
Abstract
For more than 50 years psychiatrists and trainees in the New Zealand Public Health system have been required to allocate coded diagnoses for their patients’ disorders according to the extant version of the International Classification of Diseases (ICD). Over the middle of last century clinical diagnostic practice most often used textbook-derived diagnostic labels with conversion on discharge by either clinicians or clerical coders to the ICD codings. The development of a multiaxial approach to classification, by the World Health Organization (WHO) in child psychiatry in the 1950s and the American Psychiatric Association (APA), in the third edition of the Diagnostic and statistical manual of mental disorders (DSM-III) published in 1980[1], were attempts to combine the advantages of a diagnostic conclusion with the necessity to better inform management planning by including a broader range of patient information. With the advent of the DSM-III, clinical diagnostic practices became heavily dependent on using that system with much less reference to textbook-derived categories and criteria. At present the WHO and the APA are both in the relatively early stages of developing their next versions, ICD-11 and DSM-V, respectively. The current versions (ICD-10 and DSM-IV) have grown enormously from their predecessors of the first part of the last century [2, 3]. Psychiatric research, and the peer-reviewed literature, are constantly seeking refinements in our understanding of pathogenesis of the disorders we treat, with implications for the diagnostic categories that are used. These are most often particularly centred around the best ways of defining disorders, the boundaries between disorders, and sometimes developing new labels. There are also occasional thoughtful reviews or suggestions for the exploration of more fundamentally different approaches [4–9]. Mezzich has argued that there is a need to shift from ‘what’ to ‘how’, from reliability of symptomatology to a focus on outcomes. The capacity to elicit, organize and postulate as to the interrelations between the pieces of relevant information gathered on a variety of axes requires that the clinician integrate dimensional and categorical approaches [10, 11].
These researched and opinion-based developments, and the enormous increase in detail and complexity of the official classificatory systems, have occurred largely in the absence of any systematic collection of the views of the principal users, namely practising psychiatrists.
This paper reports on a project that sought to ascertain the views of a sample of New Zealand psychiatrists and trainees on some of the more global attributes of our presently used systems.
Method
The names, vocational activities, and official addresses of all New Zealand doctors registered with the Medical Council of New Zealand are public information. A list was compiled of all those practising as psychiatrists, or trainee psychiatrists, which formed the subject pool.
A questionnaire (Appendix I) was developed and modified through several iterations of New Zealand peer exposure, but particularly through the New Zealand National Committee of the Royal Australian and New Zealand College of Psychiatrists (RANZCP). It was mailed out to the 542 given names and addresses. A stamped, return address envelope was included with the questionnaire. Two weeks after the initial mailing a reminder was sent to all those for whom an email address was available (450).
The current view of the New Zealand Ethics Committees is that in such situations, with anonymous non-personal questionnaires, completion implies consent (G. Mellsop: personal communication, 2005).
One month after the initial mailing, data entry was commenced with Data Entry Builder Software for Windows (SPSS Data Entry Builder 4.0, Chicago, IL, US). The data was double-entered to ensure the best quality for the analysis.
The analysis was performed using SPSS for Windows 14.0 (SPSS). Trends were analysed and also discussed when breaking down the data by demographic information, such as gender, age and area of specialty (child and adolescents; adults; older adults; forensic; addictions; other).
Results
A total of 235 completed questionnaires were returned, which equates to a 43% response rate. The completion rates of returned questionnaires were high, with more than 90% for most of the questions and for some, 99%.
It was lower for question 6, which asked respondents to rank from 1 to 4 the Axes’ usefulness; 89.7% answered that question. The part of question 9 dealing with the ICD-10 also had more missing values, with 86.4% and 84.1% of questionnaires answered respectively for the ICD-10–clinical and ICD-10–functional questions.
