
Abstract
A growing body of evidence supports the efficacy of computerized cognitive behavioural therapy (CCBT). This technology has the potential to increase the capacity of mental health services, and to overcome some of the barriers to accessing mental health services, including stigma, traveling time for rural patients, treatment delays, and the low availability of skilled clinicians. This review discusses key issues around the implementation of CCBT in current mental health services, and summarizes recent evidence for the efficacy of CCBT in anxiety and depression. Many CCBT systems exist, and the evidence for each varies in quality and quantity. It is concluded that CCBT, particularly guided by a therapist, represents a promising resource. However, considerable work needs to be done to develop CCBT techniques that are appropriate to Australasian populations, acceptable to patients and clinicians, easy to use, and are clinically and cost effective. Suggestions are made for further research and useful website addresses are provided to assist clinicians in familiarizing themselves with CCBT.
Comparisons between the recent Te Rau Hinengaro: The New Zealand Mental Health Survey and its Australian counterpart revealed that New Zealand and Australian adults appear to share several important similarities. First, adults in the two countries have similar rates of mental disorders [1–3]. Second, anxiety disorders and major depression account for the majority of adults with mental disorders in Australasia. Third, these high-prevalence conditions are associated in each country with considerable disability [2, 4]. And fourth, it appears that no more than 40% of Australian or New Zealand adults with a mental disorder seek treatment from a mental health professional in a 12 month period [5, 6].
These statistics are of particular concern because there is ample evidence for the effectiveness of pharmacological and cognitive behavioural treatments (CBT) for the mood and anxiety disorders [7–9]. For example a recent review of meta-analyses of the efficacy of CBT indicated large effect sizes for unipolar depression, social phobia, panic disorder with/without agoraphobia, post-traumatic stress disorder, and generalized anxiety disorder [7]. Indeed, comparisons with pharmacological treatments indicate that CBT is more acceptable to patients [10], and has lower dropout rates [9]. Hence, there are many Australian and New Zealand adults living with a mental disorder that could, in principle, be treated [11].
Unfortunately, if all Australasian adults with a high-prevalence mental disorder actually sought treatment for their anxiety or depression, the increased demand would outstrip the service capacity of the mental health workforce in each country [11, 12]. This is particularly relevant outside major urban centres in Australia [13], with similar patterns likely in New Zealand. The restricted availability of CBT in particular is due to the considerable training and supervision required of practitioners and because of the treatment time required per patient. These issues are not, however, limited to Australasia. For example, the London School of Economics recently presented economic arguments for training 10 000 additional CBT therapists in the UK [14–16], noting that the cost of face-to-face CBT would repay itself in 1 month of regained earnings by a patient. Meanwhile, in Australia, attempts have been made to reduce this shortfall in capacity by recruiting and training additional mental health staff and by upskilling primary practitioners [17–19]. While such strategies are welcome, the shortfall continues.
One potential strategy for increasing the capacity of mental health services to provide CBT is the utilization of computerized CBT (CCBT). CCBT aims to provide structured sessions of CBT via computer with various levels of therapist contact. CCBT or similar computer education and training programs have already been widely used to help manage a range of health conditions including smoking cessation [20], headaches [21], weight loss [22], tinnitus [23], and physical activity [24].
Although attempts at translating features of psychological therapy into computer-delivered programs have occurred over at least four decades [25], recent studies have generally supported the potential utility of CCBT in the treatment of depression and anxiety disorders [26–30]. Clinicians, researchers, and planners of mental health services have also begun promoting the potential use of CCBT as an early intervention within a formalized stepped-care approach [11, 28, 31–39]. However, important questions about CCBT currently remain unanswered. This review summarizes recent outcome literature on the use of CCBT for treating anxiety and depression, and discusses issues relevant to the implementation of such programs in the Australasian environment.
What is CCBT?
For the purposes of this review CCBT is defined as computer programs that present the principles and methods of CBT in an interactive manner via a computer interface in two or more sessions. These sessions of CCBT can be presented either on-site (in a treatment facility), online (via the Internet), or via palmtop computers, and the level of therapist involvement can range from none to considerable. Research examining the efficacy of static web pages without interactivity are excluded from this review, as are chat rooms, blogs, eTherapy (or the provision of individualized synchronous or asynchronous therapy on line), preventive programs, and virtual reality tools.
In general, CCBT programs present CBT in a clearly operationalized, highly structured manner often with interactivity based on different multimedia techniques including web pages, cartoons, animations, video, and sound [40, 41]. Homework assignments are often included, as are follow-up and feedback sessions. The topics included in a CCBT program are usually divided into 2–12 sessions, with material from previous sessions often repeated to assist learning and retention. Depending on the disorder CCBT may include sessions on events scheduling, negative thinking, identifying negative automatic thoughts, challenging unhelpful thinking, identifying core beliefs and attributional style, problem solving, sleep management, graded exposure, and progressive relaxation. In addition, most CCBT programs include an introductory session involving psychoeducation, and a final session on relapse prevention.
The frequency of therapist contact in CCBT programs can range from none (completely self-help or self-guided) to maximum (CCBT is used as therapy preparation) [26]. In addition the type of contact can include contact by email phone, or face-to-face consultation.
Does CCBT work?
There are many CCBT programs in use, most of which have been developed for research, although there are a small number of commercially available CCBT programs (Beating the Blues (BtB) [42], Fearfighter [43], and Good Days Ahead: The Multimedia Program for Cognitive Therapy [44, 45]). Reflecting this, the outcome literature is characterized by evaluations of a diverse range of CCBT programs, often with small samples sizes, and differing along several dimensions including the specific content, type of computer interface, types of multimedia, frequency and type of therapist contact, and number of sessions. Rather than attempt a potentially unhelpful meta-analysis, the following summary of the more recent literature will group studies by the specific disorder treated, and will attempt to identify themes and patterns in the results, including effect sizes (ES) when reported. There are recent review with other aims [27, 28, 35].
Depression
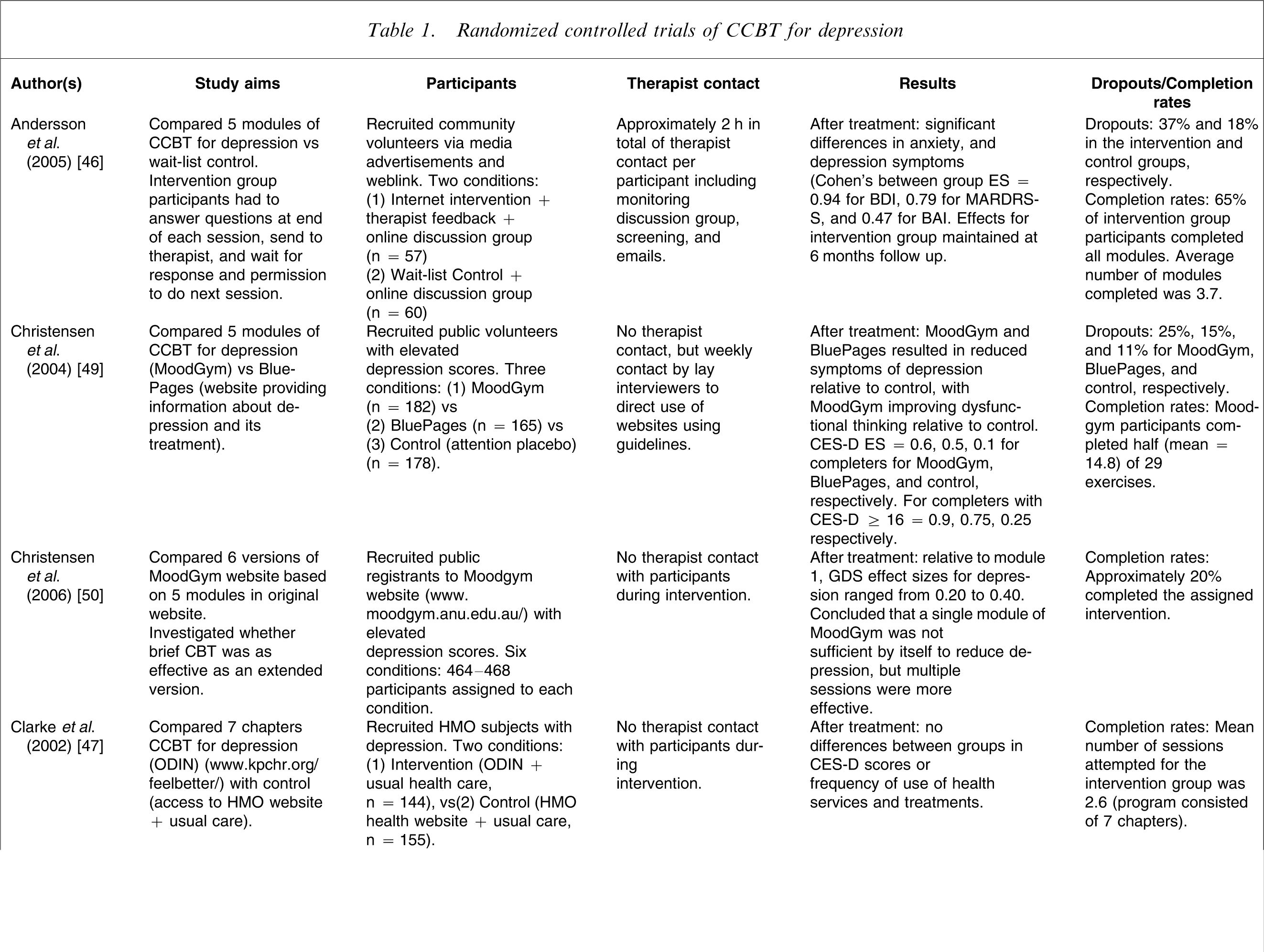
The first CCBT program for depression (Table 1) was developed in the 1980s [30] by Selmi et al. who conducted a three-arm randomized controlled trial (RCT) in which community volunteers with depressive disorder were randomly allocated to either six sessions of a CCBT program for depression (n = 12), or six sessions of therapist-guided CBT (TCBT) (n = 12), or to a wait-list control (n = 12) [41]. The subsequent results were encouraging, with significant differences found between both treatment groups and controls at post-treatment evaluation and reported within-group ESs on the Beck Depression Inventory (BDI) of 0.88 and 0.74 for the CCBT and TCBT groups, respectively, which increased at 2 month follow up. Although the authors reported that no formal therapist contact occurred with the CCBT group, they noted that the CCBT group had approximately 20 min week–1 of contact with the experimenter for assessments.
