
Abstract
Objective:
E-mental health technologies are increasing rapidly, both in number and in utilisation by consumers, health systems and researchers. This review aimed to: (i) examine the features and scientific evidence for e-mental health programs; (ii) describe the growth in these programs in the past decade, and track the extent and quality of scientific research over time; and (iii) examine Australian and international contribution to the field.
Method:
Two types of e-mental health programs; ‘web interventions’ and mobile applications’; targeting depression, bipolar disorder, generalised anxiety disorder, social anxiety, panic disorder and general stress were included. Data were collected from the Beacon website (www.beacon.anu.edu.au; last updated July 2011). Features of each program and their supporting scientific evidence were coded.
Results:
In total, 62 web interventions and 11 mobile applications were identified. Half of these were developed in Australia. The majority of programs were aimed towards adults and were based upon cognitive behavioural therapy. Approximately equal numbers of programs were developed for all targeted disorders except bipolar disorder, which was underrepresented. Only 35.5% of programs, all of which were web-based, had been evaluated by at least one RCT. The number of publications over the last decade is increasing. The majority were from Australian sources. Non-Australian research was lower in diversity and quantity.
Conclusions:
E-mental health research is increasing globally. Australia continues to be an international leader in this field. Depression, anxiety and panic disorder remain the disorders most targeted. Whilst the scientific evidence supporting e-mental health programs is growing, a substantial lack of high-quality empirical support was evident across the field, particularly for mobile applications and bipolar and social anxiety.
Keywords
Introduction
Australia, along with Sweden and The Netherlands, has been a leader in e-health over the last decade (Burns et al., 2010; Slade et al., 2009; Webb et al., 2008). The field itself has burgeoned since the late 20th century, with research on web interventions, robotic solutions, virtual reality and mobile phones emerging from many countries worldwide, seemingly at an accelerated pace. Over the last 5 years, e-health solutions have been legitimised via implementation into national health systems. For example, Norway and Sweden now offer Internet-based mental health services (Andersen and Svensson, 2011). Australia has just established a web portal that offers a range of federally funded online interventions and connects users to a range of web-based mental health services (see www.mindhealthconnect.org.au/). The number of mobile applications that allow consumers to manage and track their physical and mental health is ever increasing (Fox, 2010).
In light of this increasing growth and consumer utilisation of e-mental health technologies (Smith, 2012), this report aimed to take stock of the present state of e-mental health research, with particular reference to Australia. Whilst a wide range of e-health solutions exist, we examine here two types of e-mental health program: ‘web interventions’ and ‘mobile applications’.
The review had three specific aims:
To examine the type, content and level of evidence for identified programs in general and as a function of different psychological/psychiatric diagnoses; namely, generalised anxiety disorder, social anxiety, depression, bipolar disorder, panic disorder and general stress. We collected data only on programs targeting these mental health conditions as they correspond to the main psychiatric diagnoses reflected in the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases (ICD)-10, and cover a representative cross-section of affective and anxiety disorders. Substance use disorders were not considered.
To describe the growth in e-mental health programs over the last decade, and to determine whether the extent and quality of scientific research has increased over time.
To examine Australia’s contribution to the field relative to the rest of the world.
Method
Sample
Data on publications and web interventions were collected from the Beacon portal (www.beacon.anu.edu.au; last updated July 2011) (Christensen et al., 2011), an open-access website maintained by Australian National University. It lists all currently available web and mobile interventions and services used in the prevention or treatment of health disorders, along with descriptive information about their features and an evaluation of the scientific evidence on which they are based. All web interventions are listed on Beacon, even if evidence has not yet emerged of their effectiveness. Psychoeducational programs are also listed but, owing to the large number of sites providing psychoeducation online, to be included they must have been subject to at least one trial evaluation.
Data collection
The features of each program were coded by one of us (KP) in August 2012. The supporting scientific evidence for each program was coded in three ways: the number of research trials; the number of those research trials that were randomised controlled trials (RCTs) (categorised into five levels: 0 RCTs or contradictory evidence, 1–2, 2+, 2+ and supporting evidence, and 3+); and the number of annual publications.
Outcomes
Data are descriptive, with numbers and proportions reported.
Results
Programs
Number and features of programs
In total, 73 e-mental health programs were identified: 62 were websites and 11 were mobile applications. Of these, 15 were developed for depression, 16 each for generalised anxiety disorder (GAD) and panic disorder, and 17 for stress. Only five and four programs targeted bipolar and social anxiety disorder, respectively. Of the 73 programs listed, over half were developed within the Asia-Pacific region (38/73; 52.1%), with 36 of Australian origin. US/Canada and Europe shared a similar proportion of programs (14/73 and 17/73, respectively). The Middle East (3) and international consortia (1) were underrepresented as program developers. Australia clearly dominates the development of web interventions, having developed over half of all existing programs (36/62; 58.1%). Within the smaller domain of mobile applications, US/Canada and Europe are on par as leaders, having developed four applications each to date, whilst Australia follows with two.
