
Abstract
Objective:
To identify subgroups of forensic psychiatric patients based on the age onset of serious mental illness and offending and assess the external validity of the subgroups with theoretically based sociodemographic, clinical, legal and risk-related variables.
Method:
The age onset of serious mental illness and criminal contact was ascertained for a sample of 232 patients. A range of sociodemographic, clinical, legal and risk-related variables were coded to assess whether age onset subgroups differed in a manner consistent with the literature on typologies of mentally ill offenders.
Results:
One-quarter of the sample was classified as early starters (patients whose first offense occurred before becoming mentally ill), while two-thirds were late starters (where first offense occurred following illness onset). A small percentage (8%) of patients were deemed late late starters, defined as late starters who had experienced 10+ years of illness and were >37 years upon first arrest. A larger proportion of early starters had a substance use disorder, antisocial personality disorder and a greater number of static/historical risk factors for violence. Early starters were younger upon first arrest and had more previous criminal contacts compared to late starters and late late starters. Mental illness was found to start later in life for late late starters; this group was also more likely to have been married and to have a spouse as victim in the index offense.
Conclusion:
We found support for distinct subgroups of mentally ill offenders based on the age onset of illness and criminal contact. Compared to late starters, offenses committed by early starters may be motivated more frequently by antisocial lifestyle and attitudes, as well as more instrumental behaviors related to substance abuse. In addition, late late starters may represent a distinct third subgroup within late starters, characterized by relatively higher levels of functioning and social stability; future work should replicate. Findings suggest different rehabilitation needs of the subgroups.
Introduction
Evidence suggests that individuals with serious mental illness (SMI) are at elevated risk of violence (Brennan et al., 2000; Douglas et al., 2009), including homicide (Richard-Devantoy et al., 2009; Simpson et al., 2004; Taylor and Gunn, 1999; Wallace et al., 1998). However, people with SMI may behave violently for a variety of motivations (Nestor, 2002), including as a direct result of positive symptoms of psychosis or when symptoms result in heightened stress or exposure to provocation (Hiday, 1997). Other ‘conventional’ risk factors are relevant to the violence committed by those with SMI: neurocognitive impairments, early behavioral problems, substance misuse and antisocial personality are more common in people with schizophrenia (Andrews et al., 2006) and may partly explain the increased prevalence of violence in SMI (Hodgins, 2008). In addition, varying developmental trajectories to violence are well documented: in particular, Moffitt’s taxonomy differentiating life course persistent (LCP) and adolescent-limited (AL) offenders has shown that early and severe childhood behavior problems are associated with violence and criminality, as well as significant mental and physical health problems that persist into adulthood (Moffitt, 1993; Moffitt et al., 2002; Piquero et al., 2010; Satterfield et al., 2007).
A similar distinction has been made for individuals with psychotic illnesses who offend. Hodgins (Hodgins, 2008; Hodgins et al., 2014) proposed that the age at which antisocial behaviors emerge is a key variable to identify those whose offending is the result of illness as opposed to other criminogenic risk factors. She posited three trajectories to violence among individuals with SMI: (1) Type I offenders (‘early starters’, or ES), who exhibit antisocial behavior that begins in childhood or adolescence, prior to illness onset, and persists into adulthood; (2) Type II offenders (‘late starters’, or LS), who exhibit no antisociality prior to becoming mentally ill, but who are repeatedly violent following the onset of illness; and (3) Type III offenders (‘late late starters’, or LLS), who suffer from a chronic SMI, but who exhibit no aggression until one or two decades after illness onset, when they commit a single and serious violent offense often against someone caring for them. Whereas the violence witnessed in Type I offenders is thought to be influenced by specific genes conferring vulnerability for both early conduct problems and SMI, Type II and III offenders may be more influenced by post-illness neurological changes, including those caused by illness, substance misuse and psychotropic medication (Hodgins et al., 2014).
A small number of studies have investigated ES and LS subgroups on a number of dimensions (see Table 1), lending support to the existence of distinct subgroups showing varying trajectories to violence. Unfortunately, ES and LS groups have not been consistently operationalized across studies, and just one study (Van Dongen et al., 2014, 2015) has investigated the LLS group. One approach has been to define the groups on the basis of whether the first incident of offending occurred before (ES) or after (LS) 18 years of age (Hodgins and Janson, 2002; Laajasalo and Hakkanen, 2005; Pedersen et al., 2010b; Tengström et al., 2001) or whether or not they had a diagnosis of conduct disorder prior to age 15 (Mathieu and Côté, 2009; Sánchez-SanSegundo et al., 2014). A second approach defines ES as those with an age of first arrest or violence which is less than the age onset of their SMI, and vice versa for the LS (Jones et al., 2010; Kooyman et al., 2012; Taylor, 1993; Van Dongen, 2014, 2015). This latter approach is arguably more developmentally meaningful, being sensitive to the interrelationship between the age onset of illness and offending.