Randomized controlled trials of CCBT for depression
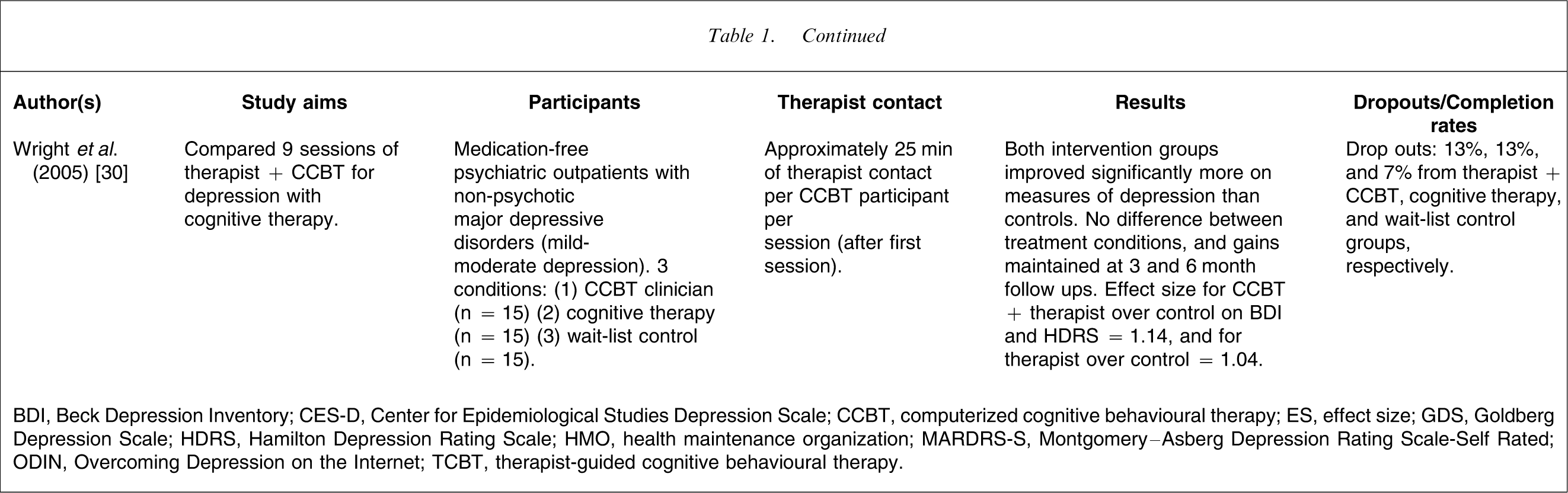
BDI, Beck Depression Inventory; CES-D, Center for Epidemiological Studies Depression Scale; CCBT, computerized cognitive behavioural therapy; ES, effect size; GDS, Goldberg Depression Scale; HDRS, Hamilton Depression Rating Scale; HMO, health maintenance organization; MARDRS-S, Montgomery–Asberg Depression Rating Scale-Self Rated; ODIN, Overcoming Depression on the Internet; TCBT, therapist-guided cognitive behavioural therapy.
In another three-arm RCT again with a small sample Wright et al. randomized participants with mild to moderate depression to either CCBT plus approximately 25 min of therapist time per session, or to cognitive therapy, or to a wait list control group (n = 15, each group) [30]. After 8 weeks of treatment participants receiving therapy had significantly lower symptoms of depression scores (BDI and Hamilton Depression Scale; HDS) than controls, with within-group effect sizes of 1.14 for CCBT, and 1.04 for cognitive therapy.
Using larger samples in an RCT design with two conditions Andersson et al. contrasted the efficacy of CCBT for depression (n = 57) with a control group (n = 60) [46]. In the treatment condition depressed patients completed five sessions of Internet-based treatment for depression with minimal therapist involvement (a total of approximately 2 h per patient including time spent communicating via email) plus involvement in an online discussion group. In contrast, the controls participated in a (different) online discussion group only. The treatment group experienced greater reductions of depressive and anxiety symptoms (ES on the BDI was 0.94 between-groups at post-treatment evaluation), with improvements generally maintained at 6 months follow up.
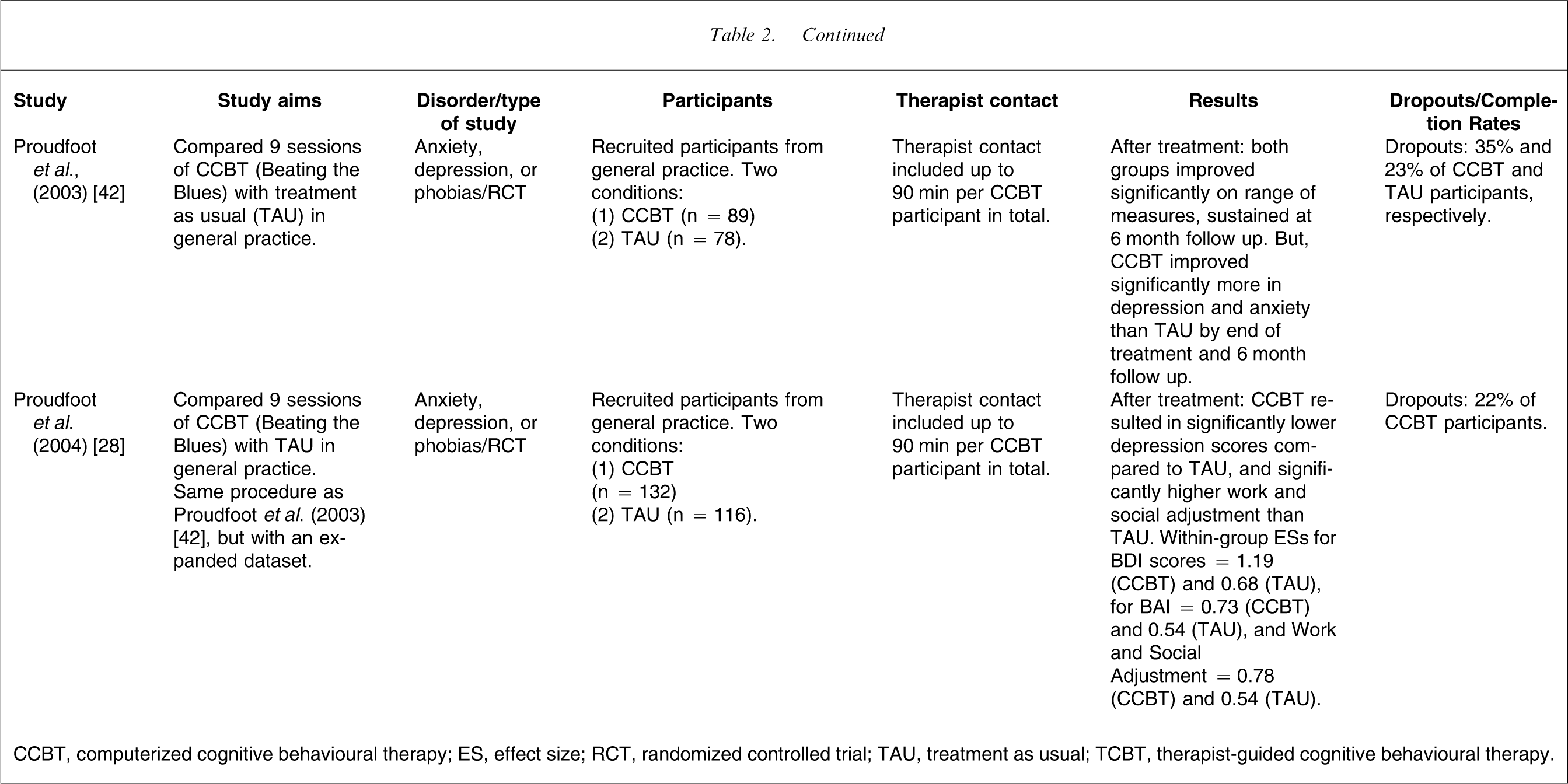
In one study with a commercially available CCBT program for depression [42], BtB was administered to 77 patients in general practice and contrasted with treatment as usual (TAU; n = 66). The BtB program, which involves nine sessions, begins with an introductory video followed by eight therapy sessions with practice nurse contact of no more than 10 min per session. In this RCT, TAU patients were able to receive any treatment, including psychological treatments. The results indicated statistically and clinically significant improvements across measures of anxiety, depression, and work and social adjustment, in favour of the CCBT program although ESs were not reported. These results were subsequently replicated with an expanded sample [28], and the within-group ESs for the BtB group on the BDI, Beck Anxiety Inventory, and Work and Social Adjustment Scale were 1.19, 0.73, and 0.78. The comparable ESs for the TAU group were 0.68, 0.54, and 0.54. The ES superiority of the BtB group over the TAU group was therefore 0.51, 0.19 and 0.24, respectively.
