for control and greater use of more negative forms of gaining control. Lee et al. acknowledged that the study could not ascertain if these control issues were peculiar to EDs because the study design did not include a non-ED sample [33], and thus it is not clear what the psychological control norms would be in the Hong Kong population. Nevertheless, the authors hypothesized that while fear of fatness may not be present in some women with AN in Hong Kong, the general similarity of control profiles between typical and atypical (non-fat phobic) patients may mean that psychological control is a more useful culturally impervious diagnostic criterion. Because information regarding this is almost absent, an equally plausible hypothesis is that a typography using phenomenon of psychological control (rather than fat phobia as proposed by [17]) may be equally worthwhile exploring. That is, can variability between cultures, or typical and atypical cases within a culture, be captured by a typography based on psychological control profiles?
In summary, a particular control profile in itself may not be pathological; instead, the degree to which it deviates from the relevant population norm may be of greater clinical importance in understanding its association with EDs. To the best of our knowledge, this hypothesis has not been previously investigated despite the existing implication that control issues may be the psychopathology that permeates all cultures. This leaves the intriguing and entirely underresearched question as to whether any presumed pathological control styles, expressions and ambitions in EDs are culturally-bound.
The aim of the present study was to investigate psychological control profiles in North European Australian and Singaporean Chinese women with and without an ED in their own cultural setting. Based on the limited studies to date, it is hypothesized that (i) certain expression of psychological control may be culture dependent and, in particular, Singaporean Chinese participants will prefer less assertive and more passive means by which to experience control, and have less motivation for control overall than their North European Australian counterparts; (ii) the previously observed strong association between psychological control and EDs will permeate both cultures; and (iii) the specific psychological control pathology associated with an ED may be culture dependent.
Method
Participant and recruitment method
Participants (n = 117) were women aged 14–38 years recruited in the 2 years ending June 2004 across two countries (Australia and Singapore) as part of a larger study investigating cross-cultural differences in body composition, body image, and EDs. The study was approved by the relevant Ethics Committee and Authority at each recruitment site in each country (Human Research Ethics Committee, University of Sydney; Ethics Review Committee, Central Sydney Area Health Board; Human Research Ethics Committee, Western Sydney Areas Health Board; Ethics Committee, Singapore General Hospital). When participants were deemed minors (under 16 years of age in Australia; under 21 years of age in Singapore), written informed consent was obtained from the participant's parents.
The ED participants were recruited from four teaching hospitals affiliated with University of Sydney and from two teaching hospitals in Singapore. All were undergoing treatment for an ED (AN, bulimia nervosa (BN), or eating disorder not otherwise specified (EDNOS)) as classified by DSM-IV criteria [34].
Healthy Australian participants (of North European ethnicity) who had never been diagnosed with an ED (as per clinical interview self-report) were recruited via advertising flyers at University of Sydney campus and website, and by word of mouth. Participants needed to have been born in Australia, or migrated there from North European settings before the age of 12 years. Healthy Singaporean participants (Chinese ethnicity) were recruited through the nursing department at Singapore General Hospital. In this instance, potential participants were made aware of the study by verbal announcements through the nursing management structure and each staff shift handover. Exclusion criteria were non-fluency in spoken or written English, self-report of current or past ED, and current pregnancy or lactating.
Data collection and measures
In all cases, face-to-face appointments were made to obtain written consent, undertake the physical assessments (weight, height etc.), and complete demographics sheets recording ethnicity/cultural group and age. For the ED participants, formal diagnosis was made by the treating psychiatrists using DSM-IV criteria, and collected from their current clinical medical records in the clinic setting where they were receiving treatment. All participants then completed the Shapiro Control Inventory (SCI) [35] in their own time as part of a larger questionnaire booklet examining cultural differences in ED psychopathology and sociocultural factors. This was returned immediately or shortly thereafter.
Shapiro Control Inventory
The SCI is a 187-item Likert-style questionnaire assessing an individual's multi-dimensional psychological control profile. The duration for completion is 20–30 min. The SCI has been used to investigate issues across a wide range of psychiatric and medical populations, including in ED populations in New Zealand [27] and Hong Kong [33]. It uses language comprehensible to individuals with equivalence of 8 years formal education, and has demonstrated good internal consistency across clinical populations, including Hong Kong Chinese women [33, 35–37]. Nine scales examine three different facets of control, which can be summarized as follows.