A summary of results from previous studies that have examined differences between early and late starters.
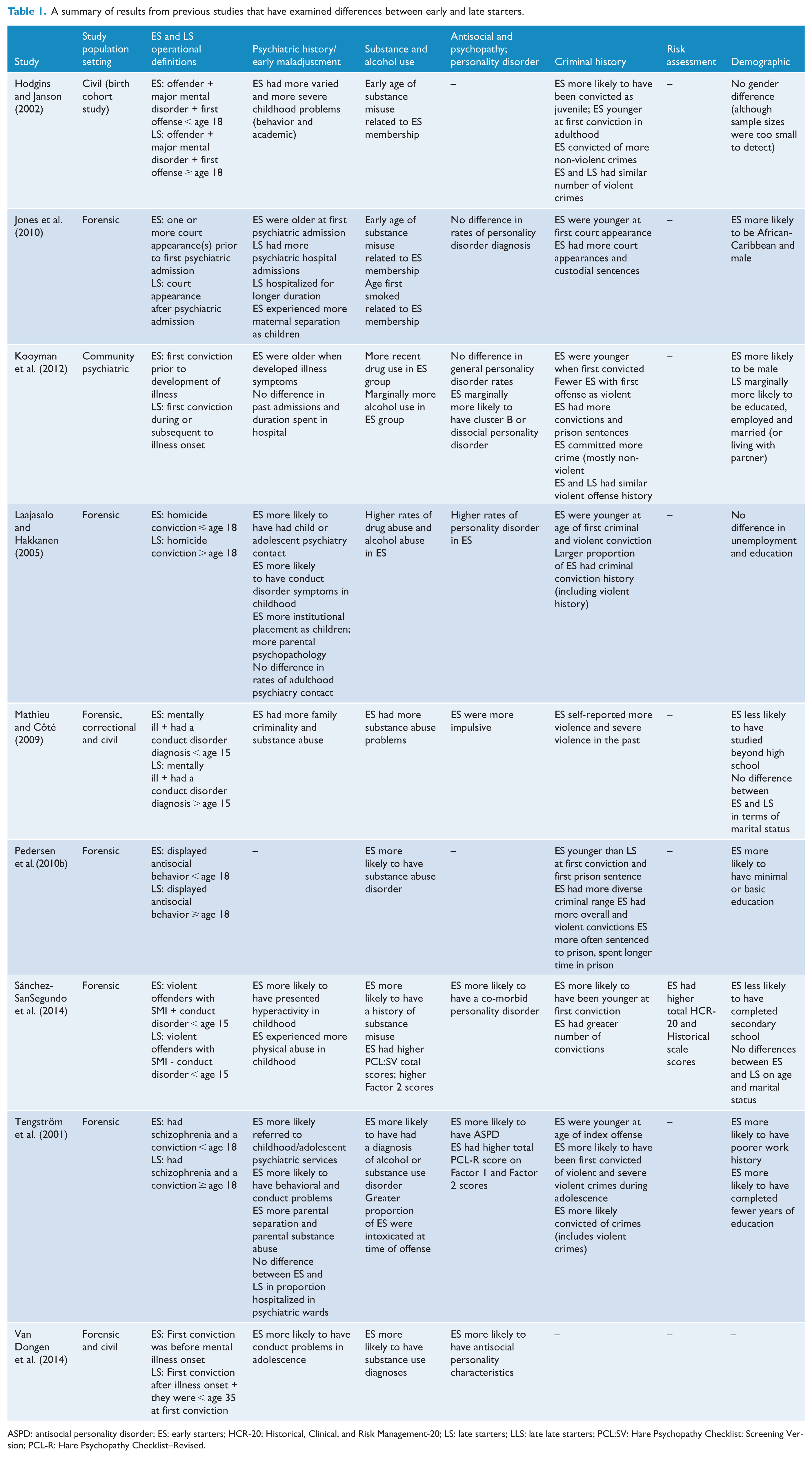
ASPD: antisocial personality disorder; ES: early starters; HCR-20: Historical, Clinical, and Risk Management-20; LS: late starters; LLS: late late starters; PCL:SV: Hare Psychopathy Checklist: Screening Version; PCL-R: Hare Psychopathy Checklist–Revised.
