
Abstract
The purpose of the present paper was to review the current state of evidence for types of case management, focusing on the last 10 years since publication of the Cochrane Systematic Reviews of case management and assertive community treatment. A literature review of electronic databases from 1995 to the present to identify recent research on psychiatric case management, both original studies and reviews, was carried out. Original articles were organized on basis of year of study, experimental group and outcome variables to determine patterns. Sixty relevant papers were located. Thirty-nine are reports of experimental trials of types of case management and 21 are reviews or discussion papers. The focus of research is on assertive community treatment or intensive case management, with only five papers on other forms of less intense case management. Numerous outcomes have been examined, of those examined often enough to draw meaningful conclusions only one, engagement with services, has been consistently positive. All other outcomes have produced mixed results. The strength of findings in favour of case management has weakened over time. A heterogeneous group of experimental designs limits comparisons. Numerous issues with methodology and definitions of types of case management have beset research in this field. Assertive types of case management (including assertive community treatment and intensive case management) are more effective than standard case management in reducing total number of days spent in hospital, improving engagement, compliance, independent living and patient satisfaction. More important than the type of service configuration is to understand the clinical criteria of the services provided and their effectiveness.
Case management is a ubiquitous practice central to 21st century public mental health services in many Western countries. Despite its widespread implementation there remains controversy regarding the benefits of various types of case management. In historical terms case management has had a rapid rise to prominence since deinstitutionalization shifted the emphasis from hospital-based to community care. The driving forces behind this massive systemic change were largely political and financial. Although a number of individual components of community treatment have been found to be both acceptable to patients and families and associated with some improvement in quality of life, the evidence for case management as the best structure to deliver these services is debated.
The Team for the Assessment of Psychiatric Services (TAPS), found that moving out of the mental hospital into well-resourced non-hospital settings improved the life circumstances and social functioning of the residual long-stay patients. The resettlement process had little impact on psychiatric symptomatology [1].
In the Australian context a study of patients transferred to community care units (CCU) had similar findings [2]. Other studies have found that supported accommodation in the community has encouraging outcomes for residents, at least in the short term, both in Australia and overseas [1, 3, 4]. The vast majority of patients in contact with public mental health services receive some form of case management, accounting for a large proportion of community resources, both financial and personnel. Case managements’ primacy has arisen despite an unclear and controversial evidence base.
In the 1990s two Cochrane systematic reviews focusing on case management for severe mental disorders were published. The first in 1996 reviewed case management [5] and the second in 1998 reviewed assertive community treatment (ACT) [6].
The first Cochrane review found little evidence for benefits of case management. Although case management increased the numbers of patients who remained in contact with services, it approximately doubled the numbers admitted to psychiatric hospitals. The authors’ conclusions regarding case management were clear, stating that case management did not produce clinically significant improvement in mental state, social functioning, or quality of life, nor did it improve outcomes on any other clinical or social variables, while increasing health-care costs.
The concluding remarks were ‘case management is an intervention of questionable value, to the extent that it is doubtful whether it should be offered by community psychiatric services’ [5]. These findings and provocative conclusions drew great debate and vehement rebuttal from the psychiatric community around the world. The review was criticized for its choice of principal outcomes [7]. First, contact with services may be interpreted positively or negatively and may not relate to the usefulness or influence of that contact. Second, Parker argues that the use of decreased hospital admissions as a primary outcome measure is generally underpinned by political and philosophical motives rather than clinical criteria and does not necessarily reflect a failing of the system [7]. A more clinically relevant outcome might be duration of hospital admission, which has since been studied. Third, the expectation of finding a significant result in ‘improved clinical outcome’ in those with severe mental illness and significant disability is questioned as being realistic.
The control and experimental groups have been criticized as being ill-defined, and the experimental groups critiqued for being staffed with poorly trained personnel and limited to a very narrow model, ‘a passive sedentary office hour's brokerage model being implemented in the UK’ [7–9]. Further critique of this first Cochrane review has included the limitations of very strict inclusion criteria that resulted in only nine trials being assessed in the original paper [8]. The results of a large meta-analysis published in 2000 [10] contradict the Cochrane findings on case management. Forty-four studies were included on ACT and case management and both were found to decrease total hospital days.