Type of intervention, access and target populations
Over half of all programs (40/73; 54.8%) used cognitive behaviour therapy (CBT) as their primary therapeutic modality, mainly by programs targeting GAD (13/40), panic (12/40) and depression (7/40), indicating that it forms the basis of much of the e-mental health field. Psychoeducational approaches (i.e. interventions that provide information, educational materials or feedback/advice in order to educate individuals about the nature and treatment of psychological disorders; Donker et al., 2009) were the next popular, employed by 15/73 programs, most of which targeted depression (6/15) and stress (5/15). Just over half of all web interventions were open-access and free (38/73; 52.1%), 35.6% (26/73) were fee-based, 8.2% (6/73) were accessed through an email administrator and 4.1% (3/73) were closed to research participants only. The majority (61/73; 83.5%) of e-mental health programs were aimed towards adults, 8/73 (11%) targeted child and adolescent age groups and the remaining 4/73 (5.5%) targeted all ages or families.
Scientific evidence
Number of research trials
Of the 73 programs, 38 (52.1%) had not been evaluated by any research trial as of July 2011 (28 web interventions and 10 mobile applications). Only 22 programs (30.1%), all of which were web interventions, had been evaluated by at least one RCT.
Number of RCTs and quality of scientific evidence
Table 1 depicts the evidence-base underlying the available mental health programs. Almost half (28/62; 45.2%) of all web interventions have not yet been evaluated by a research trial. Only 22 of the 62 (35.5%) web interventions have been supported by at least one RCT. Out of a total of 11, only one mobile application has been evaluated through scientific investigation, indicating a substantial lack of high-quality scientific support for existing mobile applications.
Level of evidence for web interventions and mobile applications across disorders.
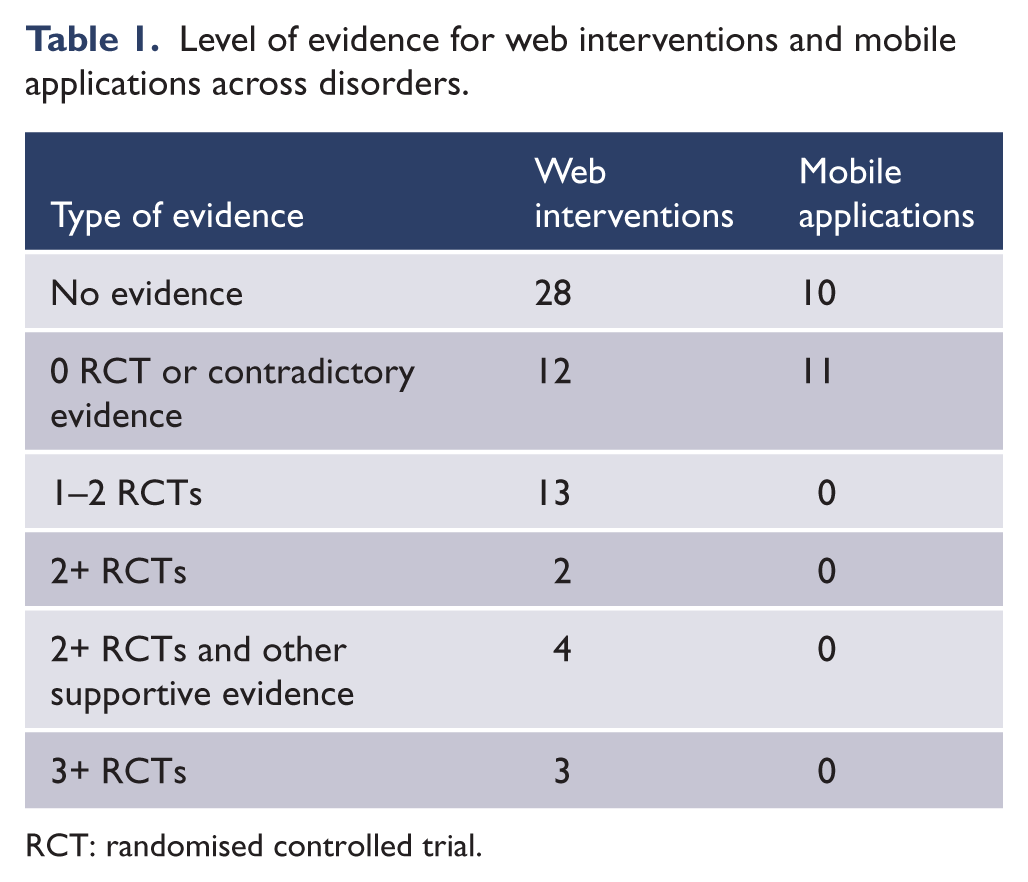
RCT: randomised controlled trial.
