
Abstract
A forensic psychiatric patient's fate often lies in the space between a society's perceptions of its need for safety and an individual's right to liberty [1, 2]. It is this uncharted space between these two often polar opposite needs that governments and legislatures have struggled to define. Within the past four decades, Western countries have begun a journey toward the deinstitutionalization of patients with mental disabilities [3, 4]. This trend has focused primarily on the individual's right to freedom and the result has been to move mentally ill persons from institutions into the community [5]. In many jurisdictions, however, this promise – especially for forensic patients – remains little more than theoretical [6]. Yet, to preserve legal rights, the “least restrictive alternative” doctrine must apply to all cases involving persons institutionalized because of their mental disabilities.
In 1979, the Chinese Criminal Code was adopted by the Second Session of the Fifth National People's Congress [7]. Article 18 of this Code imposes a legal obligation on the family members or guardians of persons found ‘not guilty by reason of a mental disorder’ (NGMD) to arrange for their surveillance and medical treatment [8].
If deemed necessary, the government may impose compulsory treatment on persons found NGMD. Yet, enforcement and integration of these laws have not been achieved. Continued treatment and compliance with the Code have been lacking and often non-existent. The forensic psychiatric service system has not made the necessary advancements to properly serve the community if and when treatment is necessary and needed [9].
At the end of 2004, 22 Ankang hospitals were established in 18 different provinces, autonomous regions and municipalities (not including Hong Kong, Macau and Taiwan) of China [10]. Thus, approximately, half of the provinces in China, including Hunan, do not have an Ankang hospital. As a result, treatment is not uniform throughout the region, and varies significantly from province to province. By way of example, if an Ankang hospital is available in the province in which the patient resides, a patient found NGMD would be able to receive psychiatric treatment there. However, if an Ankang hospital were not available, the care and custody would take place in general psychiatric hospitals or in the community through any arrangements made by family members. This is most common in rural areas where resources are limited and the patients have to pay for treatment [10, 11]. Generally, the government covers all expenses for general patients hospitalized in Ankang hospitals but covers only a portion of the expenses incurred by forensic patients. Percentages of expenses covered for forensic patients differ based on each province's individualized economic level [11].
An additional barrier is the relatively high proportion of forensic patients who are sometimes unable to get necessary medications and treatment at China's psychiatric hospitals, especially where the Ankang hospitals are not available [12]. The Ankang hospital is run by the public security system while the general psychiatric hospitals are run by the health and welfare system. Generally, most mentally ill patients in China undergo involuntary treatment while in the custodial and general psychiatric hospitals. Patients are not afforded a legal right to refuse treatment in Ankang hospitals based on Act 18 of Chinese Criminal Code [8]. Patients in the general psychiatric hospitals can request to not have certain treatment but it is rare for them to make such an application. The purpose of the present study was to track persons referred for forensic psychiatric assessments through the Chinese legal system.
Method
From 1 January 2001 to 31 December 2002, 240 mentally ill offenders were assessed at the forensic psychiatric assessment center of Central South University, Hunan, China. All demographic information was gathered from police files and psychiatric reports maintained in this center. A 16-item self-developed structured questionnaire was mailed to patient family members to determine the disposition and status 1 year after patient psychiatric assessment. Items in this questionnaire included the courts’ decisions, sentences, treatment at forensic psychiatric hospital (FPH), general psychiatric hospital (GPH) or outpatient department (OPD), dangerous behaviours, recidivism, management of the illness, financial support and other such factors. The family member was permitted to complete the questionnaire using information contained in the court documents and medical records of the hospitals. No statistical significance was found in the sex, age, education level, marital status, diagnoses or psychiatrist opinion of criminal responsibility between the group of 170 subjects who returned completed questionnaires and the group of 70 subjects who did not complete their questionnaire.
A total of 170 questionnaires (70.8%) were fully completed and returned by family members on 31 March 2004. Fifty-seven questionnaires were not returned; 11 questionnaires were returned due to improper address information; and two questionnaires were not fully completed.