In summary, studies examining the efficacy of CCBT with therapist contact for treating depression have produced encouraging results. Indeed, a preliminary meta-analysis [25] that calculated mean ESs on the BDI across five studies (n of subjects = 151) estimated that CCBT with therapist contact for depression results in a large pre–post-treatment mean ES of 1.38. This is consistent with some studies that have found comparable ESs between CCBT and TCBT [43].
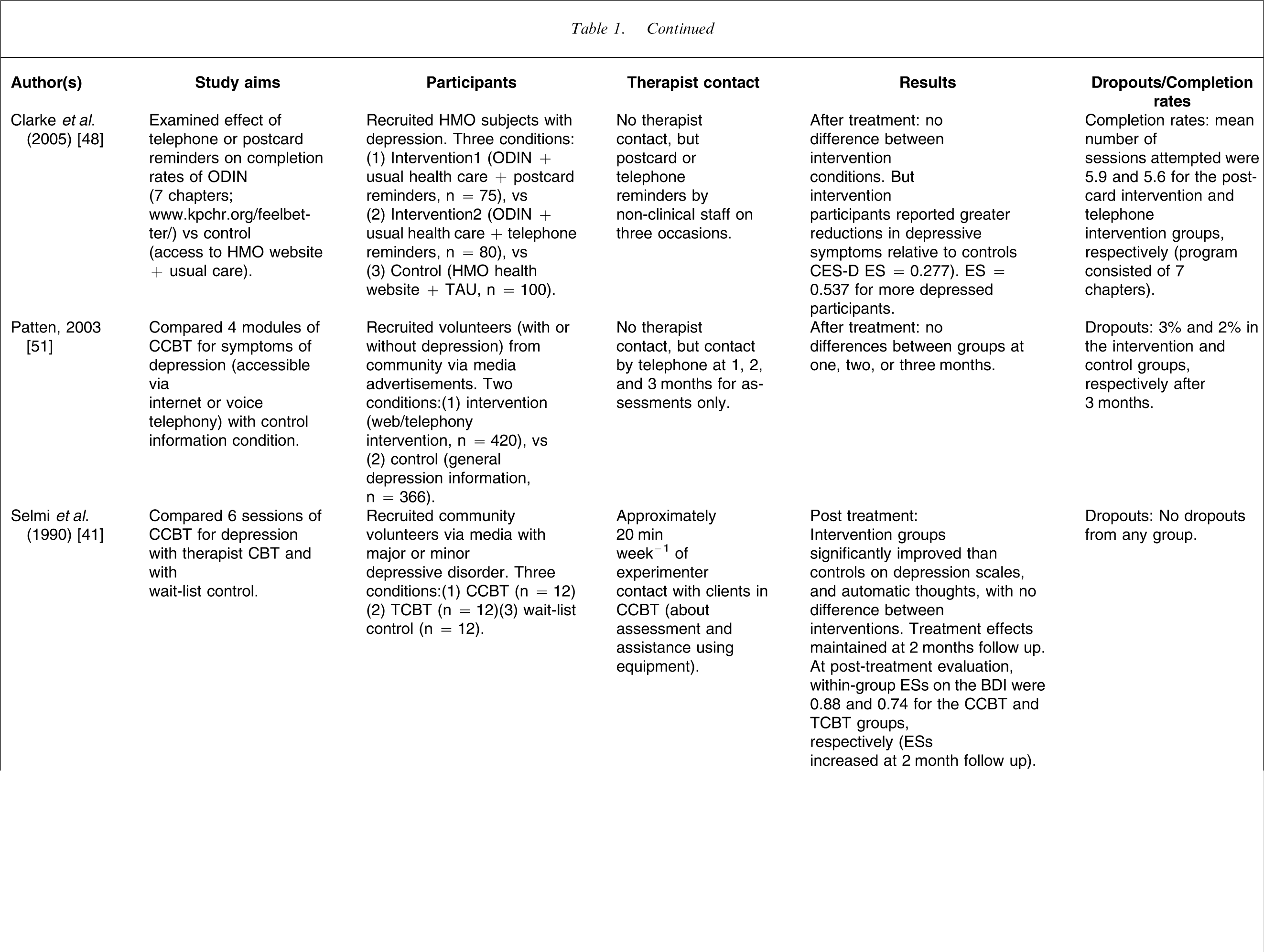
Outcome studies of CCBT without therapist contact for depression have produced a different pattern of results. Studies of CCBT without therapist contact have generally been characterized by larger sample sizes, but low completion rates and more modest effect sizes. For example, in a study of CCBT without therapist contact Clarke et al. randomly allocated participants with depression either to an intervention condition (CCBT plus TAU; n = 144) or to a control condition (involving access to a health website plus TAU; n = 155) [47]. No differences were found after treatment or at follow up between groups or within groups, with reportedly high attrition rates. This methodology was subsequently modified in a three-arm RCT in an attempt to increase completion levels by either sending participants in the intervention groups postcard reminders (n = 75) or telephone reminders (n = 80), with no reminders to controls (n = 100) [48]. After treatment, intervention participants described a greater reduction in depressive symptoms (ES = 0.28; ES = 0.54 for more depressed participants), indicating that reminders did assist completion rates, although the reported completion rates were still low, with median use of the website of 2 sessions, when seven sessions were available.
Christensen et al. explored the efficacy of an Australian CCBT (without therapist contact) website for depression (MoodGym) in a three-arm RCT by randomly allocating participants either to five modules of the MoodGym program (n = 182), or to a website providing information about depression and its treatment (BluePages; n = 165), or to a control condition using an attention placebo (n = 178) [49]. They reported that participants allocated to Moodgym and BluePages reported significantly reduced symptoms of depression relative to controls with ESs for the Center for Epidemiological Studies Depression Scale (CES-D) of 0.4, 0.4, and 0.1 for the MoodGym, BluePages, and the control interventions, respectively, with higher reported ESs for completers (MoodGym participants completed half the assigned exercises on average).
In a subsequent study the same research group explored how to increase website use and retention of MoodGym participants [50]. In that RCT, participants were randomly allocated to one of six different versions of MoodGym that differed in number of sessions and content (n = 464–468 participants in each condition). The results indicated that single sessions were insufficient to reduce depression, but that modules comprising extended CBT components were associated with greater improvements (within-group ESs for the Goldberg Depression Scale ranged from 0.20 to 0.40).