(1) As the first and most general component, Sense of Control “measures a person's view that s/he has control, as well as the belief that s/he can gain control if desired” (p. 7, [35]) The Overall Sense of Control score (scale 1) gives the broadest view of the respondent's sense of control, and is further analysed with respect to its constituent parts: Positive Sense of Control (scale 2), which assesses belief in the ability to attain future control, ability to utilize positive modes of control, and current level of self-control; and Negative Sense of Control (scale 3), which assesses the sense of loss of control in areas previously experienced as controlled, aspects of inadequate of self-control or environmental control, and feelings of helplessness and passivity. Sense of Control is also examined with respect to domains in which such control is experienced, either as an overall Domain Sense of Control score (scale 4) or by each of seven specific domain scores (body, mind, relationships, self, career, environment, or impulse control) imbedded in the scale. In this way, to what extent loss of control in one domain is also experienced in another can be examined.
(2) Mode of Control assesses the means by which an individual attempts to attain and maintain a sense of control. Distinctions are made across the two dimensions of assertive–yielding and positive–negative, thus yielding four scales. Positive–assertive (scale 5) measures the perceived ability to use an active, altering mode of control, and includes descriptors such as ‘decisive’, ‘leading’ and ‘communicating needs’. Positive-yielding (scale 6) measures sense of control through means of letting go of active control. Descriptors include ‘patient’ and ‘accepting’. Negative-assertive (scale 7) measures too much active control (‘manipulating’, ‘dogmatic’) while Negative-yielding (scale 8) measures aspects of too little control, with descriptors such as ‘indecisive’ and ‘manipulated’.
(3) Motivation (Desire) for Control (scale 9) measures the desire for psychological control, over oneself, others, and the environment. Components of desire include the perceived importance of being in control, efforts to achieve control, and fear of losing control.
Statistical analyses
All analyses were conducted with SPSS Version 13.0 for Windows (SPSS Inc., Chicago, IL, USA). Each SCI scale and the seven domain-specific subscales of scale 4 were analysed using the general linear model (GLM) with cultural group (North European Australian and Chinese–Singaporean) and caseness (ED or no ED) as independent variables. Because body mass index (BMI) was associated with cultural group (t(115) = 1.9, p = 0.056) and caseness (t(115) = 6.7, p = 0.000), and both BMI and age were significantly associated with aspects of the dependent measure (SCI scales), BMI and age were included as covariables in all linear regression analyses.
Results
Characteristics of the sample
Participants from both cultures included young women in the age range typical of those who present with EDs both in Western and Asian settings (Table 1) [33, 38]. Among the ED participants, 69% had a primary diagnosis of AN, 25% a primary diagnosis of BN, and the remaining 3% were diagnosed with EDNOS.
Demographic characteristics of sample (mean ± SD)
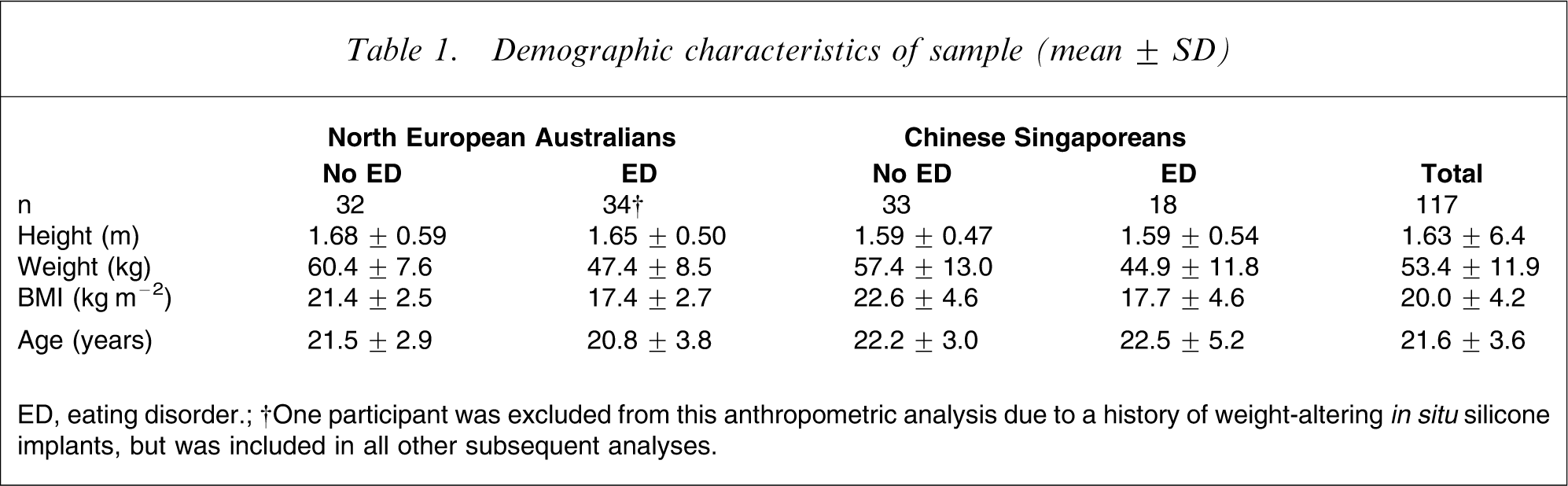
ED, eating disorder.