Results
Demographic characteristics
The subjects consisted of 87.7% men and 12.3% women (Table 1). The average age was 32.71±9.30 years. The education level of more than half of the patients (55.9%) was at the middle school level. A total of 53.5% of the subjects were unmarried. Most of the patients (68.8%) came from rural areas. The proportion of patients who had a psychiatric history and a conviction history before their index offence was 88.8% and 17.1%, respectively.
Demographic data (n = 170)
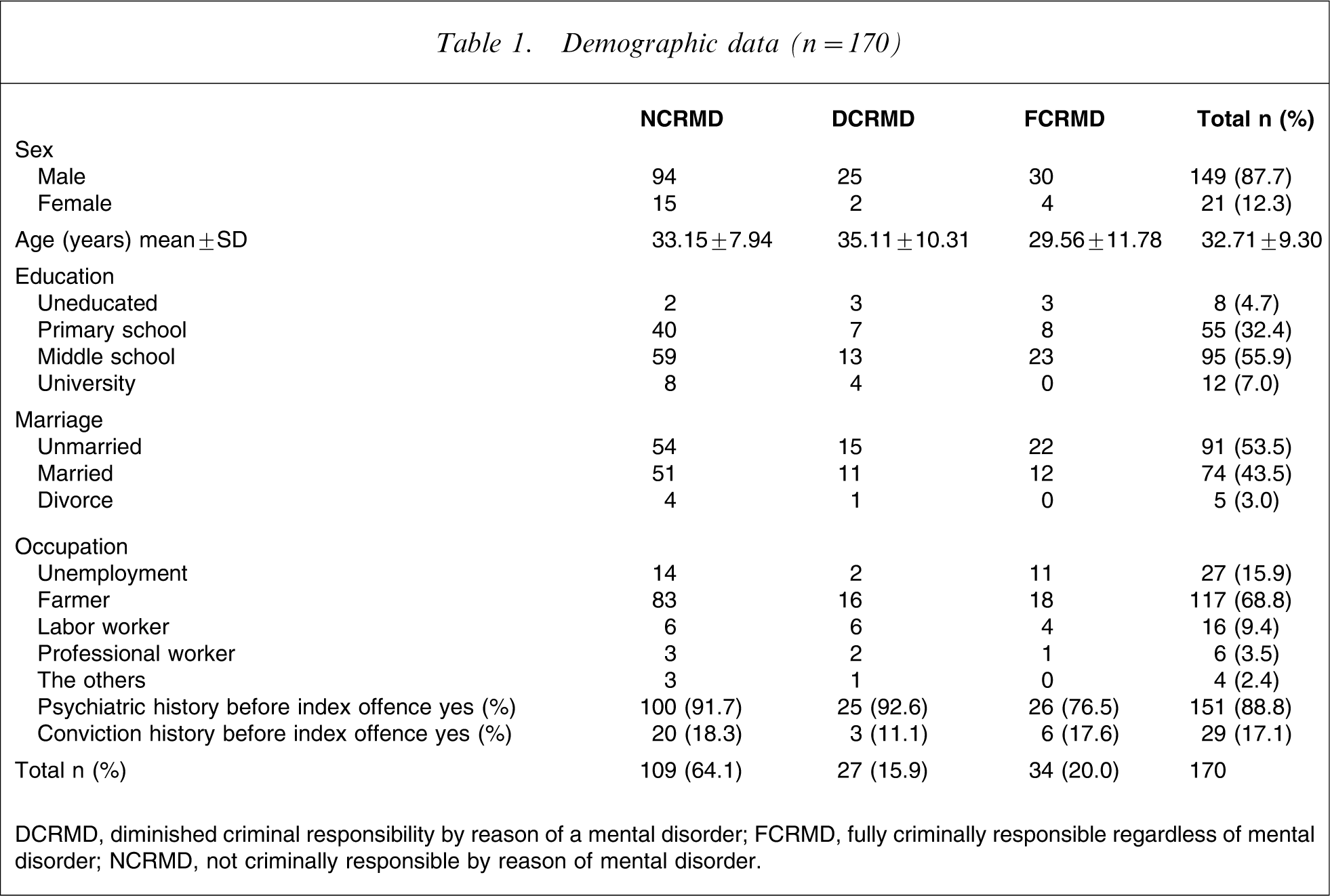
DCRMD, diminished criminal responsibility by reason of a mental disorder; FCRMD, fully criminally responsible regardless of mental disorder; NCRMD, not criminally responsible by reason of mental disorder.