In another RCT of CCBT without therapist contact Patten randomly allocated community volunteer participants either to four sessions of CCBT for depression over the Internet (n = 420), or to a control condition involving access to website information about depression (n = 366) [51]. No differences were observed on the CES-D between groups at 1, 2, or 3 months, but the author reported that the mean interaction time with the program was only 50 min in total, suggesting low exposure to the therapy materials.
In brief, CCBT for depression with therapist contact is associated with ESs comparable to those observed in face-to-face therapy. The ESs of CCBT without therapist contact are considerably more modest and reflect the low completion rates that are probably due to the absence of a therapist who would help motivate a client, reinforce their progress, and encourage further efforts. However, there is evidence that CCBT without therapist contact can result in improvements in some participants [48] and, given the cost-effective nature of such interventions, they may be an appropriate resource, particularly with motivated participants.
Anxiety
Most studies of CCBT for anxiety (Table 2) have included therapist contact and have targeted specific anxiety disorders.
Randomized and uncontrolled trials of CCBT for anxiety disorders
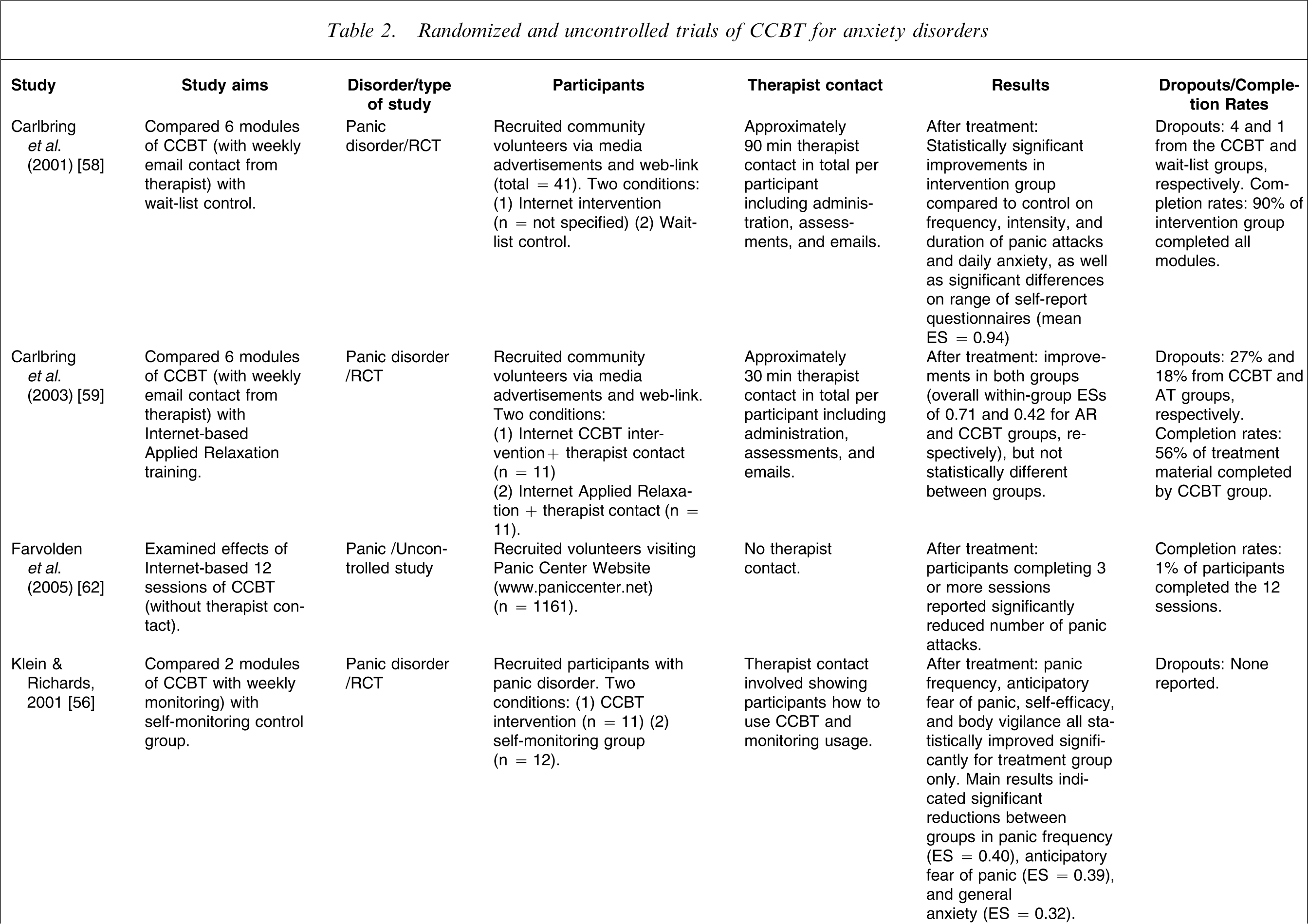
CCBT, computerized cognitive behavioural therapy; ES, effect size; RCT, randomized controlled trial; TAU, treatment as usual; TCBT, therapist-guided cognitive behavioural therapy.
Panic
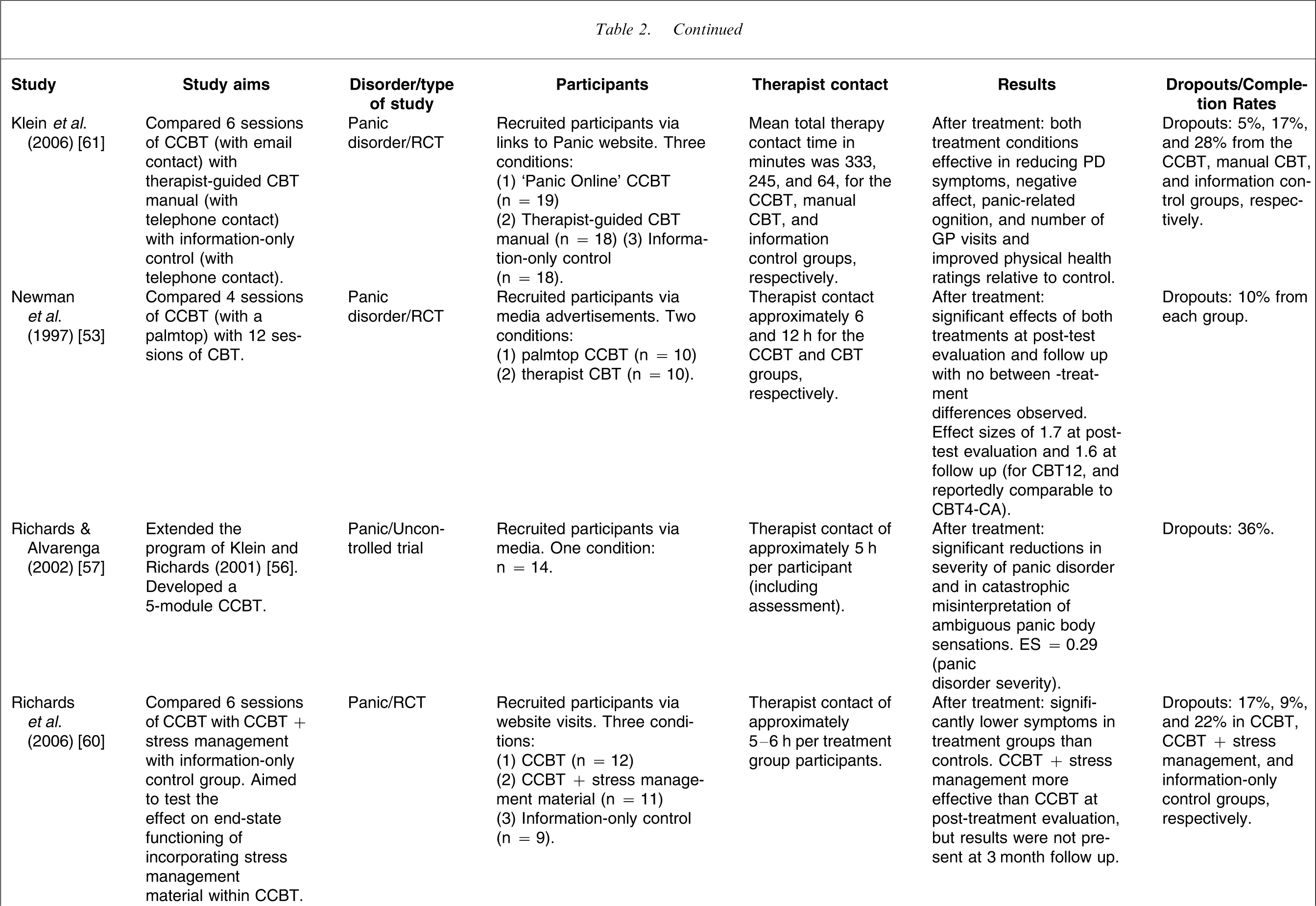
Studies examining the efficacy of CCBT for treating panic disorder have generally yielded encouraging results [52], but have tended to involve small sample sizes. For example, in an earlier study participants with panic disorder with or without agoraphobia were randomly allocated to CCBT using a portable palmtop computer plus 4 h of therapist contact (n = 10), or to 12 h of TCBT (n = 10) [53]. Significant differences were found at post-test evaluation for both groups, with no differences between treatment groups, and combined ESs of 1.7 at post-treatment evaluation and 1.6 at follow up. Palmtops have been used to treat several anxiety disorders including social phobia, generalized anxiety disorder, panic disorder, and obsessive–compulsive disorder [54], although concern has been raised that they may potentially act as a safety device reducing patient anxiety and fears [55], indicating that their use should be carefully monitored.