Van Dongen et al. (2014, 2015) studied the LLS group in a sample of forensic inpatients based on the timing of their first offense vis-à-vis the onset of psychosis (ES = offending before onset; LS and LLS = offending only after onset), as well as age (LS < 34 years old; LLS > 34 years old). Each group was compared with civil psychiatric non-offenders within the same community. The authors found that LLS comprised a small proportion of their sample (7%) and that substance misuse was significantly less likely among LLS compared to ES and non-offenders with schizophrenia. Although still evident in both ES and LS, persecutory delusions were most strongly associated with membership in the LLS group, while the ES group had more antisocial personality traits, conduct problems in adolescence and substance use problems (Van Dongen et al., 2014). LS were not compared to LLS on these latter dimensions. The authors concluded that there are more similarities than differences between LS and LLS and inferred that offending in these two groups is associated with positive symptoms (particularly delusions) but not with antisocial traits as in ES.
Taken together, the research in Table 1 has established that ES, as compared to LS, show earlier behavioral problems and greater adversity in childhood, greater criminal involvement and higher rates of antisocial personality disorder (ASPD) and substance misuse. They are more likely to be male and less educated than LS. Differences in the onset and severity of psychiatric problems are less clear; it may be that LS developed psychiatric problems at an earlier age and had more severe psychiatric issues as evidenced by more frequent hospitalizations. Research regarding whether LLS exists as a third subgroup is limited, as well as how this group may differ from ES and LS.
Aims of the study
This study investigates whether discrete subgroups of forensic psychiatric patients exist based on the age onset of SMI and offending. Subgroups were constructed based on the relative timing of SMI and criminal contact, and we investigated whether evidence of a third subgroup of SMI offenders, the LLS, appears in this sample. Building on existing research and theory, we conducted direct comparisons on specified sociodemographic, clinical, legal, offense- and risk-related variables between the three subgroups. We hypothesize that the ES group will have more offenses, although not necessarily more serious offending, and are likely to show more antisocial personality traits and have higher rates of substance misuse than both the LS and LLS groups. We hypothesize that the LLS group will have more social stability but a higher severity of offending than the ES and LS groups and will be more likely to offend against a caregiver or family member.
Method
Study design and participants
Data were drawn from the forensic program at the Centre for Addiction and Mental Health (CAMH) in Toronto, Ontario, Canada, one of the largest providers of forensic psychiatric services in the country. Details of every patient enrolled into the program from 2011 to 2012 (N = 434) were collected, representing approximately 30% of individuals in Ontario adjudicated Unfit to Stand Trial (UST) or Not Criminally Responsible on account of Mental Disorder (NCRMD). The Ontario Review Board (ORB) oversees all people found UST or NCRMD and reviews the status of every person under its jurisdiction on an annual basis. For each annual hearing, a psychiatric report is provided and the ORB hears evidence and produces its own Reasons for Disposition. These two documents, the psychiatric report and the Reasons for Disposition, were used to populate the patient registry.
Of the 434 patients in the registry, this study included only those with a diagnosis of a psychotic disorder (e.g. schizophrenia, schizoaffective disorder, delusional disorder) and who committed a violent index offense or who had a previous violent charge or conviction (N = 348). Of these, 116 were excluded due to missing data related to age onset of illness and offending, resulting in a final sample of 232. Chi-square and analysis of variance (ANOVA) were run to compare missing versus non-missing cases on age, sex, schizophrenia diagnosis and whether the index offense was violent. We found no significant differences except for age (Mmissing = 47.4, Mnon-missing = 42.4, F = 14.14, p < 0.01), suggesting that the current sample may be missing some older patients.
Procedure
A coding scheme and manual were developed, containing all relevant sociodemographic, clinical, legal and risk-related variables. Two research analysts (RAs) were trained and inter-rater reliability was established by examining agreement between the RAs and a doctorate-level researcher (T.G.) who developed the measures. Good inter-rater reliability was achieved for all variables (intraclass correlation coefficient [ICC1] > 0.75 [Kappa coefficient for categorical variables]). Cases were coded using information found in the most recent psychiatric report and Reasons for Disposition.
Measures
Operational definitions of key variables used in this study are described below.
Early maladjustment
This was captured using the early maladjustment item on the Historical, Clinical, and Risk Management-20 (HCR-20) (Webster et al., 1997). This risk factor is rated on a 3-point scale (0, 1 and 2) and includes victimization experiences, witnessing violence, conduct problems and other maltreatment during childhood.
Age at first psychiatric symptoms
This was based on self- or collateral report. Symptoms included positive symptoms of psychosis (e.g. delusions, hallucinations) and mood symptoms such as depression or anxiety.
Age of first hospitalization for psychiatric reasons
This variable included general hospital, civil psychiatric or forensic admissions, encompassing emergency, short-term or long-stay admissions.
Psychiatric disorders
The most recent clinical diagnoses made by the treating psychiatrist were coded. Substance abuse or dependence disorders were not distinguished by the specific substance misused (e.g. cannabis, cocaine, opiates). Diagnoses were based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) (American Psychiatric Association, 1994).