†One participant was excluded from this anthropometric analysis due to a history of weight-altering in situ silicone implants, but was included in all other subsequent analyses.
Relationship between sense of control, culture and caseness
Culture was significantly associated with three aspects of psychological control (Table 2), all of which related to the means by which people prefer to gain control. North European Australian participants preferred to gain control through positive assertive methods (SCI scale 5; F(1,110) = 17.4, p < 0.001) and positive yielding methods (SCI scale 6; F(1,110) = 6.4, p < 0.05), and were significantly less likely to use negative yielding methods (SCI scale 8; F(1,110) = 4.0, p < 0.05) to attain control than their Chinese Singaporean counterparts.
Psychological control (SCI) scores by culture and caseness (mean ± SD)
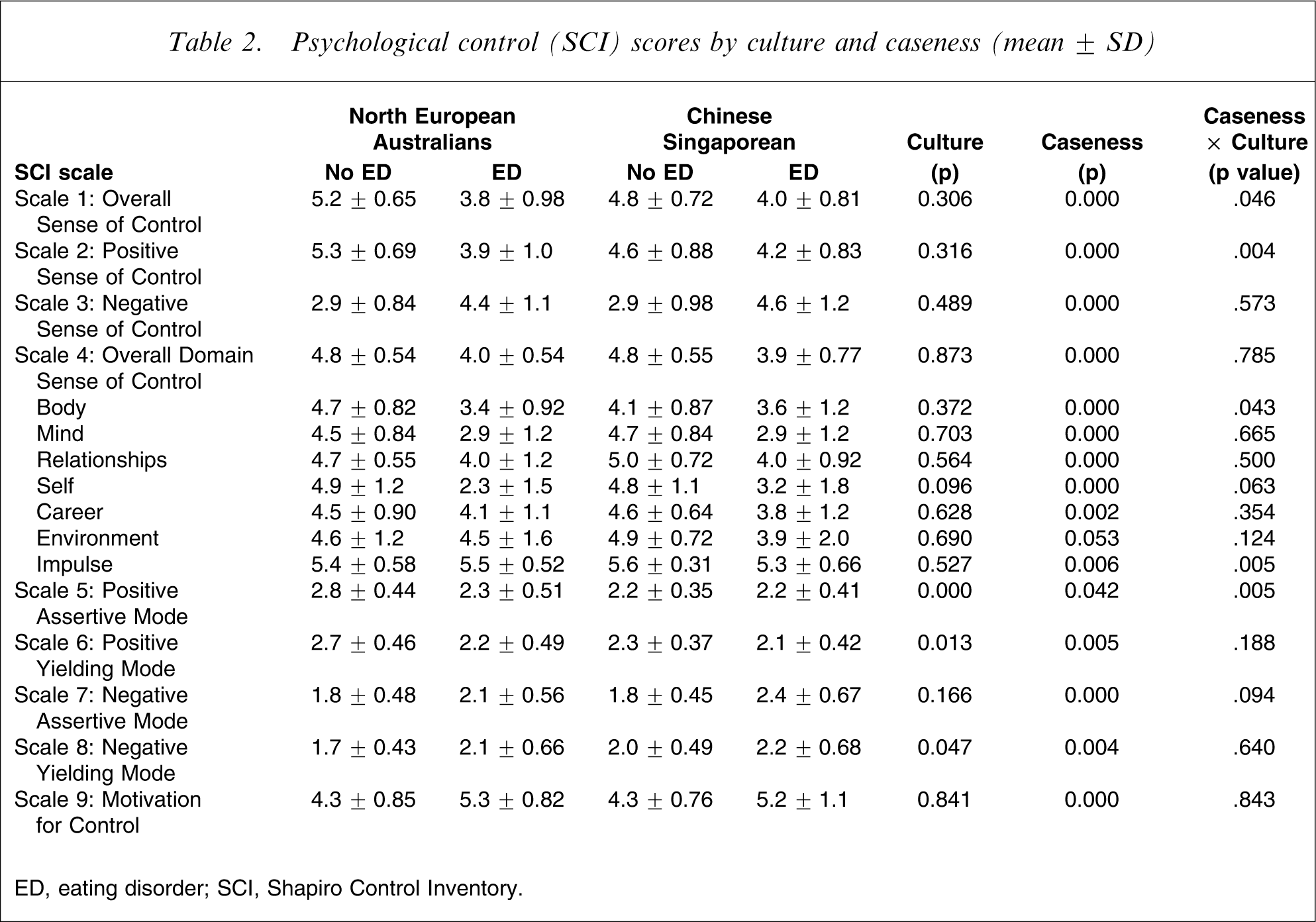
ED, eating disorder; SCI, Shapiro Control Inventory.
Caseness was significantly associated with all major SCI scales. That is, ED participants reported a reduced overall sense of control (SCI scale 1; F(1,111) = 35.2, p < 0.001) including the positive and negative components of this (SCI scales 2,3; F(1,111) = 18.3, p < 0.001 and F(1,111) = 48.3, p < 0.001 respectively), along with reduced control in all domains (SCI scale 4; F(1,103) = 51.8, p < 0.001) of functioning (excepting control over environment), reduced use of positive means of gaining control (SCI scales 5,6; F(1,110) = 4.2, p < 0.05 and F(1,110) = 8.1, p < 0.01, respectively), increased use of negative means (SCI scales 7,8; F(1,106) = 17.4, p < 0.001 and F(1,110) = 8.4, p < 0.01, respectively), and significantly elevated desire for control (SCI scale 9; F(1,111) = 23.4, p < 0.001).