Using a brief CCBT program of only two sessions Klein and Richards used an RCT design to assign participants with panic disorder to an intervention group (n = 11), or to a self-monitoring group (n = 12) [56]. That study demonstrated that even a brief CCBT intervention with regular monitoring of usage could result in statistically significant differences between groups, with between-group ESs ranging from 0.32 to 0.40 across several measures including panic frequency and anticipatory fear. In an uncontrolled study that extended the CCBT program described in [56] to five sessions, Richards and Alvarenga found smaller within-group ESs of 0.29 for panic disorder severity, even though participants received an average of 5 h of therapist contact [57].
In an RCT with a larger sample (total n = 41) Carlbring et al. used the Internet to deliver CCBT to participants with panic disorder over six sessions lasting up to 12 weeks with regular therapist contact by email (approx. 90 min in total per participant) [58]. After treatment, statistically significant improvements were observed in the CCBT group compared to the control group across a wide range of measures, with an overall ES of 0.94. In a subsequent RCT Carlbring et al. partially replicated their earlier procedure [58] to explore the effect of reducing the frequency and total amount of therapist contact [59]. They randomly allocated participants with panic disorder to Internet CCBT (n = 11), or to an Internet Applied Relaxation condition (n = 11), but with only 30 min of total therapist time for the CCBT group [59]. Overall ESs within groups were 0.71 for the applied relaxation group, and 0.42 for CCBT, indicating that the 30 min of total therapist time in that study may not have been sufficient, particularly because participants in the applied relaxation group received SMS reminders, and some CCBT participants subsequently reported that they would have preferred deadlines and prompts to help them to complete the program.
Richards et al. conducted a three-arm RCT with patients with panic disorder randomized to an Internet-based CBT program (n = 12), or to an Internet-based CBT program with additional stress management information (n = 11), or to an information-only control group (n = 9), to try to determine whether the addition of stress management information would improve end-state functioning [60]. Although both treatment groups improved significantly more than controls the benefits of the added stress management information were not continued at 3 month follow up, although the small sample size may have obscured effects.
Finally, Klein et al. conducted another three-arm RCT with participants with panic disorder randomized to CCBT (n = 19), or to TCBT using a manual based on the CCBT material (n = 18), or to an information-only control group (n = 18) [61]. After the 6 week program participants in the treatment groups reported significantly fewer panic related symptoms than controls with fewer reported GP visits and better reported physical health. Furthermore, participants in the CCBT group were rated by clinicians as having reduced agoraphobia and had a lower number of GP visits at post-treatment than the TCBT manual condition. That study is particularly relevant because it compared CCBT with a therapist-guided manual based on the material in the CCBT versus a control condition. In addition, those authors conducted a cost-effectiveness analysis, which indicated that the CCBT condition required slightly more therapist time, but required less total days in treatment than the manualized condition.
Non-therapist contact
The effectiveness of non-therapist CCBT for symptoms of panic and agoraphobia has also been examined and, as with depression, CCBT for anxiety without therapist contact has resulted in modest success. For example, in an uncontrolled study 1161 volunteers were recruited from a popular website about panic (www.paniccenter.net), into a 12 week CCBT program [62]. Despite only 1% of participants completing, they reported significant reductions in reported attack frequency and severity in participants who had completed at least three sessions. As with non-therapist sites for depression, these results indicated that non-therapist sites are likely to be associated with large attrition rates, but that even participants who do not complete the entire programs may still gain benefit.
Social phobia
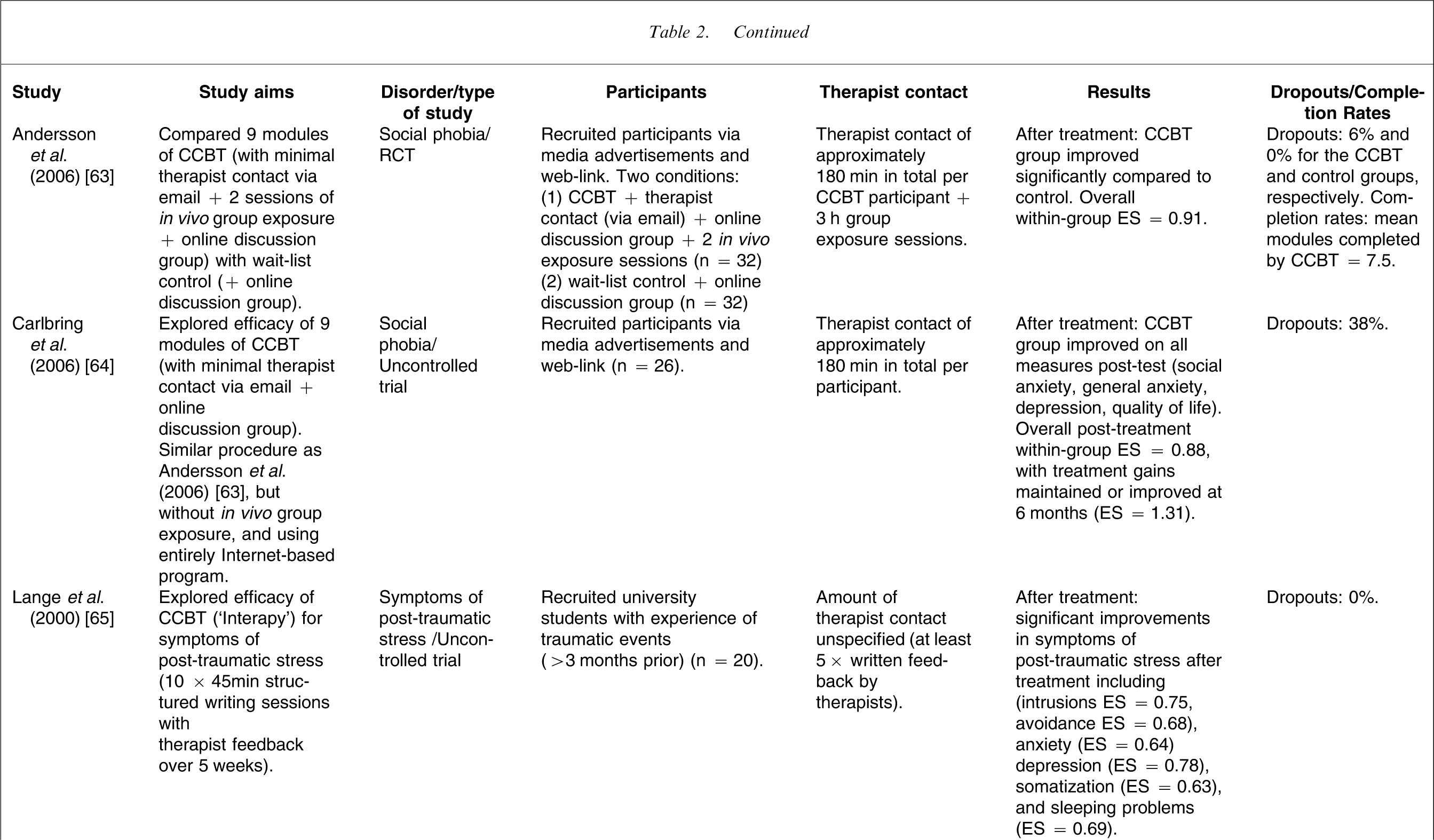
Two studies using similar designs have explored the efficacy of using CCBT for social phobia, and both have produced encouraging findings [63, 64]. Andersson et al. used a two-arm RCT to randomize participants with social phobia either to an intervention condition comprising nine Internet sessions plus minimal therapist contact via email plus two in vivo exposure sessions plus access to an online discussion group (n = 32), or to a wait-list control group who had access to a (different) online discussion group (n = 32) [63]. The mean within-group ES for the intervention condition was 0.87 while the mean between-groups ES across all measures was 0.70, reflecting significant improvements on measures of social anxiety, general anxiety, depression, and quality of life. These results were maintained at 1 year follow up. In a subsequent but uncontrolled study, the same research group examined the effect of omitting the real-life group exposure sessions from the procedure [64]. The 26 participants in the treatment group confirmed the improvements observed in their earlier study with improvements in quality of life, depression, general anxiety, and social anxiety, with an overall within-group ES of d = 0.88 (Cohen's d). Again, treatment gains were improved or maintained 6 months after treatment (d = 1.31).