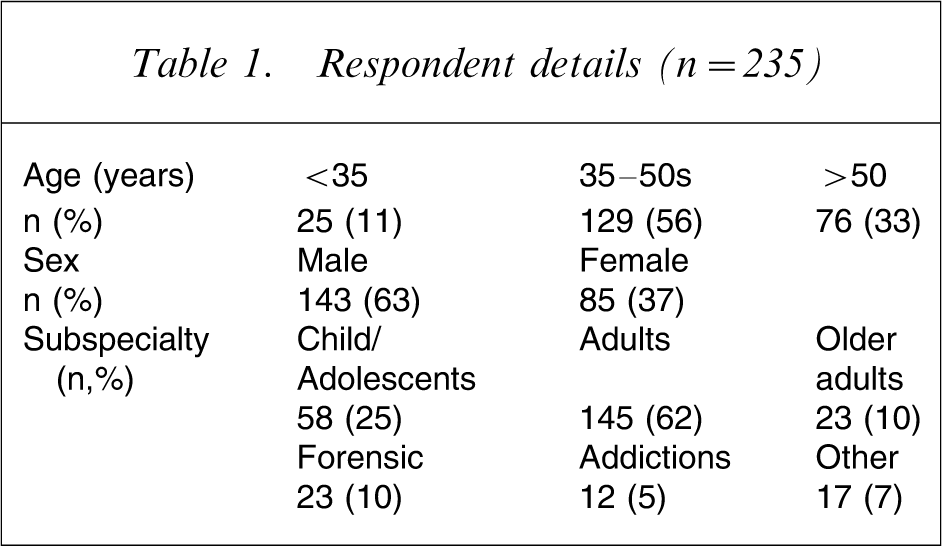
The minimal data collected on demographic characteristics of the respondents are reported in Table 1. This shows that two-thirds were male and the respondents were distributed throughout the major subspecialty areas.
Respondent details (n = 235)
Approximately three-quarters of the respondents included commentary to explain their use of either system or the axial parts of their preferred system. (Tables 2 and 4).
New Zealand respondents using current classification options in their clinical practice
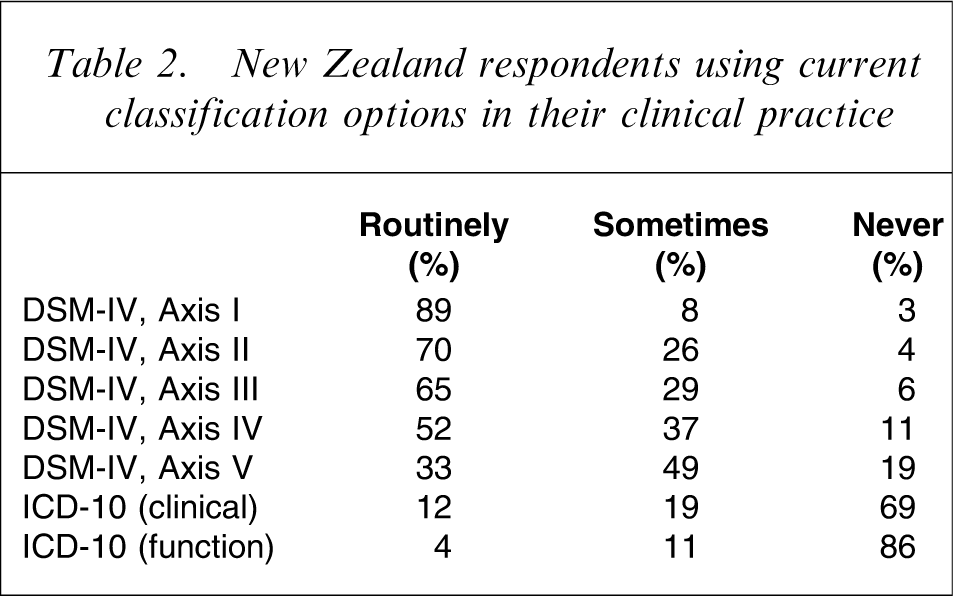
Overwhelmingly the major reason for using the DSM system was that it had been the basis of their training as psychiatrists. It was also the system widely used in their textbooks. Two other very commonly given reasons were that their employer health provider systems (including IT) were based on the DSM and, that because ‘everybody’ used it, communication was facilitated. The overwhelmingly common reason for not using ICD-10 was ‘unfamiliarity’. A few used ICD-10 because it was the official statistical system. A few did not like DSM because it lacked validity or they preferred to formulate than to diagnose. Many commented that in their view axis V was unreliable and lacked clinical applicability.