A significant interaction for culture and caseness was found for specific aspects of psychological control. In this respect, compared with their Chinese Singaporean ED counterparts, eating disordered North European Australians deviated significantly more from their cultural norm on aspects of overall sense of control (SCI scale 1; F(1,111) = 4.1, p < 0.05), positive sense of control (SCI scale 2; F(1,111) = 8.9, p < 0.01), positive assertive methods of attaining control (SCI scale 5; F(1,110) = 8.3, p < 0.01) and control in the domain of body (SCI 4 subscale Body; F(1,108) = 4.2, p < 0.05). Compared with their North European Australian ED counterparts, Chinese Singaporeans with an ED deviated significantly more from their cultural norm on aspects control in the domain of impulsivity (SCI subscale 4 Impulsivity; F(1,109) = 8.1, p < 0.01).
Discussion
Psychological control is a construct of sustained interest in the area of EDs, but one that requires further explication to reconcile the contradictory literature within cultures and add to the limited knowledge base across cultures. Theories and some empirical evidence suggest that expressions of control may be, in part, affected by culture. Existing arguments are also made that the expression of ED symptoms may be influenced by culture. This is the first study to examine multidimensional aspects of psychological control in ED subjects and their non-ED peer group concurrently in two cultures.
The study does suffer from a number of limitations, many of which are associated with obtaining cross-cultural samples, and a larger sample overall would have enabled more subtle and detailed results beyond those obtained, including analysis by ED subtype. A further limitation is that the sample was recruited under different circumstances and with different strategies – in part due to the cultural and infrastructural difference between Australia and Singapore. Although care was taken to minimize such differences, they may have, nevertheless, impacted on the findings. Also, the ED participants recruited in the treatment centres may not be representative of the wider ED population in each setting, especially given the referral bias that may be operating in non-Western clinic settings.