Post-traumatic stress symptoms
At least two studies with university students [65, 66] and one study with members of the public [36] have examined the efficacy of an Internet-based CCBT program for symptoms of post-traumatic stress (no formal psychiatric diagnoses were reported in these studies). In contrast to most CCBT programs, the treatment technique used in these studies primarily involved writing therapy (‘Interapy’), in which participants provide written submissions about a trauma topic specified by their online therapist, with whom they were in regular contact. These studies each involved 10 sessions of 45 min duration, and with five or seven sets of therapist feedback, provided by email, and although the exact amounts of therapist time were not reported, the nature of the feedback presented by therapists suggested that considerable time was involved. In brief, the results of these studies have been positive.
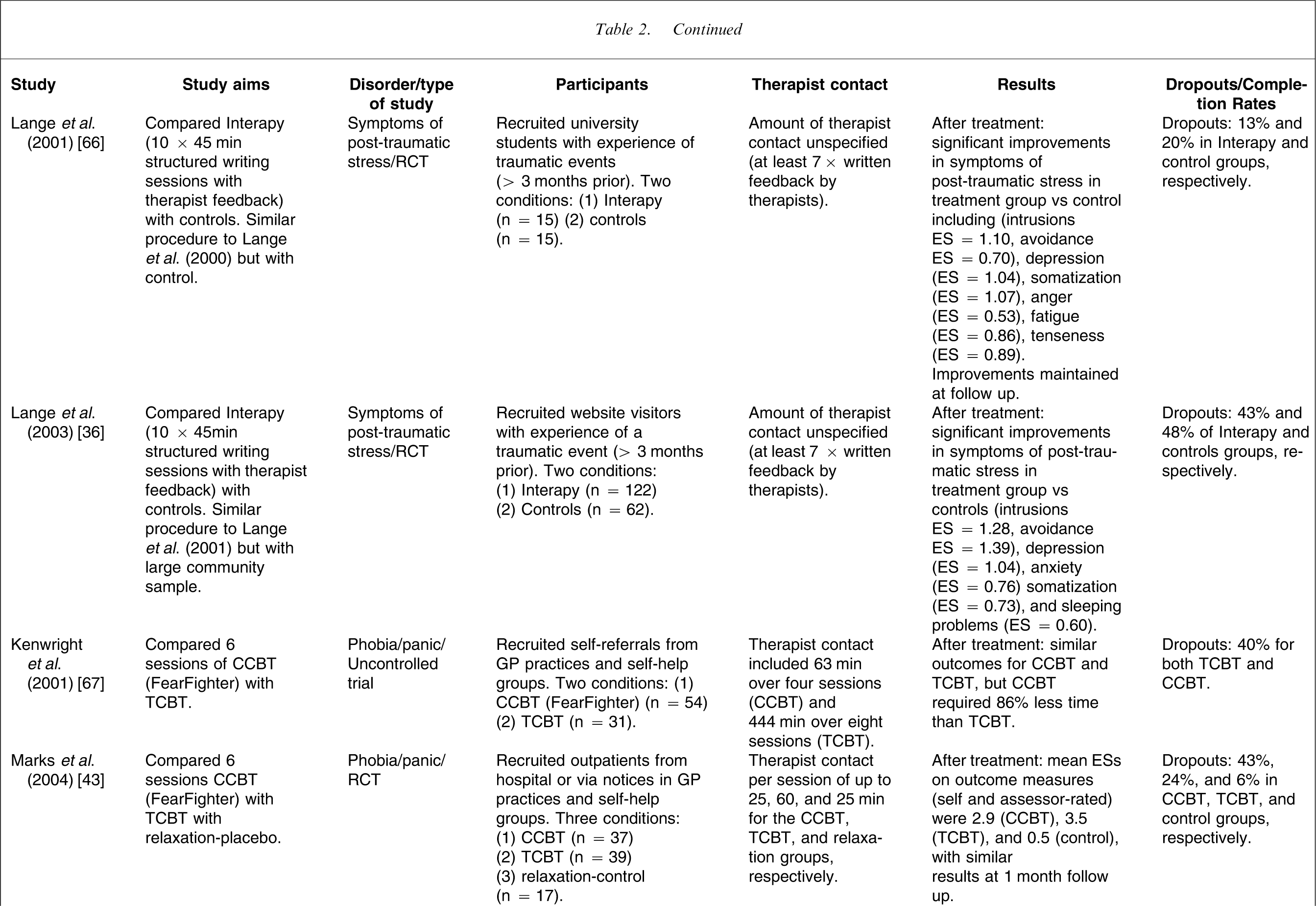
In the first study with university students and using an uncontrolled design (n = 20), post-treatment ESs across a range of measures ranged from 0.63 to 0.75 [65]. In the second study using university students but employing a two-arm RCT design the Interapy group (n = 15) improved significantly more than controls (n = 15) across a range of measures (intrusions, avoidance, depression anger, fatigue, tenseness, and somatization) with ESs ranging from 0.53 to 1.10 [66]. These findings were confirmed in a subsequent two-arm RCT with community volunteers using a larger sample, where the Interapy group (n = 122) again improved significantly more than controls (n = 62) across a range of measures with ESs ranging from 0.60 to 1.28 [36].
General programs for anxiety
In addition to CCBT for specific anxiety disorders, a more general and commercially available CCBT program, FearFighter [43], has been developed to treat patients with panic and/or phobia. FearFighter involves nine steps of exposure, with up to 20 min of therapist face-to-face contact per session. In an uncontrolled study Kenwright et al. contrasted six sessions of Fearfighter (n = 54) with TCBT (n = 31) administered by nurse therapists [67]. Similar clinical outcomes were found between groups, but the CCBT program was reported to require 86% less therapist time than TCBT. These findings were confirmed in a subsequent three-arm RCT, in which patients with phobia and/or panic were randomly allocated either to Fearfighter (n = 37), or to TCBT (n = 39), or to a computer-guided relaxation control group (n = 17) [43]. In that study within-group effect sizes of 2.9, 3.5 and 0.5 were reported at post-treatment evaluation for the CCBT, TCBT, and relaxation groups, respectively, with no significant difference between the two intervention conditions. Again, a significant reduction in therapist time (>70%) was observed with CCBT over TCBT. Of note, large dropout rates were found in the CCBT (43%) and TCBT conditions (24%), but the difference between groups was not statistically significant.
Summary: does CCBT work?
In summary, these preliminary results of studies evaluating the efficacy of CCBT for anxiety disorders and depression are encouraging. The results favour therapist-led CCBT, although it appears that as few as three sessions of non-therapist CCBT can result in reductions in symptoms for some participants.
Methodological problems in CCBT research
There are several methodological problems that should be considered when evaluating this research. For non-therapist-based CCBT studies administered solely over the Internet [47–51, 62] these include issues of sampling bias, with participants usually self-referring, and having higher education levels and lower levels of comorbidity than the general population of patients [58, 63, 64]. This may not challenge the validity of the results, providing that demographic and psychiatric characteristics of completers and non-completers are carefully reported, but it does raise questions about the generalizability of reported findings to other patient populations.
A potentially more difficult methodological issue with such studies is the uncertainty about the actual identity of participants, which cannot easily be confirmed. Consequently, it is likely that some participants may actually be curious, rather than anxious or depressed, and may withdraw from a study or provide invalid responses for reasons unrelated to a study, potentially confounding analyses [68]. In addition, self-selection without a thorough clinical assessment provides the opportunity for inaccurate self-diagnosis by patients, leading to attempts at inappropriate and unhelpful treatment, further confounding results.
Another methodological issue with non-therapist-guided CCBT studies administered over the Internet are their high dropout rates with, for example, one study reporting completion rates of 1% of registered users [62]. In addition, studies rarely clearly describe how much exposure participants have actually had to the materials, raising questions about the extent of program engagement [69] and making it difficult to interpret findings. New strategies for reporting and analysing the results of CCBT studies are required [70]. There is some validity to such calls, particularly since so-called dropouts who may not be included in final analyses, may actually have improved and had withdrawn because their symptoms were sufficiently improved [43], in the way that clients in TCBT may withdraw before the completion of a planned course of sessions because their symptoms have become manageable. Finally, a more pressing issue in much of the CCBT research involving therapists is the relatively small sample sizes, which, combined with sampling bias, highlight the need for larger studies.