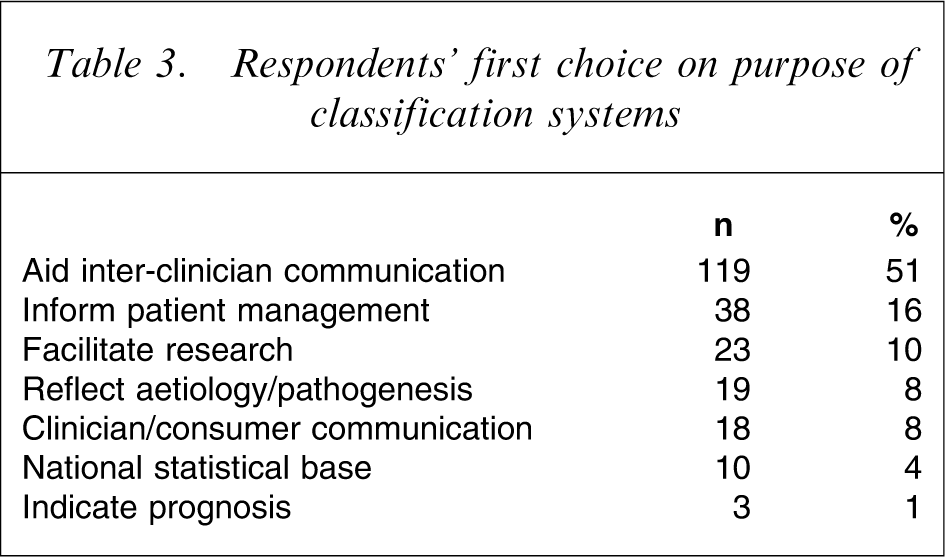
Respondents’ first choices for the purposes of a classificatory system are listed in Table 3.
Respondents’ first choice on purpose of classification systems
Analysis of subgroups of the respondents showed only minor differences. Gender did not appear to influence the responses to any of the questions. The over-51 age group were significantly (p = 0.04) less interested in reliability of interclinical communication than the remainder and were more interested in having the classification convey information about aetiology and clinical management plans. Analysis by area of practice indicated that this was particularly the view of those working in adult mental health services.
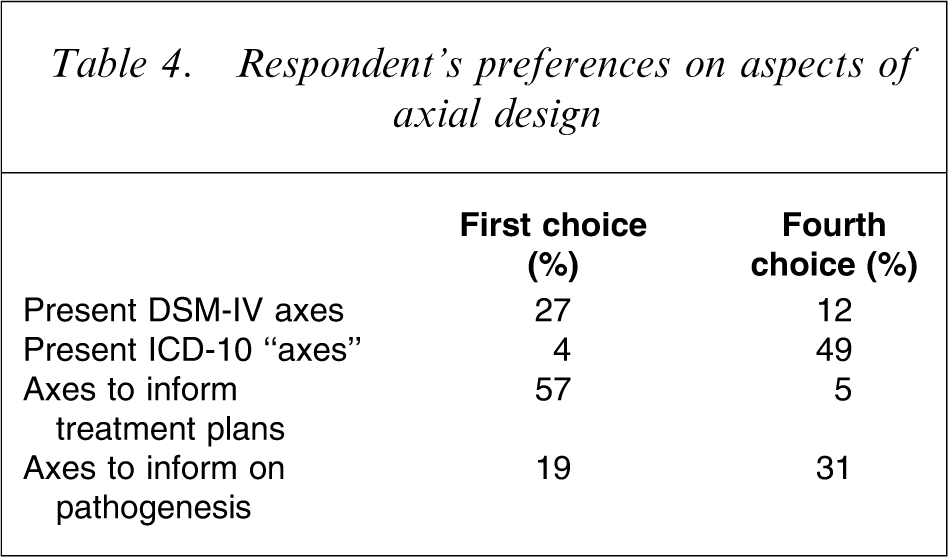
Question 8 asked respondents to list the qualities or attributes they need or want from a psychiatric classification. Respondents varied from recording nothing in this box to providing one to five different requirements. A core part of their reported needs reflected the same purposes as noted in Table 3. The three most prominent requirements were simplicity (of use), reliability and usefulness to guide treatment. Needs or wants recorded that had not been reflected in Table 3 included having a less rigid system allowing more individuality, flexibility to be useful in a variety of contexts, more emphasis on dimensions in some areas, a system that would be more valid and reliable over time, and broader (and fewer) categories.
Respondent's preferences on aspects of axial design
In response to question 5, opinions were evenly divided on whether a future classificatory system should convey information concerning causes, prognosis and treatment decisions (55%), or be separated into two, with one designed to facilitate clinical management decisions, and a second system to reflect cause/pathogenesis (45%).
Most respondents made no comment in question 10, in which they were asked to indicate if there were any specific diagnoses in DCM-IV or ICD-10 that they consider would be better moved to another section or removed. Three areas were referred to by 5–10% of respondents: post-traumatic stress disorder, personality disorders and impulse disorders. A variety of comments were made about these three areas. Additionally some raised concerns about comorbidities and overlap between clinical entities. Approximately 25 other disorders received one or two mentions in the 235 returned questionnaires. Of interest were the comments specifically about the lesser utility of the age-related disorders at both ends of the spectrum.