Substance or alcohol abuse
Based on self-, collateral or clinician report, abuse of alcohol or drugs (before and after age 18) was coded as present when there was indication that use had impaired the patient’s socio-occupational function. In addition, dependence or abuse after age 18 was coded as present when there was a formal diagnosis of alcohol or substance abuse or dependence.
Number of previous charges and convictions
Age at first arrest, previous charges and convictions are included in psychiatric reports and obtained through the Canadian Police Information Centre (CPIC). For a small number of cases, CPIC information was not available, and so previous legal history was based on self-report or collateral (parent/family) information. Information pertaining to juvenile arrests and convictions is not typically included in CPIC reports.
Index offense
This included the criminal offense(s) for which the patient was found UST or NCRMD. Offenses categorized as violent included assault, sexual assault, murder, attempted murder, kidnapping, reckless driving, threatening, robbery, weapons charges and criminal harassment. Offenses that were considered severely violent included murder, attempted murder and/or aggravated assault.
Index offense victim
Ample detail about the index offense(s) is provided in police synopses and included in ORB decisions and psychiatric reports. Victims were defined as individuals directly affected by the offense(s).
Risk assessment measures
The HCR-20 is a 20-item violence risk assessment scheme for use with adults who have a history of violence as well as mental illness and/or personality disorder. Items appearing on the HCR-20 are grouped thematically into historical/static risk factors, clinical/current concerns and future-oriented/risk management variables and are coded on a 3-point scale of 0 (not present), 1 (possibly/partially present) and 2 (definitely present). After indicating the presence/absence of the 20 items, a summary risk judgment is generated (low, moderate or high). The Historical scale represents largely static risk factors (e.g. ‘risk status’; Douglas and Skeem, 2005), whereas the Clinical and Risk Management scales include dynamic factors amenable to intervention. There is substantial evidence attesting to the HCR-20’s reliability in a range of settings (e.g. Douglas et al., 1999; McNiel et al., 2003; Pedersen et al., 2010a), and it is found to be a robust predictor of future violence in general psychiatric (Douglas et al., 1999), forensic psychiatric (Douglas et al., 2003; Gray et al., 2011) and correctional populations (Douglas et al., 2005).
The Hare Psychopathy Checklist–Revised (PCL-R) is a 20-item measure designed to capture the interpersonal, affective and behavioral features of psychopathy. Each item is scored on a 3-point scale of 0 (not present), 1 (present to some extent, or with exceptions) and 2 (definitely present) and may be grouped into two factors representing interpersonal/affective traits (Factor 1) and deviant/criminal behavior (Factor 2). The PCL-R has demonstrated excellent reliability (Hare, 2003) and validity for future violence and delinquency (Hemphill and Hare, 2004; Salekin et al., 1996).
Subgroup classification
ES were defined as patients for whom the age at which they first experienced psychiatric symptoms was greater than the age when they were first arrested (n = 59). LS were defined as those whose age of first known psychiatric symptoms was less than or equal to the age when they were first arrested. This group (n = 173) was then subdivided into two subgroups: those who had suffered fewer than 10 years of mental illness before their first arrest and who were younger than 37.5 years at the time of their first offense (LS; n = 154), and those who experienced 10 or more years of illness duration before their first arrest and who were 37.5 years or older when they were first arrested (LLS; n = 19). The duration of 10 years was used as a proxy for chronic mental illness and was the 75th percentile of illness duration within the 173 LS cases. The age of 37.5 years was used to align with Hodgins (2008), who described LLS as typically being in their late 30s or early 40s.
Statistical analyses
One-way ANOVAs were used to compare ES, LS and LLS subgroups on continuous demographic, clinical, legal and risk-related variables. Tukey’s post hoc tests were applied to examine comparisons between the three subgroups when the F-statistic was significant. A chi-square analysis was conducted to evaluate subgroup differences on categorical variables. If the chi-square statistic was significant, standardized residuals were examined to determine which group showed significantly different proportions from that which was expected. A 0.05 significance level was applied and the Benjamini–Hochberg multiple comparison correction was used to control for false discovery rates for independent tests (Benjamini and Hochberg, 1995). All analyses were conducted using IBM SPSS Statistics 20 for Windows.
Results
Patient characteristics
The majority (88%) of the study sample was male, with a mean age of 43.19 years (standard deviation [SD]= 11.40). Of the patients, 34% were previously or currently married, and 11% were married at the time of the index offense. In all, 31% had children. Most were diagnosed with schizophrenia (79%) and smaller proportions with schizoaffective disorder (12%), delusional disorder (4%) and other psychotic disorders (6%). A total of 55% were diagnosed with a substance use disorder. Approximately 23% of the sample was diagnosed with a personality disorder, 28% of whom had ASPD and 65% of whom had personality disorder not otherwise specified (NOS) or with mixed traits. 1 Mixed traits were typically antisocial, narcissistic and/or borderline (cluster B) traits and less often passive-aggressive, dependent or histrionic traits. The mean age at first psychiatric hospital admission was 26.35 years (SD = 9.44).