Index offence
Most of the subjects had been convicted of a violent crime, such as murder/attempt (57.1%), assault (12.9%), robbery (8.2%) and sexual assault (7.1%; Table 2).
Index offence (n = 170)
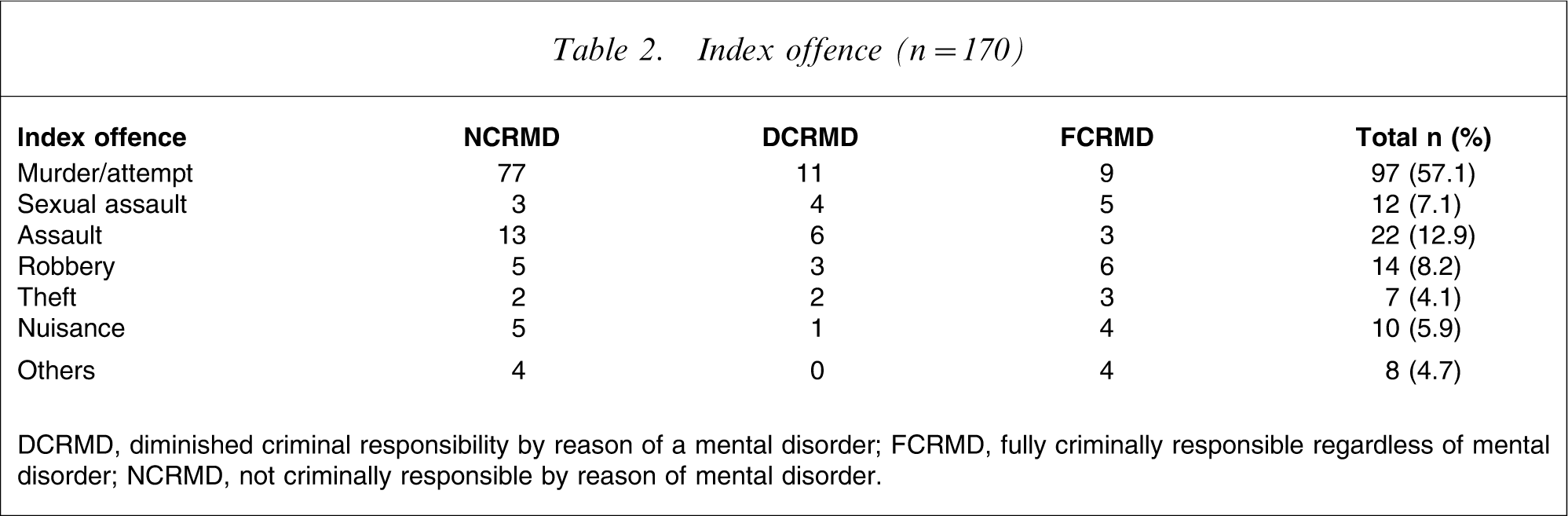
DCRMD, diminished criminal responsibility by reason of a mental disorder; FCRMD, fully criminally responsible regardless of mental disorder; NCRMD, not criminally responsible by reason of mental disorder.
Psychiatric diagnosis
A total of 71.8% of patients were diagnosed with schizophrenia, 12.4% with a mood disorder, 7.6% with mental retardation and 8.3% with other diagnoses (Table 3).