Disorder-specific research
Research into depression, GAD and panic disorder dominates the e-mental health evidence-base. Despite this, a general trend is evident within the field where at least half of existing programs are unsupported by scientific evidence. Of the 15 depression programs, 8/15 (53.3%) were not supported by any evidence and only 5/15 (33.3%) programs had been investigated with at least one RCT. A comparable pattern emerged for GAD, with around half of GAD programs unevaluated (9/16; 56.3%) and a quarter (4/16; 25%) evaluated by at least one RCT; similarly for social anxiety. A slightly higher proportion of panic disorder programs (8/16; 50%) had been evaluated by at least one RCT but, even still, half of these were unsupported by scientific evidence. Whilst an equivalent number of stress-based programs (17) exist relative to other disorders, a significantly greater proportion of these programs (14/17; 82.4%) had not been subjected to the same degree of rigorous scientific investigation as GAD and depression programs. Evaluation of bipolar programs was particularly lacking, with no RCTs undertaken to date.
Publications
Across all disorders to date, 95 papers have been published on e-mental health programs since 2002 (Figure 1). Of these, 65/95 (68.4%) were Australian and 30 from international (non-Australian) sources. Following an initial spike in the first half of the decade, the number of publications doubled between 2007 and 2009. The 2010 publications were lower than previous years; however, the trend continued to rise in 2011. As actual publications in 2011 reflect only half the anticipated number (Beacon last updated July 2011), we have anticipated that the number of publications in 2011 will double to 26.
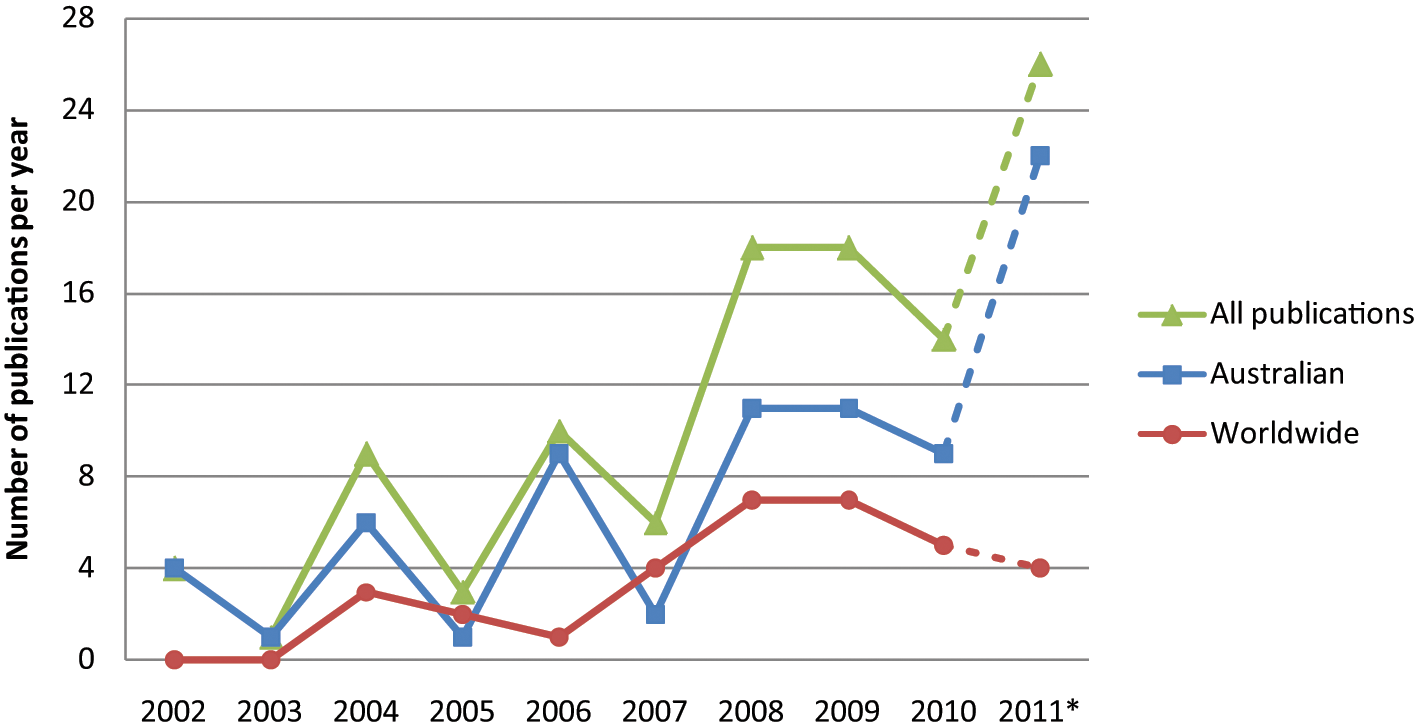
Australian, worldwide and total e-mental health publications between 2002 and 2012. (*All 2011 figures represent projected e-mental health publications up until December 2011; site last updated July 2011.)