The overall pattern revealed in this series of analyses was that women with EDs in these two cultures exhibit control profiles that cannot be differentiated by culture. That is, ED women, irrespective of culture, can be marked out from their non-ED peer group by their reduced overall sense of control, greater negative sense of control, reduced control in the domains of mind, relationships, self and career, and marginally lower levels of control in the domain of environment. ED women across both cultures also reported significant differences in the methods by which they attain psychological control. Having an ED seems to mute use of active assertive methods. It means that these people are less likely to experience control through trusting others, and more likely to resort to dogmatic methods at the same time as feeling manipulated by others. Clearly, this occurs while experiencing elevated motivation for control. The ED control profile across these two cultures is very similar in these respects, and it is a profile that concurs with existing recent studies within cultures [27, 33, 39]. In particular, Lee et al. observed that AN patients in Hong Kong used less assertive means of achieving control and were more likely to view themselves as being controlled by others when compared to normal or recovered individuals [33].
Although the aforementioned similarities initially suggest that control psychopathology may be impervious to culture, this is not the case for all aspects of control, and some important differences exist. In terms of cultural norms, in the present study the means by which individuals prefer to attain and maintain control is significantly associated with culture, with Chinese Singaporean women being less likely to use methods involving assertiveness and self-initiation, whereas North European Australians were less likely to use strategies that risk a sense of manipulation or indecision. Put another way, although no more motivated to achieve control than Chinese Singaporean women, the Australian norm is one of less timidity and more assertiveness in the choice of methods by which day-to-day control is achieved. Longstanding cultural traditions in both settings could account for this. East Asian societies have been described as highly conforming and supportive of a social norm that promotes a sense of fatalism [29, 31]. Likewise, a western cultural conditioning to value self-responsibility and decisiveness is likely to colour which methods of gaining control are selected. This style is one that also permeates psychological interventions [39]. Although we hypothesized that Singaporean Chinese women would have less motivation for control overall, the present study did not find this. A potential reason is that level of acculturation was not taken into account; and westernization in Singapore in view of its prominent use of the English language, and access to English language media, may have served to distort (increase) desire for control in this more recent sample.
By far the most intriguing findings, especially in terms of understanding the directionality and extend of control psychopathology, relate to the interactions between cultural group and caseness. In many respects, there was some evidence of convergence at the stage of a clinical ED, yet on specific aspects of psychological control North European women with an ED deviated much more from their cultural peers than their Chinese Singaporean ED counterparts. That is, the extent of specific aspects of control pathology in those with an ED is culture dependent, with North European Australian women more likely to exhibit much more severe deviations from their non ED peers in the direction of reduced overall control, reduced control in the domain of body, and more aberration in their ability to utilize positive assertive methods by which to gain control. Whereas having an ED in Singapore may lead to greater deviancy from one's Chinese Singaporean peer group in the domain of impulse control than one's Western ED counterparts. It is not clear why this latter finding emerged but it may reflect the higher proportion of BN patients in the Singaporean Chinese ED sample compared to the North European Australian clinical sample.
The study of the role of psychological control in EDs in non-Western groups has only recently commenced and further studies are clearly necessary before more conclusions can be drawn. Fear of fatness has been previously proposed to be a culture-bound feature of EDs [40], and in many respects the present study suggests that, in general, psychological control issues may be the more universal and less culture-bound feature of EDs. That is, an ED powerfully distorts sense of control irrespective of culture. That said, the present study provides preliminary evidence that it is western culture that may experience the more pathological shifts once an ED takes hold. Although these findings cannot evaluate the hypothesis that issues of self-control are the more primary motivator in non-Western EDs [21], they nonetheless suggest that the ambition to achieve self-control is no more intense than that seen in Western ED cases.
Clearly, cultural differences with respect to aspects of a normal control profile need to be taken into account when understanding the meaning or significance of any assumed control psychopathology associated with an ED. In short, deviation from a cultural norm may be just as important in understanding control psychopathology in each culture, and universal conclusions cannot be drawn simply about absolute levels of control. In specific areas, deviation from a cultural norm on issues of psychological does not occur to the same degree in Singaporean ED patients. It could be that future shifts towards westernization (and thus more westernized control norms) could see ED women in Asian settings become more deviant in their control profile, and for this reason future research should consider the effect of adherence to Western or traditional cultures. If deviance from a cultural norm is something that matters, then this may not be static. These are all important hypotheses requiring further examination before control-based approaches to treatment [e.g. 21] can be confidently applied.
Footnotes
Acknowledgements
This study was partly supported by the Edith Mary Rose Travelling Scholarship awarded to the first author.