Psychiatric diagnosis (n = 170)
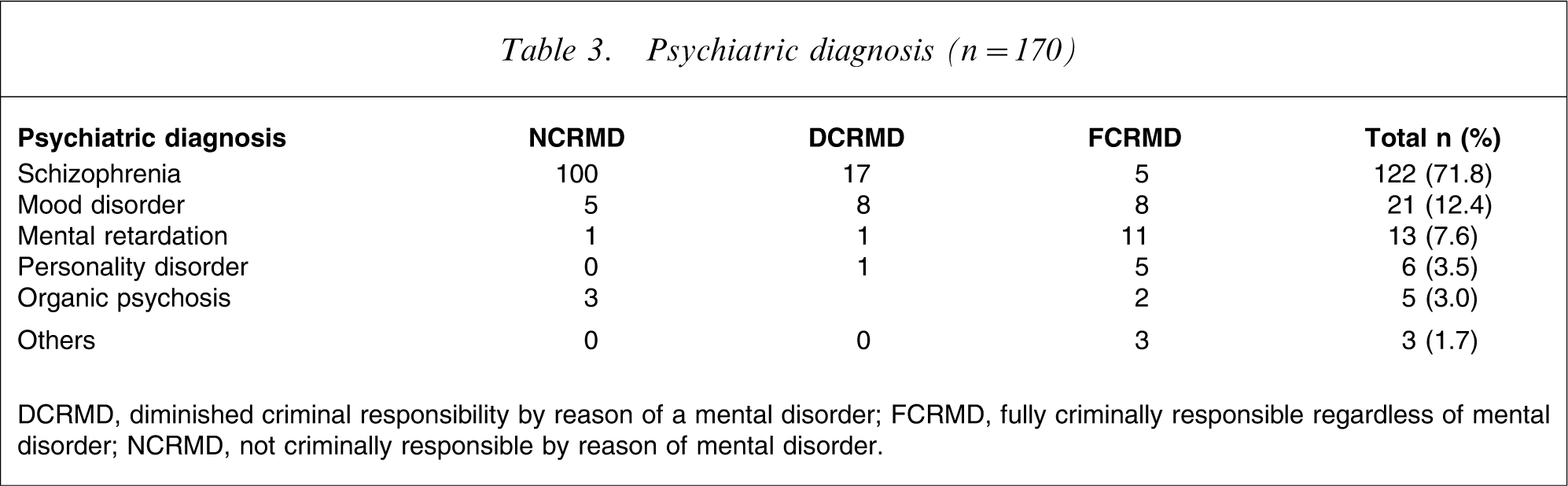
DCRMD, diminished criminal responsibility by reason of a mental disorder; FCRMD, fully criminally responsible regardless of mental disorder; NCRMD, not criminally responsible by reason of mental disorder.
Psychiatrists’ opinion and judicial decision
Table 4 shows that 109 subjects (64.1%) were determined by a psychiatrist not to be criminally responsible by reason of mental disorder (NCRMD), 27 (15.9%) had diminished criminal responsibility by reason of a mental disorder (DCRMD) and 34 (20.0%) were found to be fully criminally responsible regardless of their mental disorder (FCRMD). In a total of 99 out of 109 NCRMD cases, six out of 27 DCRMD cases and five out of 34 FCRMD a decision of not guilty was handed down by the judicial system. The agreement between the psychiatrist recommendation on the issue of criminal responsibility and judicial determination of guilt was 87.6% (i.e. [(99 + 21 + 29)/170]×100).