The follow-up Cochrane Review on ACT was published in February 1998 and, in contrast to the earlier review, had unambiguously positive results [6], with ACT comparing favourably to standard community care, hospital-based rehabilitation and case management. ACT increased those in contact with services and decreased number of hospital admissions and length of time in hospital. Significant and robust differences between ACT and standard community care were found on accommodation status, employment and patient satisfaction. ACT consistently reduced the cost of hospital care, compared to both standard community care and case management.
Despite such positive findings for ACT there is growing acknowledgement that the mental health system in Australia is failing to adequately support some of the most disadvantaged members of our community [11]. This literature review and a partner review (currently underway) on the components of community care that have been shown to be effective, has been conducted to develop an understanding of what are the asserted and evidence-based components of any mental health service that provides community care to people with severe mental health problems.
Method
Electronic databases (Medline, Psychinfo, OVID, Google scholar) were searched for articles with a primary focus on case management published since 1995. (The Cochrane Collaboration reviews had reviewed papers up until 1995). Search strings were ‘case management’, ‘psychiatry’, ‘mental illness’, ‘community mental health services’, ‘assertive community treatment’, ‘intensive case management’ and ‘outcomes’. Articles were limited to ‘randomized controlled trials / controlled trials’ and ‘reviews’. These limits detected two specific types of articles. First, those reporting on controlled trials of case management, which shall be referred to as ‘analytic’ studies. Second, reviews or commentaries that captured some of the discussion and controversy around case management. These articles shall be referred to as ‘descriptive’ articles. References of identified articles were hand-searched for evidence of papers missed by the computerized search. Exclusion criteria were a primary focus on substance use disorders, psychogeriatric populations and health economics.
Additional early articles on the establishment of community treatment teams were hand-selected to test the hypothesis that findings in favour of case management have weakened with recent research.
Experimental arms are reported in this paper using the exact terminology from each study.
Results
A total of 60 relevant papers were located with 39 papers identified as analytic and 21 as descriptive articles. Of the analytic articles almost half (17/39) reported on the outcomes of two large UK studies, 12 relating to the UK 700 study [12–23] and five to the PRiSM study [24–28]. Eight of the 21 descriptive articles related to the UK 700 or PRiSM studies [29–36]. The remaining 13 descriptive articles included meta-analyses, systematic reviews and non-systematic reviews [7–10, 37–45].
The controlled trials were a heterogenous group including comparisons of ACT, intensive case management (ICM) or other case management to ‘standard/usual care’ or another form of case management. Due to the heterogeneity of experimental types and results, we examined three different domains to determine patterns. We compared studies on the basis of the experimental group, year of study and outcome measure.
Experimental group
Experimental arms included ACT, ICM, generic case management, close supervision, outreach case management and strengths model. There were a small number of studies that focused on particular high-risk patient groups such as the homeless and those with low IQ.
A difficulty common to the present study and earlier research in the area is adequately differentiating ACT from ICM. ACT appears to be more widely used in US studies while ICM in more prominent in the UK [43]. ACT is more consistently defined than ICM, with an international consensus on essential features based on Stein and Test's model [33, 46]. Essential features are: caseloads of 8–12 patients, an integrated multidisciplinary team that shares caseloads, 24 h-a-day, 7-days-a-week availability, team autonomy, and part-time psychiatrist input.
ICM is also based on Stein and Test's Training in Community Living Model [47] but there is a less clear international consensus on defining features. ICM incorporates elements of ACT, such as small case loads, multidisciplinary teams and an assertive outreach approach. One distinction between ICM and ACT is that caseloads are shared in the latter. In a comprehensive review of case management styles this was the only feature that consistently distinguished ICM from ACT [38].
Assertive community treatment
Ten articles looked at ACT. The majority of these compared ACT to standard care [48–55], one compared ACT to hospital-based rehabilitation [56] and one, to a brokerage model [57].