The majority of papers focused on e-mental health programs targeting depression (29/95; 30.5%), followed by publications on panic disorder (23/95; 24.2%), GAD (16/95; 16.8%), social anxiety (13/95; 13.7%) and stress programs (10/95; 10.5%). Only four papers on bipolar programs have been published to date (4/95; 4.2%).
Figure 1 shows Australia’s contribution relative to the rest of the world. Australia appears to have begun research in e-mental health earlier and produced a larger quantity of research over time. Further, Australia has sustained publication output in the field of e-mental health over the past decade across all disorders, particularly in depression and panic disorder, and recently in social anxiety and GAD. In contrast, worldwide publications are lower in both diversity and quantity (data not shown). Non-Australian research has focused mainly on depression and stress to the detriment of anxiety disorders and bipolar disorder.
Conclusions
The findings of this descriptive study confirm that e-mental health research is increasing globally and that Australia was and continues to be at the forefront of these developments, most notably as an international leader in the development of web interventions. The US and Canada are now leading the way in mobile phone technologies, although Australia is ranked second. Depression, anxiety and panic disorder remain the disorders most targeted. The scientific evidence is mounting for the effectiveness of the interventions.
Limitations
A number of limitations of this report need acknowledgement. The data presented in this report were based upon sites identified by the Beacon site using their search criteria. However, the site undertakes extensive conventional and web-based searches of literature and the Internet. The Beacon site was last updated in July 2011 (T Reardon, 2012; personal communication), so a lag in publications is present in the data. We did compensate for this where indicated by estimating publication rates on the basis of proportion of the year that had elapsed. Data coding was undertaken by one researcher and was not subject to independent verification. Additionally, coding was of the pre-existing categories determined by Beacon, and as such data in this report represents descriptors assigned by the site.
Challenges for the field
The current report has highlighted substantial gaps in the evidence-base underlying existing e-mental health programs, particularly in mobile applications. The report highlighted a substantial underrepresentation of bipolar and social anxiety programs and research. For Australia, the challenge will be to maintain our lead globally. This may involve investigating new technologies such as tablets, which possess unique advantages for mental health programs in that they combine the advantages of mobile and web platforms. Tablet use is also growing (Purcell, 2011). A second area may be to use our expertise in prevention in areas such as suicide, and investigate how technologies are capable of leveraging content to be delivered at a population level. A third plank in maintaining our leadership is the interest Australia now has in integrating e-health technologies into current health practice, bolstered by new initiatives in the youth space, including headspace and the Young and Well Cooperative Research Centre. It will be important to ensure that we do not allow current practices, bureaucracy, professional ownership and/or organisational culture to stymie the opportunities we have created in this field. Consolidating and expanding the evidence-base around best practice is essential for the field to progress and deliver effective treatment and prevention options via new technologies. Capacity development of young researchers in this environment is critical.
Footnotes
Funding
The Beacon website is maintained by the Centre for Mental Health Research at the ANU. Beacon was developed by Helen Christensen, along with input from the Dissemination Working Party of the International Society Research in Internet Interventions, and ANU e-hub staff. Site development was undertaken by Agile Digital Engineering in association with e-hub staff, ANU. It was funded by a SEO awarded with a NHMRC Principal Research Fellowship 366781 to Helen Christensen and its continued delivery is funded by the Australian Commonwealth Department of Health and Ageing.
Declaration of interest
Along with other ANU researchers, including Professor Kathy Griffiths, Helen Christensen developed MoodGYM and E couch and was involved in the development of BluePages. These sites feature on Beacon. The Black Dog Institute has recently developed Mycompass and BiteBack, which are mental health early intervention and treatment mobile and websites, also listed on the Beacon website.