Psychiatric opinion and judicial decision (n = 170)
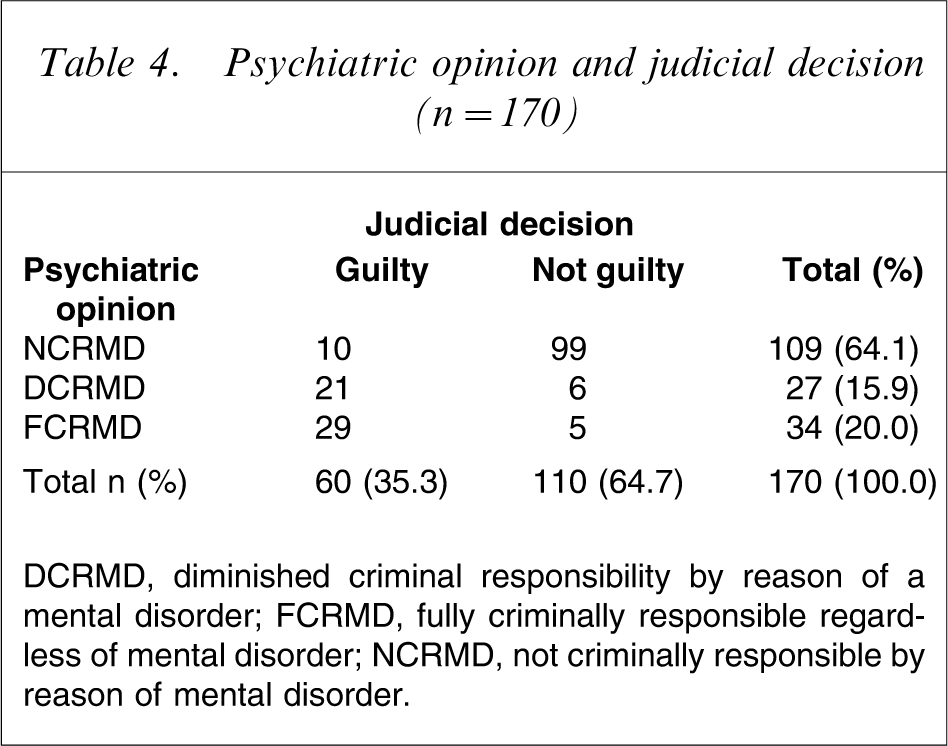
DCRMD, diminished criminal responsibility by reason of a mental disorder; FCRMD, fully criminally responsible regardless of mental disorder; NCRMD, not criminally responsible by reason of mental disorder.
Sentences
Table 5 shows that 10 NCRMD subjects were found guilty and given a sentence varying from 1 to 20 years. Only one subject received probation.
Sentences for the mentally ill offender found guilty (n = 60)
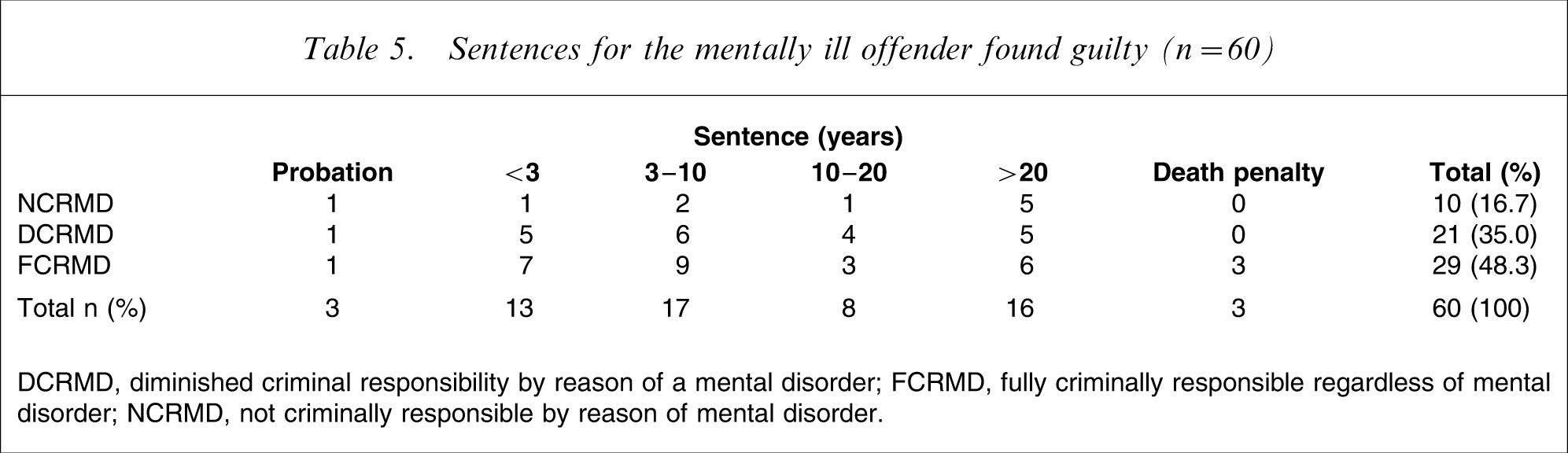
DCRMD, diminished criminal responsibility by reason of a mental disorder; FCRMD, fully criminally responsible regardless of mental disorder; NCRMD, not criminally responsible by reason of mental disorder.