The mean age at first arrest was 25.75 years (SD = 11.16). In all, 22% had no previous charges, 10% had one previous charge and 43% had two or more previous charges (note: prior charges data were missing for 25% [n = 58] of the sample). A total of 38% had no previous convictions, 10% had one previous conviction and 48% had two or more previous convictions. Most of the index offenses (87%) were of a violent nature, with assault being the most common. Regarding severe violence, 10% of the sample had committed murder, 12% committed aggravated assault and 5% attempted murder.
Overall, 25% (n = 59) were classified as ES, 66% (n = 154) were classified as LS and 8% (n = 19) were deemed LLS, according to the definitions above. Table 2 presents the differences between the subgroups with respect to the specified demographic, clinical, legal and risk-related variables.
Subgroup means, standard deviations, proportions and post hoc between-group comparisons on demographic, clinical, legal and risk factors.
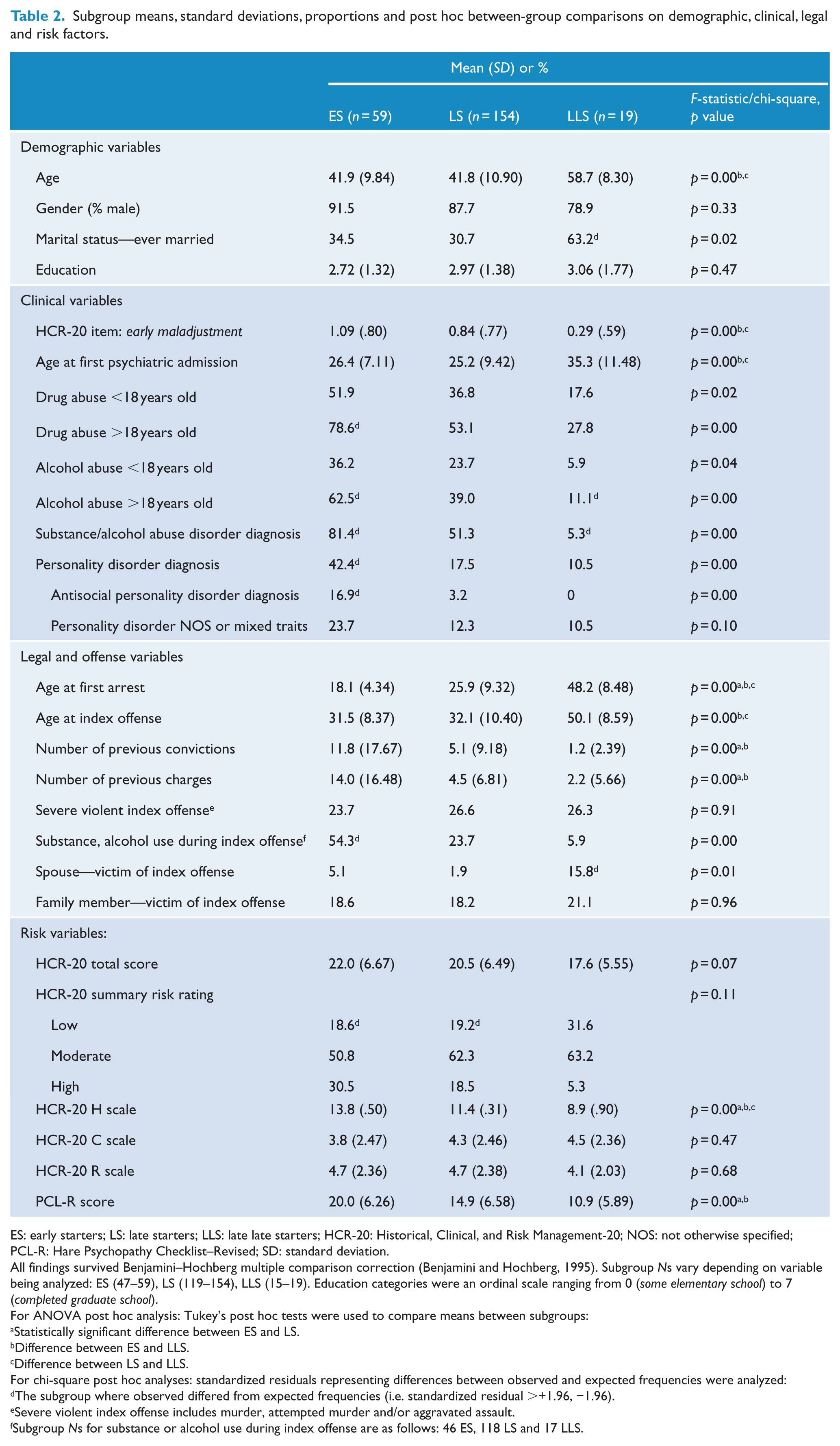
ES: early starters; LS: late starters; LLS: late late starters; HCR-20: Historical, Clinical, and Risk Management-20; NOS: not otherwise specified; PCL-R: Hare Psychopathy Checklist–Revised; SD: standard deviation.