Advantages of CCBT
Despite the methodological weaknesses noted here, CCBT presents several potential advantages to clinicians, patients, and service managers. These advantages include the dissemination of standardized yet individualized treatments provided with a high degree of fidelity [55, 71], the inclusion of measurement tools, and the ability to collect and monitor relevant data.
Furthermore, the advantages, specifically for patients, are numerous, including that CCBT can potentially reduce barriers for non-metropolitan or rural residents who have to travel considerable distances to gain access to high-quality mental health resources [54, 72], it can provide consistent feedback [26], and may promote self-monitoring. In addition, CCBT can also potentially reduce some of the barriers associated with the stigma or embarrassment of seeking specialist mental health services [64]. This may be particularly relevant to populations who traditionally avoid seeking treatment or who may not usually consult a health professional [73]. In addition, CCBT can potentially provide a treatment opportunity for people who are unable to attend therapy during usual clinic hours, due to employment, family, or other commitments. These points are pertinent given the low proportion of people actually seeking treatment for mental illness [2, 6]. An additional potential advantage is that CCBT can teach patients the basic constructs in CBT as well as the language of therapy, which may potentiate subsequent CBT.
Perhaps the most touted potential advantage of CCBT is the promise of increasing the capacity of trained CBT therapists due to reduced time required by therapist per patient [11, 43, 74]. This advantage will appeal to patients, who may experience shorter treatment delays; to clinicians, who could provide high-quality treatment to a larger number of patients; and to service managers, who are responsible for increasing the capacity of their mental health services.
Cost-effectiveness and implementation
When considering the implementation of new technology, service managers will consider several issues including its clinical effectiveness, cost-effectiveness relative to current treatments, acceptability to users, and the direct and indirect costs of implementation.
Clinical effectiveness of CCBT
Some studies involving therapist contact have reported effect sizes comparable to those obtained in face-to-face therapy for the treatment of anxiety disorders and depression [28, 30, 36, 41–43, 53, 63–66]. This is an encouraging first step but needs to be explored further with larger sample sizes and, given their specificity, it is likely that CCBT programs should be evaluated individually. A related and unresolved issue concerns the minimum levels of therapist contact time that may be considered clinically effective. This is particularly relevant because some researchers have noted that low therapist contact can result in patients reporting feeling isolated and demotivated [59], while other researchers have cautioned about the risks of failing to identify potentially suicidal patients [26, 52]. This illustrates the point that CCBT is a clinician extender, rather than a clinician replacer [75], and that failing to provide adequate therapist support to patients using CCBT may constitute unacceptable clinical practice.
Cost-effectiveness of CCBT
Several studies have provided estimates of the cost effectiveness of CCBT, with one major review concluding that CCBT reduces therapist time in comparison with therapist-delivered CBT [27]. For example, in the UK, the FearFighter system has been demonstrated to save at least 70% of a clinician's time relative to equivalent face-to-face therapy, with no difference in outcome [34, 43, 67]. More locally, cost savings of CCBT over therapy provided by general practitioners have also been demonstrated in an Australian study [76].
In apparent contrast, however, at least one study found that the BtB program was actually slightly more expensive per person to administer than TAU in the short term in general practice, possibly because general practitioners had to proactively review patients [37]. However, they reported that in the medium to longer term BtB was less expensive, because savings were made on reduced employment costs and by TAU participants using more Accident and Emergency Department (A&E) visits and more post-intervention counselling than the BtB group. These data are particularly instructive because they indicate the risk of cost shifting, and the importance of considering service utilization across a range of areas when evaluating the cost effectiveness of CCBT. Second, these data indicate the need to carefully compare different CCBT programs, because characteristics and features vary considerably between programs.
A related question concerns the cost-effectiveness of CCBT relative to other forms of guided self-help treatments. There is limited evidence that clinician-guided CCBT results in superior outcomes compared to clinician guided self-help manual [61, 77]. However, some [78, 79] but not all [80] studies on minimal therapist contact CBT bibliotherapy for depression have reported large effect sizes, indicating that further comparisons are necessary, particularly because the implementation costs of guided bibliotherapy may be more acceptable than CCBT, although it should also be noted that books are less interactive, more difficult to disseminate on a large scale and harder to modify [75].
Acceptability of CCBT
A critical issue in the implementation of any treatment technique or strategy involves its acceptability to users. Encouragingly, data about participants’ perceptions of CCBT programs have generally appeared positive, and similar to those attributed to therapist-delivered CBT [27, 34, 61, 75]. From another perspective, the dropout rates during CCBT with therapist contact are often comparable to TCBT [81], indicating that it has acceptable clinical validity to patients.
Unfortunately, there appears to be little data exploring CCBT's acceptability to the general public or to clinicians, although several pieces of evidence suggest that CCBT is acceptable in principle: First, a high number of Internet users report using the Internet to explore health sites [82], with approximately 18% specifically searching mental health sites [83]. Second, general hit rates on CCBT open access Internet sites are very high, with for example, the MoodGym site registering 15 000 users over a 19 week period in 2005 [50], while the Panic Center website recorded almost half a million visits from almost 100 000 users over an 18 month period [62]. Third, more than 90% of British CBT therapists recently indicated that they would consider using computer-based self-help programs, although only 2% were actually using it [84]. And finally, the results of a postal survey inquiring about the respondents’ preferences for treatment for anxiety disorders indicated that a high proportion (>90%) reported a desire to access some form of computer-aided self-help [85].
Taken together, these strands of evidence suggest that CCBT is acceptable in principle, but two caveats should be noted. First, the low completion rates of some sites suggests that further studies to support participants to complete more of the material are needed and, second, the low rate of use by clinicians suggests that considerable education of clinicians is required prior to any attempt at implementation.
CCBT and stepped care
Another important issue regarding implementation relates to CCBT's location within a stepped care model. Several authors have proposed a role for CCBT in primary care, in order to promote standardized and high-quality treatment particularly of high-prevalence conditions [11, 31–39], while other authors have also recommended CCBT as a relapse prevention tool in stepped care [25]. Evidence from the UK suggests that CCBT can be successfully implemented in primary general practices [28, 42] and in community mental health clinics [34, 86]. For example, Gega et al. described using several CCBT programs in a community mental health clinic with overall ESs in excess of 0.8 on several measures, with moderate levels of user satisfaction, and with significant reductions in therapist time per patient [34]. Furthermore, two CCBT programs (BtB and FearFighter) were recently recommended by the UK-based National Institute for Clinical Excellence as an option for delivering CBT in the management of mild to moderate panic and phobia within a stepped-care management program [38].
There is some evidence in Australia that therapist-guided CCBT can be effective in general practice [76], but considerable research on implementation remains to be conducted. It is also important to note that the use of electronic mental health resources by Australian general practitioners appears to be very low [87], and at least one Australasian study indicates that many patients may not wish to disclose mental health concerns to their GP [88], while overseas research suggests that general health physicians may not welcome Internet-based health material presented by patients [89]. These points are particularly relevant, and indicate the need for ongoing public and professional education about mental health and treatment [90]. A related point concerns the importance of clinicians and patients recognizing that CCBT raises different ethical and professional issues to usual TCBT, and users should become familiar with existing guidelines that have been developed and endorsed internationally to assure that acceptable protocols of clinical care are provided [91].
Other issues
Numerous practical issues must be considered when determining the potential utility of CCBT. The potential of CCBT to help primary practitioners manage patients within a chronic health-care model raises issues about how best to support such practitioners to modify their clinical systems so that they can proactively support and monitor their patients [92, 93]. Issues concerning the development, maintenance, and modification of CCBT systems also need to be considered, particularly because resources will eventually require updating, and clinicians will prefer CCBT programs that are bundled together, rather than having to individually evaluate and source such programs. This will require a considerable level of coordination and resourcing, raising questions about the appropriate organizations for managing such projects. As an interim step, however, considerable work must still be conducted at local levels to demonstrate the proof of concept that CCBT can be integrated into stepped care, and such research will help identify implementation issues relevant at national and international levels. Additional research questions are included in Table 3.