Dispositions
Table 6 shows that among the mentally ill persons found to be NGMD, only six out of 110 (5.5%) were granted custodial treatment at an FPH, while 68 out of 110 (61.8%) were discharged to the community without any mandated psychiatric treatment.
Disposition of the mentally ill offender found not guilty (n = 110)
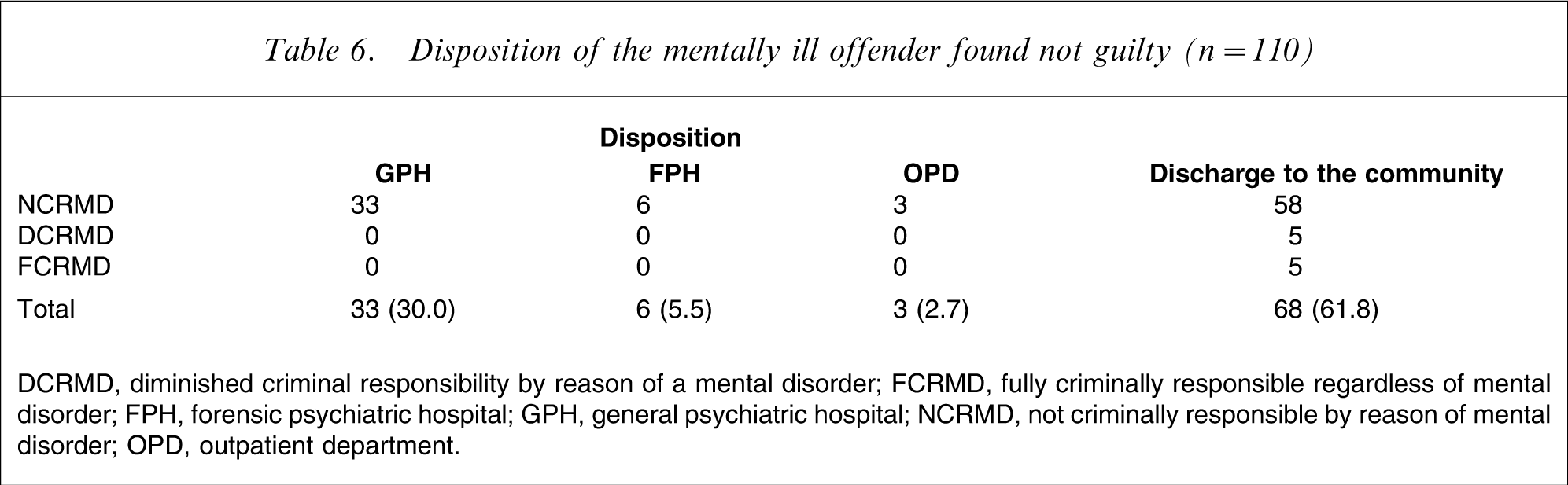
DCRMD, diminished criminal responsibility by reason of a mental disorder; FCRMD, fully criminally responsible regardless of mental disorder; FPH, forensic psychiatric hospital; GPH, general psychiatric hospital; NCRMD, not criminally responsible by reason of mental disorder; OPD, outpatient department.
Recidivism
Table 7 shows that seven out of 110 subjects found not guilty committed another offense within 1–3 years after receiving psychiatric treatment. Of those who reoffended, five out of seven were MCRMD patients. Four out of the five cases involved murder or attempted murder.