All findings survived Benjamini–Hochberg multiple comparison correction (Benjamini and Hochberg, 1995). Subgroup Ns vary depending on variable being analyzed: ES (47–59), LS (119–154), LLS (15–19). Education categories were an ordinal scale ranging from 0 (some elementary school) to 7 (completed graduate school).
For ANOVA post hoc analysis: Tukey’s post hoc tests were used to compare means between subgroups:
Statistically significant difference between ES and LS.
Difference between ES and LLS.
Difference between LS and LLS.
For chi-square post hoc analyses: standardized residuals representing differences between observed and expected frequencies were analyzed:
The subgroup where observed differed from expected frequencies (i.e. standardized residual >+1.96, −1.96).
Severe violent index offense includes murder, attempted murder and/or aggravated assault.
Subgroup Ns for substance or alcohol use during index offense are as follows: 46 ES, 118 LS and 17 LLS.
Demographic differences between subgroups
There were no differences in the gender composition or educational attainment of the subgroups. LLS were significantly older than both ES and LS (F(2, 229) = 22.90, p < 0.01), and a significantly larger proportion of LLS were previously or currently married, χ2 (2, N = 227) = 7.89, p < 0.05.
Clinical differences between subgroups
A larger proportion of ES had substance or alcohol use disorders as compared to LLS, χ2 (2, N = 232) = 36.43, p < 0.01. Similarly, more ES and fewer LLS had alcohol concerns in adulthood, χ2 (2, N = 207) = 15.85, p < 0.01, and more ES had drug concerns in adulthood, χ2 (2, N = 219) = 17.83, p < 0.01. More ES were diagnosed with a personality disorder, χ2 (2, N = 232) = 16.22, p < 0.01, and with ASPD specifically, χ2 (2, N = 232) = 14.67, p < 0.01, than LS or LLS. When ASPD was excluded, results indicated no significant differences between the subgroups, suggesting that the higher rate of personality disorder in ES was due to ASPD specifically. Subgroup proportions did not differ with respect to personality disorder NOS or personality disorder with mixed traits. Subgroups differed on the age when they were first admitted to a hospital for psychiatric problems, F(2, 218) = 9.79, p < 0.01, with LLS being significantly older than both ES and LS. Finally, LLS scored significantly lower on the HCR-20 item early maladjustment as compared to ES and LS, F(2, 219) = 7.20, p < 0.01.
Legal differences between subgroups
ES were significantly younger upon their first arrest, compared to LS and LLS, F(2, 229) = 95.42, p < 0.01. LLS were also significantly older than LS. ES were found to have a greater number of previous charges (F(2, 170) = 15.49, p < 0.01) and convictions (F(2, 219) = 8.84, p < 0.01) compared to LS and LLS. LLS were also found to be significantly older than ES and LS at the time of the index offense, F(2, 229) = 31.94, p < 0.01. A significantly larger proportion of ES had substances or alcohol involved in the index offense(s): χ2 (2, N = 181) = 19.97, p < 0.01. The frequency of severe violence committed during the index offense did not differ across the subgroups. However, a larger proportion of LLS had victims who were spouses, χ2 (2, N = 232) = 9.00, p = 0.01. No other differences emerged with respect to the frequency of offenses for which victims were family members.
Risk differences between subgroups
Violence risk assessment scores based on the HCR-20 indicated a trend toward ES having higher total risk scores than LLS, F(2, 195) = 2.78, p = 0.07. ES also had significantly higher scores on the Historical scale, F(2, 187) = 13.51, p < 0.01, followed by LS and then LLS, while no subgroup differences emerged on the Clinical and Risk Management scales. Subgroup proportions across the summary risk judgments did not reach statistical significance; however, a larger proportion of LLS (32%), as compared to ES (19%) and LS (19%), were deemed low risk. ES scored higher on the PCL-R compared to both LS and LLS, F(2, 164) = 13.24, p < 0.01.