On the question of who are the legitimate users (Table 5), forensic psychiatrists were the only group to place greater emphasis on having the classifications used only by doctors or psychiatrists (35% vs 17%, p = 0.04). Older aged respondents also took that view (32% vs 13%, p = 0.004).
Respondents’ views on whom classificatory systems should be used by:
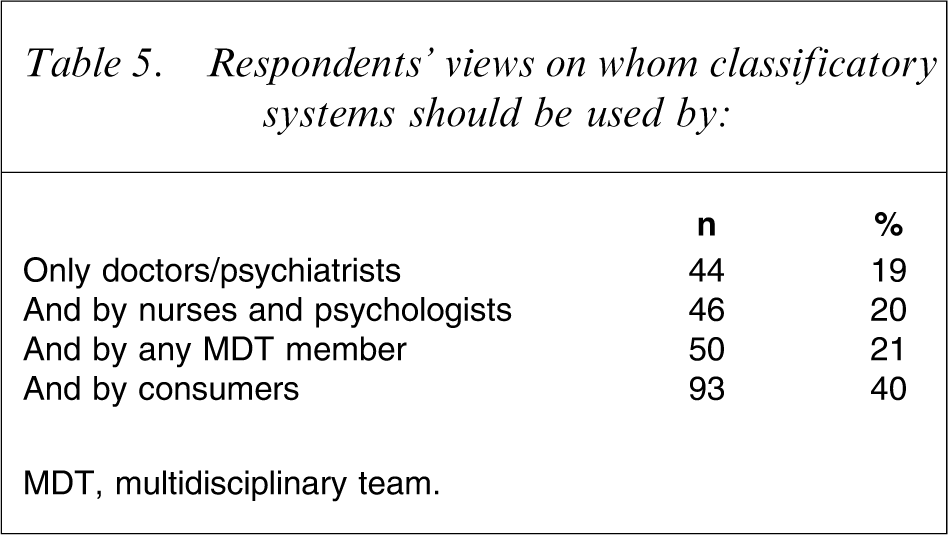
MDT, multidisciplinary team.
On a related question, 74% of the psychiatrists considered that general practitioners should use the same classification as the specialists. One-quarter took the alternative view that a modified, simpler system would be more appropriate for primary care.
Child psychiatric clinicians were much more strongly in favour of general practitioners using the same classificatory system as specialists (84% vs 70%, p = 0.02).
Using classificatory systems with more than 100 diagnostic options had the least appeal to psychiatrists working in adult mental health (16%) than for the remainder (27%, p = 0.04).
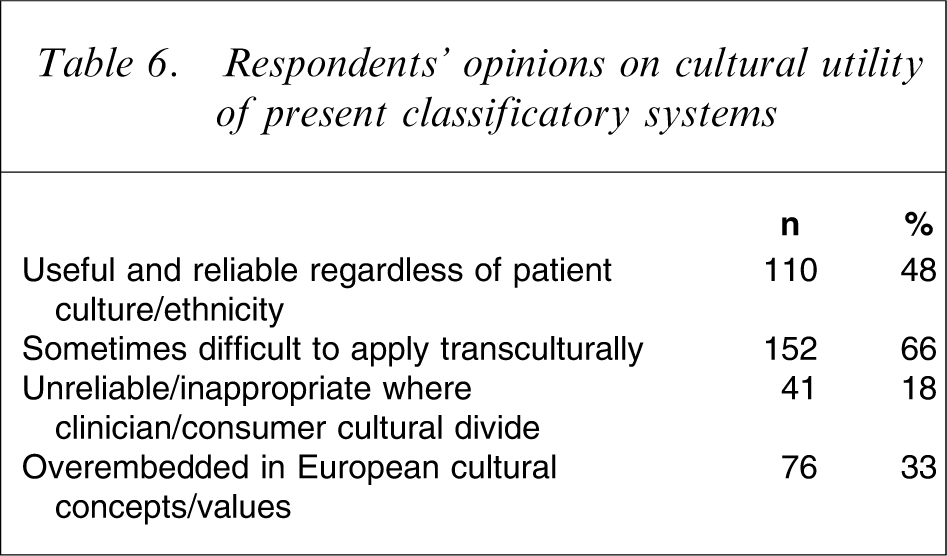
From a cultural point of view nearly half the respondents felt that the systems were universally useful, with 66% noting some difficulties in applying them transculturally (Table 6).