Recidivism of mentally ill offender found not guilty (n = 110)
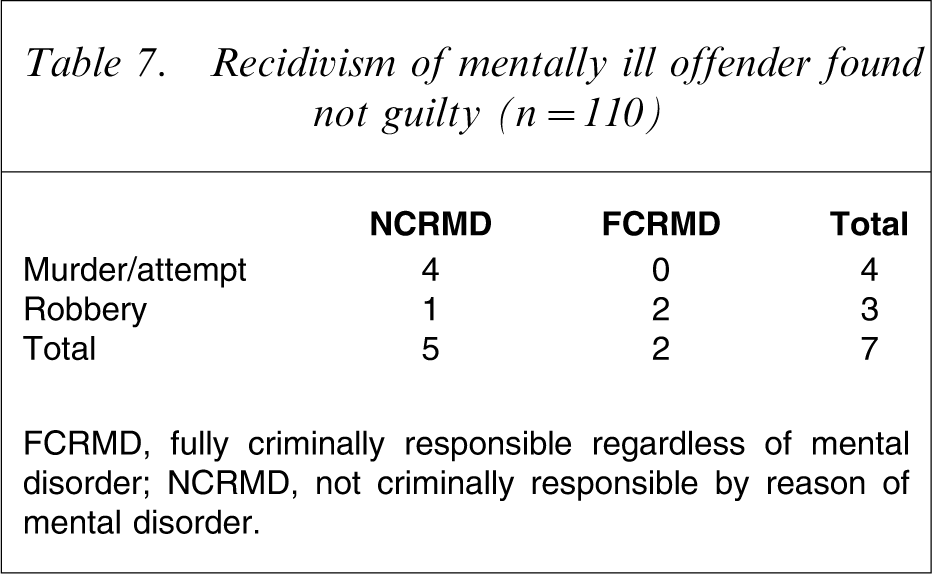
FCRMD, fully criminally responsible regardless of mental disorder; NCRMD, not criminally responsible by reason of mental disorder.
Discussion
The subjects of this study are similar to those of other studies done in and outside China. Similar to the other studies, the subjects in the present study were young men (87.7%) with low education levels, and unmarried. The present results differed from the study done by Livingston JD in British Columbia, Canada. This is due to the different circumstances surrounding the subjects such as the relatively high number of subjects who resided in rural areas (68.8%) and the overall involvement in more violent crimes, such as murder or attempted murder (57.1%) [9, 13, 14].
There are several potential explanations for these different results. Medical insurance is non-existent for most of the patients with mental disabilities residing in the rural areas of Hunan, China [15]. The patients and their families are relatively poorer than those from urban areas. The rural patients are highly likely to not seek and receive treatment due to their inability to afford such care, as opposed to patients in urban settings [15, 16]. Therefore the outcome is that the higher proportion of previously untreated forensic patients come from rural areas.
Concerning the high proportion of violent offences in Hunan, it is hypothesized that the Chinese public has a higher tolerance for non-violent or less violent offences, such as nuisance or property-related crimes committed by persons with mental illness. Therefore, lesser crimes are not frequently reported to the police and are less likely to result in criminal proceedings [9, 14]. In addition, consideration is taken into account that the patient or the patient's family would have to cover legal expenses and therefore Chinese society will excuse the lesser crimes for the sake of their low economic status. Unfortunately, further scientific data are necessary to support this hypothesis.
The present study does suggest that the agreement between psychiatrist recommendations as to criminal responsibility and judicial determinations of guilt is consistent (87.6%). This is remarkably similar to the outcomes found in the USA and Canada [17]. In China, very few cases involving offenses committed by persons with mental disabilities are brought to the court's attention. It is also not necessary for a treating psychiatrist to be present in court, and very few judicial decision-makers receive specific training in the area of mental disability and psychiatric assessment. This may best explain the overwhelming consistency between the psychiatrist's opinion and judicial determination in most of the cases.
The current study shows that the number of forensic patients discharged to the community without any psychiatric treatment is overwhelmingly high. The reasons, as stated here, are believed to be the lack of availability of FPHs in Hunan, China and the non-existent medical insurance for the patients in rural areas. The most prominent feature is the lack of enforcement behind the safeguards implemented in the Code.
In the present study only seven out of 110 subjects (6.4%) found not guilty and mentally disabled, offended following psychiatric treatment within 1–3 years after release. The rate of recidivism is dramatically lower than that found in the Livingston et al. study in British Columbia, Canada, in which 36 out of 200 persons (18.0%) discharged faced a combined total of 92 new criminal charges during the 2 year follow-up period [14]. Differences between these two studies are presumed to exist due to family support for those in China and the underreporting of offenses in Chinese society.
In summary, the majority of judicial decisions are consistent with psychiatric opinion of criminal responsibility. After such adjudication further psychiatric treatment is often neglected. Hunan, China must make a continued investment into the availability and quality of outpatient mental health treatment upon discharge for the forensic patients.