Discussion
This study investigated whether discrete subgroups of forensic psychiatric patients could be identified based on the age onset of SMI and offending and whether these subgroups differed on the basis of sociodemographic, clinical, legal and risk-related variables. Employing a reliable operational definition of the timing of illness and offending onset, we investigated variables examined in prior studies and included the additional dimension of structured risk assessment which has only been investigated in one other study (Sánchez-SanSegundo et al., 2014). In addition, alongside Van Dongen et al.’s (2014, 2015) studies, this is the second study to examine the existence of a third subgroup, proposed by Hodgins (2008), the LLS.
Our findings revealed important differences between ES and LS. Substance use problems, including a current diagnosis of substance or alcohol abuse disorder, substance or alcohol usage during the index offense, as well as substance problems in adolescence, were all more prevalent in ES, consistent with studies that have identified more severe substance issues in this group (Hodgins and Janson, 2002; Jones et al., 2010; Kooyman et al., 2012; Laajasalo and Hakkanen, 2005; Mathieu and Côté, 2009; Pedersen et al., 2010b; Tengström et al., 2001; Van Dongen et al., 2015). As hypothesized, personality disorders, including ASPD and psychopathic traits, were more prevalent in the ES group. Almost one-third of patients with a personality disorder in this sample had ASPD, while many others had personality traits in the cluster B domain. This may reflect core problems in impulse control and emotion regulation that cut across different diagnoses and are prevalent in this sample. Other studies have similarly reported higher levels of impulsivity (Mathieu and Côté, 2009), psychopathic traits (Tengström et al., 2001) and cluster B diagnoses (Kooyman et al., 2012) in ES compared to LS.
We found that ES were younger when they were first arrested and had incurred a greater number of charges and convictions than LS. This is consistent with our hypothesis and prior studies demonstrating an earlier onset and higher prevalence of criminal offending in ES compared to LS (Jones et al., 2010; Kooyman et al., 2012; Laajasalo and Hakkanen, 2005; Mathieu and Côté, 2009; Pedersen et al., 2010b; Tengström et al., 2001). Notably, the mean age of first arrest in ES (18) was higher than what has been reported previously (Jones et al., 2010; Kooyman et al., 2012; Laajasalo and Hakkanen, 2005), likely owing to our reliance on adult criminal records. However, current results may also be viewed as a conservative test of the age differences among the subgroups, given the existing literature to suggest that ES have more arrests occurring prior to age 18 (e.g. Hodgins and Janson, 2002). That is, if juvenile records had been obtained, we might expect subgroup differences in the age of first criminal contact to be even greater in magnitude. In contrast, the presence of a severe violent index offense did not significantly differentiate the subgroups, a null hypothesis that was reported elsewhere (Hodgins and Janson, 2002; Kooyman et al., 2012) and likely due to the high rate of violent offenses (87%) across our sample as a whole. Thus, while general criminal offending seems to be an important distinguishing variable, both subgroups may have a similar propensity toward severe violent offending.
Similarly, ES were found to possess a greater number of static/historical risk factors for violence, as well as increased levels of psychopathic traits. The higher risk status among ES may partly be a function of how this subgroup is defined (i.e. as having an earlier age onset of offending, as measured against illness onset), but also reflects that ES are more likely to have general markers of antisociality in their background, including ASPD, relationship and employment instability, early childhood maladjustment, substance use problems and extensive criminal histories. In contrast to static/historical markers of risk, the subgroups did not differ with respect to the dynamic risk subscales on the HCR-20. Sánchez-SanSegundo et al. (2014) found a similar pattern of HCR-20 Historical and PCL:SV scores to our results, but they found that dynamic risk was lower in the conduct-disordered (i.e. ES) subgroup. As both this study and the current one are of forensic populations, the observed differences in dynamic risk may be related to the point in recovery when the HCR-20 was measured. We also found few differences between ES and LS with respect to age, gender, marital status and education. This is in contrast to other studies which have suggested that ES tend to be male and achieve lower educational attainment (Kooyman et al., 2012; Mathieu and Côté, 2009; Pedersen et al., 2010b; Tengström et al., 2001).
Current results replicate and extend the ES and LS profiles that have emerged from previous research and highlight similarities between the ES subgroup and the LCP offenders identified by Moffitt (Moffitt, 2006; Moffitt et al., 2002). Given their elevated risk status and frequency of substance use disorders, we can hypothesize that the offenses committed by ES are motivated more frequently by antisocial attitudes and peers, as well as behaviors related to substance and alcohol misuse, than directly by symptoms of illness. It is possible then that the ES/LS distinction is at least in part a separation into broadly differing motivational groupings of people with psychosis who are violent (Hodgins, 2008; Penney et al., 2013). However, this requires further research involving inquiry into patient motivations for offending and how reports of motivation vary across subgroups.