Research questions
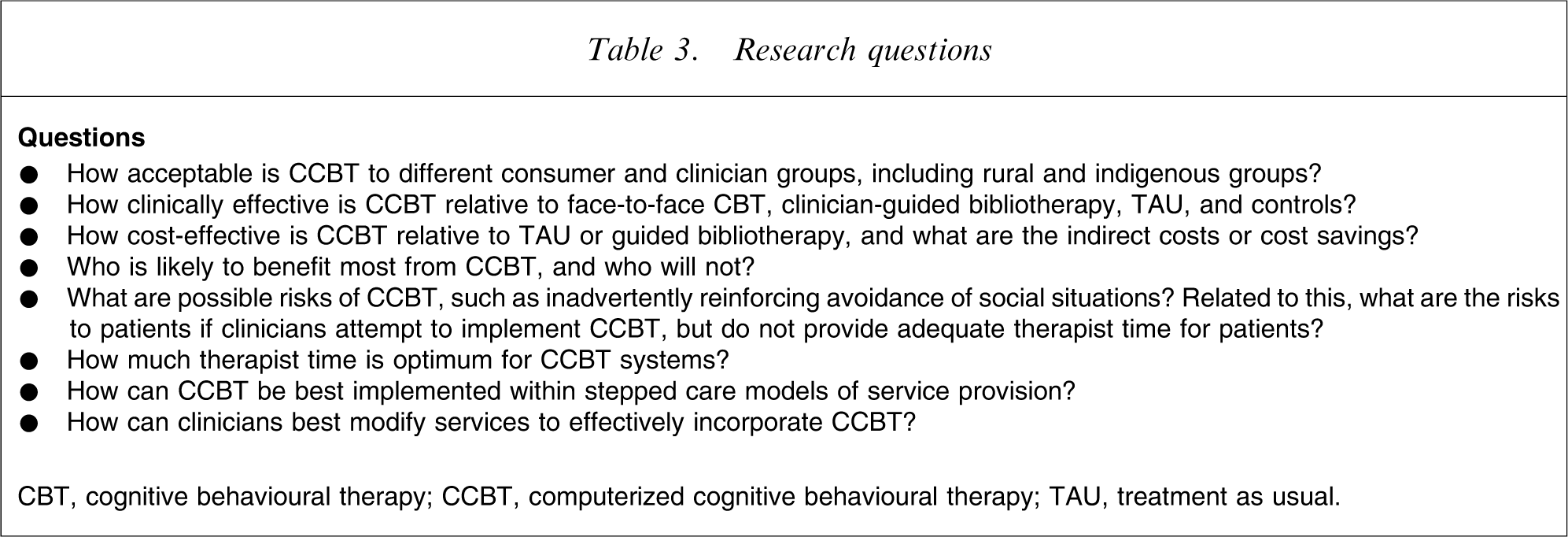
CBT, cognitive behavioural therapy; CCBT, computerized cognitive behavioural therapy; TAU, treatment as usual.
Summary and conclusions
A wide range of CCBT programs has been developed for treating depression and anxiety disorders and these vary on several characteristics including the extent of therapist contact, the number and content of sessions, and the multimedia used. The literature is generally characterized by relatively small sample sizes and in many cases, self-selection biases exist. However, the preliminary evidence is encouraging, with multiple RCTs demonstrating that CCBT programs involving therapist contact can significantly reduce symptoms of depression, anxiety, social phobia, panic disorder, and symptoms of post-traumatic stress, sometimes with effect sizes comparable to therapist-led CBT. Studies have also shown that CCBT without therapist contact may also be useful for some people, particularly if they are sufficiently motivated.
UK-based studies examining the implementation of CCBT in general practice and into community mental health services have provided encouraging reports that CCBT can be cost-effective, and that wider savings may result from reductions in service utilization at secondary or tertiary levels. This raises the issue of how CCBT might be best implemented into stepped care models of mental health service provision in Australasia. As is obvious from the present review, there is a need for considerably more research into the potential utility of CCBT into the Australasian environment, and given that Australia and New Zealand are internationally ranked within the top five countries for saturation of Internet use [94], it seems logical that we proactively explore the opportunities such technology can provide.
However, as noted by several authors it is important to stress that CCBT is not a clinician replacer, but rather, may best be considered a clinician extender [73, 95]. Until further evaluations of CCBT are reported, clinicians are encouraged to explore websites providing information about CCBT [96]. Relevant websites with published data supporting efficacy, or sites that are currently being formally evaluated, are included as Table 4.
CCBT websites
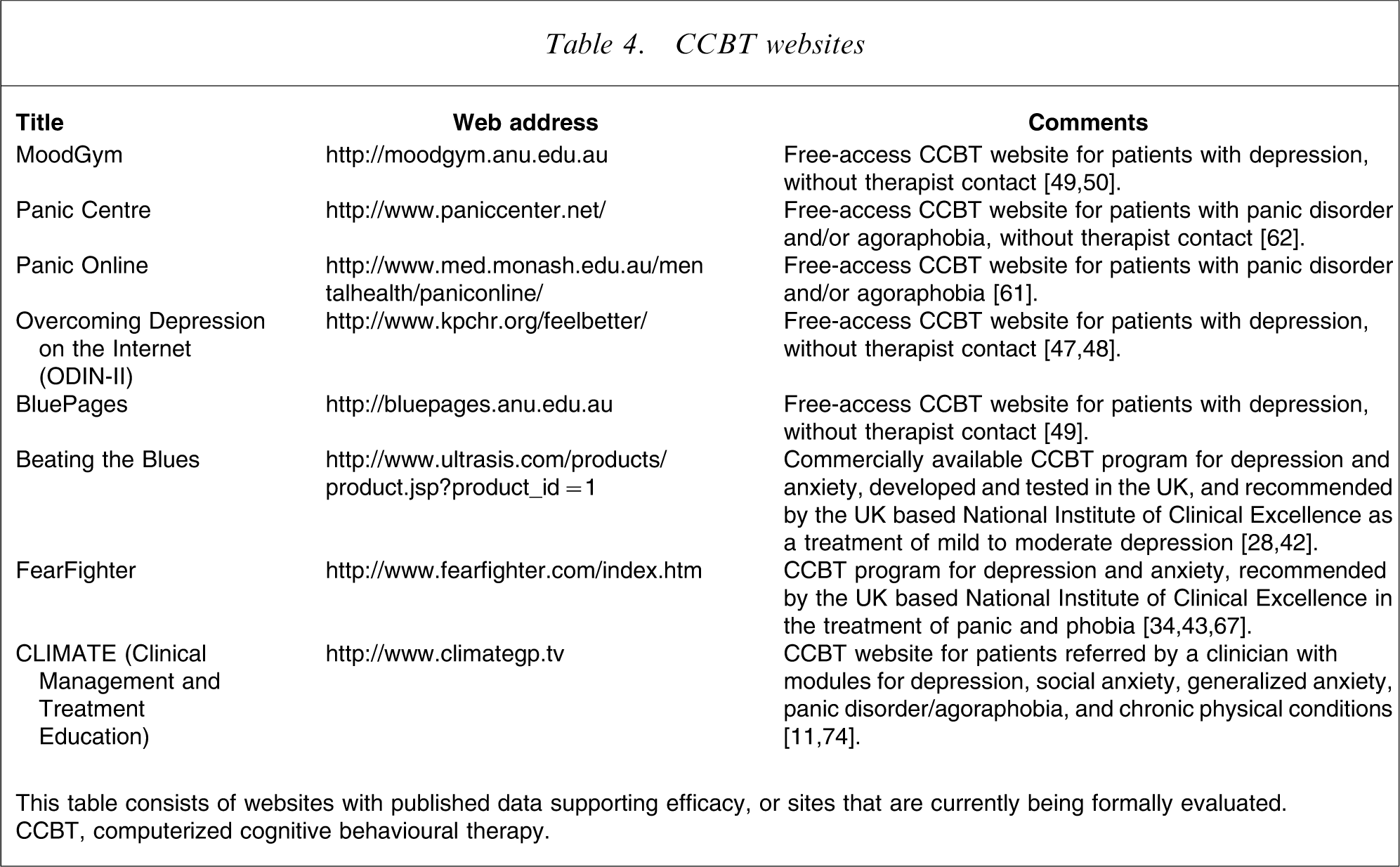
This table consists of websites with published data supporting efficacy, or sites that are currently being formally evaluated. CCBT, computerized cognitive behavioural therapy.
Considerable work still needs to be done to develop CCBT techniques that are culturally appropriate to Australasia, acceptable to patients and clinicians, easy to use, clinically effective, and cost-effective. While clinicians are currently justified in questioning the place of CCBT in current models of mental health services, there is an increasing body of evidence supporting the clinical effectiveness and potential cost-effectiveness of CCBT. Specific research can help determine whether CCBT will meet its potential of increasing the capacity of our mental health services and by doing so reduce the burden of high-prevalence mental disorders.