Respondents’ opinions on cultural utility of present classificatory systems
Discussion
The aforementioned results are based on the views of a large number of New Zealand psychiatrists and psychiatrists in training. It is likely that there would be a systematic bias influencing who would respond, in favour of those who are more interested in thinking about or commenting on issues to do with classification.
Particular uncertainties about the 43% response rates are due to the unknown number of New Zealand-registered psychiatrists who use a New Zealand address (tardily accessed) for Medical Council purposes and the number either out of office or on leave.
The results can be discussed in relation to two particular issues. First, the purposes of a classificatory system; and second, respondents’ views on the two most widely used.
The introduction to ICD-10 states ‘conditions have been grouped in a way that was felt to be most suitable for general epidemiological purposes and the evaluation of health care’ [12]. The classification of mental and behavioural disorders, chapter V, notes it ‘… is intended for general clinical, educational and service use’ [3].
The introduction to DSM-IV states: ‘The utility and credibility of DSM-IV require that it focus on its clinical, research and educational purposes… Our highest priority has been to provide a helpful guide to clinical practice. An additional goal was to facilitate research and improve communication of clinicians and researchers… and as an educational tool for teaching psychopathology (page xxiii)’ [2].
These last two goals appear to have been met, in the views of the New Zealand psychiatrists. These classifications can be argued to have reached a zenith of reliable interclinician communication, so that unlike Humpty Dumpty, when we use a word we all agree on what it means [13]. However, the value and validity of what is communicated appear more uncertain given that the only other purpose that gained >10% of their support was ‘to inform patient management’, which still only received a 16% vote. The New Zealand psychiatrists have become used to the idea that the present classificatory systems appear not to serve the purposes of explaining the pathogenesis, predicting the treatment response, or the prognosis. This is consistent with other New Zealand work in relation to treatment decisions [14, 15]. As those authors have noted, diagnostic-based clinical practice guidelines have enormous overlap, and clinicians’ resource-using clinical management decisions appear to be very little influenced by diagnosis.
The breadth of the responses elicited from the New Zealand psychiatrists is consistent with the breadth of the official stated purposes of these two major classificatory systems. However, there is some argument that having such comprehensive and diverse aims is at best unachievable, which makes the frequency of certain views from the New Zealand psychiatrists much more interesting. The frequency of their support for reliability and usefulness as a guide to treatment is far greater than for any of the other possible purposes.
A small number of respondents commented on the usefulness of the multiaxial approach in promoting a more holistic assessment. However, the very limited use of DSM axis V (global assessment of functioning) is surprising, given other literature that tends to be more critical of the clinical utility of axes III and IV. For instance studies focusing on validating the multiaxial approach have suggested that axis III is not properly used and is also under-utilized. This impacts on a clinician's ability to effectively assess impairment of function arising from the relationship between physical disorders and the axis I diagnosis. Yet capturing the information enhances treatment planning [16].
Whether or not the same classificatory approach should be used by clinicians other than psychiatrists is clearly a complex issue. The stance of DSM-IV on this is unclear, but there is the primary care version of ICD-10. The New Zealand psychiatrists do not appear to support that separation. The systematic views of general practitioners are not known. They may well take the view that psychiatrists do not know what is best for primary care clinicians [17].
The finding that only 48% of respondents thought that the classificatory systems are useful and reliable regardless of culture and ethnicity of clinician and patient could be influenced by the ethnicity of the respondent. At least in the New Zealand context, with its significant multiculturality of population and doctors and particularly strong influence of M
There was some support for one system as opposed to the current situation, and responses showed evidence that a major review of the systems is needed to make classification more clinically relevant and enhance clinical utility. There is a preference for a lot fewer categories to choose from. To set the vision for the next iteration of classification (e.g. ICD-11 and DSM-V) and maximize the value of the classificatory conclusions of a clinical assessment, to focus on patient management choices and planning would be a logical approach [18]. This might help significantly in the choice and structure of axes. The almost total dissonance between clinician use of DSM-IV and the official national use of ICD-10 is unhelpful.
Replication of this work in countries with totally different cultural contexts and further research examining the implications of some of these findings, would be important and timely given the imminent development of DSM-V and ICD-11. This is now happening in Brazil, Japan and Malaysia and is being planned in a number of other countries.