Due to the high level of criminogenic need in ES, rehabilitation efforts must go beyond simply treating active symptoms of SMI. Furthermore, the higher frequency of ASPD and other characterological problems may impede responsivity to treatment and necessitate a more intensive and multisystemic approach. Dialectical behavior therapy may be a particularly promising approach for this group, as it is well suited to deal with responsivity barriers linked to personality pathology and is effective in addressing problems related to impulse control and emotion regulation. This is not to say that addressing criminogenic needs is not relevant in other patients (indeed, half of the LS subgroup in this sample was diagnosed with a substance use disorder and had, on average, five previous convictions), but that the chronicity and scope of the needs may be more substantial in ES and may require more intensive resources to address them adequately. Furthermore, although ES and LS groups share certain risk and needs factors, their underlying contribution to violence and offending may differ. The elevated proportion of LS with substance use is consistent with the position that offending in LS is associated with neurological changes brought on by illicit drug use following illness onset (Hodgins et al., 2014). In contrast, for ES, the role of substance misuse in their criminality may be predominantly instrumental and part of a larger risk scenario characterized by antisocial lifestyle and peer affiliation.
In contrast to the ES/LS distinction, it is less clear whether LLS represent a discrete subgroup within the SMI offender population. Our findings suggest that the LLS subgroup represents an exemplar (i.e. ‘amplified’ version) of LS: if LS were higher (or lower) on some trait or behavior compared to ES, LLS were that much higher (or lower) than LS. For example, LLS were rated lower on early maladjustment, showed even lower rates of substance misuse, were older than LS at age of first arrest and at the time of the index offense, and showed the lowest risk status and summary risk judgments on the HCR-20. Furthermore, no one in the LLS subgroup was diagnosed with ASPD. Although not statistically significant, LLS had fewer criminal charges (mean = 2) and convictions (mean = 1) and lower PCL-R scores compared to LS, who were significantly less psychopathic and engaged in less criminal offending compared to ES. Further differences emerged in line with Hodgins’ (2008) hypothesized profile of LLS: namely, these patients were more likely to be married, be older when first admitted to hospital for psychiatric reasons and more likely to have a spouse as victim.
Older age at first psychiatric admission may appear counter-intuitive if we consider LLS to be chronic sufferers of SMI. In fact, other studies have shown that LS had more hospital admissions and were younger at illness onset and first psychiatric admission, compared to ES (Jones et al., 2010; Kooyman et al., 2012; Tengström et al., 2001). Based on this, we might expect LLS to be even younger when their symptoms emerged. However, the finding that these patients were older at first admission suggests that mental illness starts later in life, allowing more time to establish structure and stability in one’s life prior to the illness taking hold. Thus, they have more organized and stable lifestyles, with a spouse, and possibly symptoms which are less bizarre, but more insidious in terms of onset and delusional in nature. Van Dongen et al. (2015) found a stronger association of persecutory delusions and violence in the LLS, possibly reflecting motivations for offending that are more directly linked to illness in this group (e.g. violence in an attempt to reduce the threat associated with persecutory delusions).
Results of this study need to be considered in light of certain limitations. First, there were missing data on key variables which decreased our sample size and reduced power in some analyses. This is particularly the case for the LLS subgroup (n = 19), as we suspect that some of the missing cases would have been classified into this subgroup. Furthermore, the manner in which we created the subgroups may be a limitation. The method of imposing pre-selected criteria to divide a sample into subgroups does not allow for the grouping of features as they might occur naturally in a sample. As such, an important direction for future studies is to employ person-based statistical approaches (e.g. cluster analysis, latent class analysis) to more effectively capture the subgroups that may exist in this population.
A third limitation is that our data were cross-sectional in nature, and so there was no opportunity to examine the manner in which different risk factors and pathways to violence may unfold in real time. Future research should examine subgroups prospectively with an emphasis on symptoms, thoughts (e.g. content of delusions), behaviors and motivations around the time of an offense in order to study more proximal influences on violence. Finally, we used just a single item from the HCR-20 to indicate negative experiences in childhood, which is necessarily less reliable than if a measure incorporating multiple items was used.
Overall, we found support for distinct subgroups of people with SMI and a history of violence, and specifically for the ES and LS profiles. There is also some evidence for a LLS subgroup characterized by individuals whose psychiatric symptoms arose later in life and who were more likely to be married and commit an offense against a spouse. The emerging profile of LLS individuals requires further investigation in order to substantiate Hodgins’ (2008) theoretical framework. A better understanding of the characteristics of these subgroups, including their differing pathways to and motivations for violence, has important clinical implications since individuals with diverse risk profiles and motives will have correspondingly different treatment needs to manage risk and prevent future offending.
Footnotes
Acknowledgements
Thanks are due to Ms Stephanie Fernane, MA, for her significant contribution to data collection for this study. We also thank Ms Rida Anmol, BSc, for her contribution.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.