Intensive case management
Seven separate studies on ICM were reported in a total of 15 articles. One compared ICM to a brokerage model [58] and the rest to either standard care or standard case management [12, 18–21, 23, 25–27, 47, 59–62].
Year
We arranged analytic articles chronologically according to the year in which the study began. Four studies are excluded from this analysis because the year the study commenced was unable to be determined [51, 54, 62, 63]. The Mowbray et al. 1997 article, reporting on a 1979 study comparing ACT to standard care, found strong benefits for the experimental group [50]. This prompted the inclusion of two further studies conducted at similar times, to look for changes over time [48, 49].
A definite trend is ascertainable, with the three studies conducted in the 1970s showing overwhelmingly positive findings for the experimental group over standard care. Studies conducted since then have had less favourable results with a mix of improvement in some domains and no significant change compared to control group in other domains.
Outcomes
A number of different outcome variables have been studied (Table 1). The four most commonly used outcome measures were number of hospital admissions, total days admitted, symptom reduction and quality of life (QOL). There was no consistent outcome in terms of number of admissions or total days admitted. Symptom reduction and QOL were either improved or no significant difference compared to control.
Outcomes of case management according to experimental group
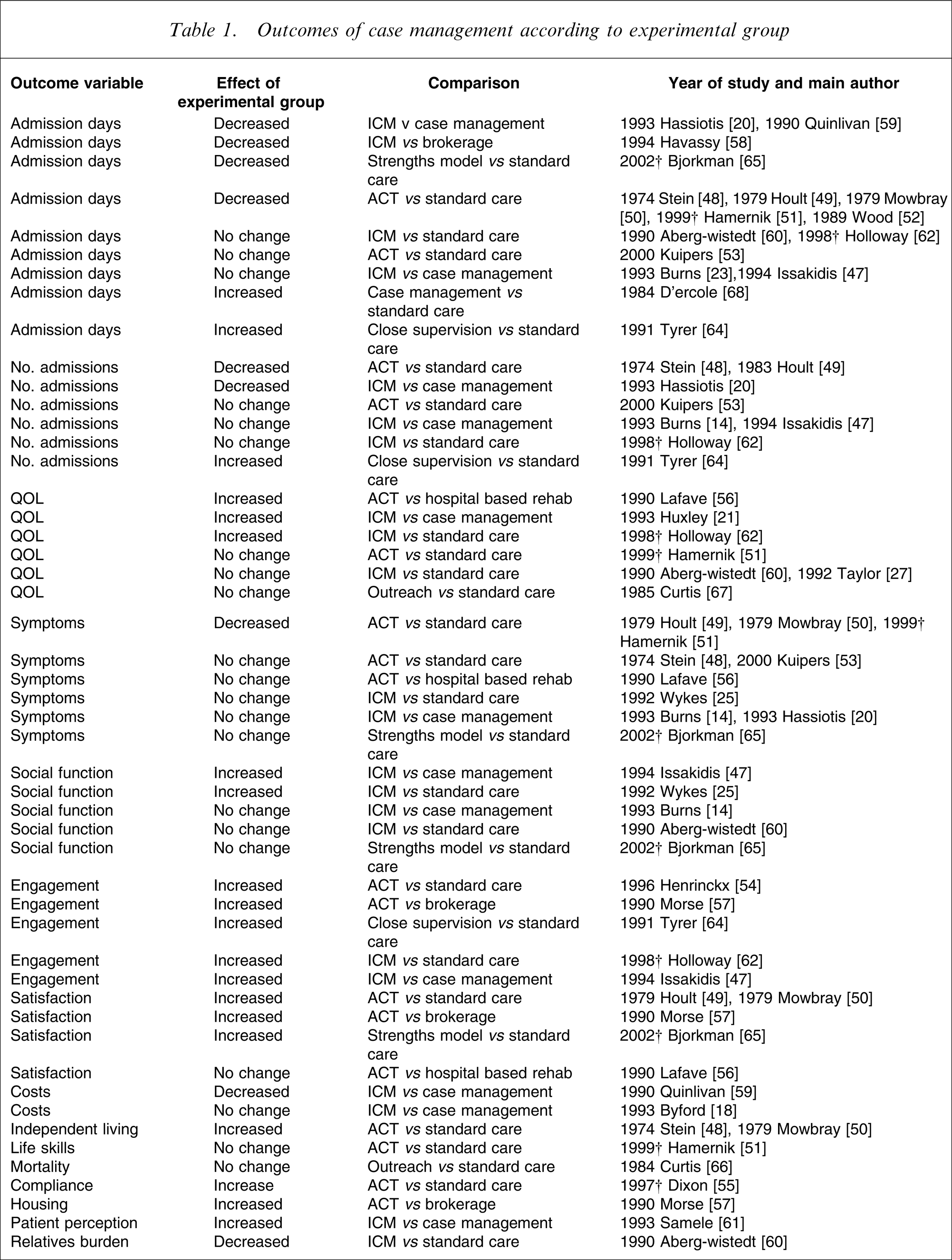
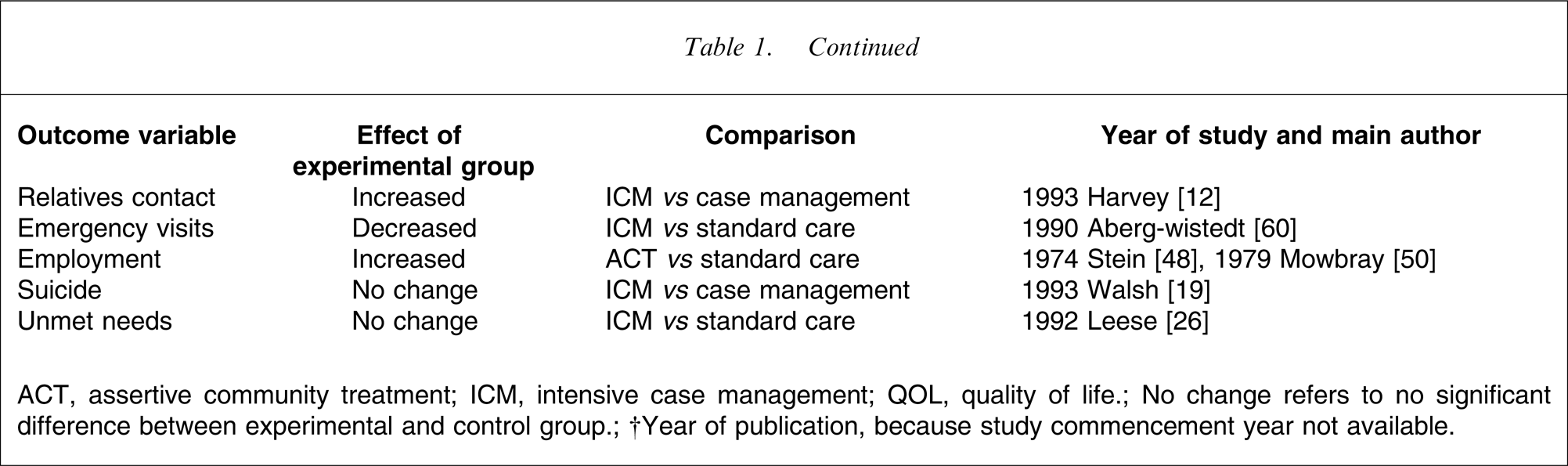
ACT, assertive community treatment; ICM, intensive case management; QOL, quality of life.
No change refers to no significant difference between experimental and control group.
†Year of publication, because study commencement year not available.
Few outcome measures were consistent in terms of direction of change across different studies. Outcomes that were consistently positive were in the domains of employment, engagement, independent living and carers burden/contact. However, the number of studies examining these outcomes was small, ranging from one to five.
Emergency room visits, housing, compliance and patient perception of treatment all improved in experimental arms, but each was reported only in single studies. Other outcomes reported only once included suicide, mortality and unmet needs, all of which were not significantly different between experimental and control groups.
Discussion
The findings of this review are consistent with previous reviews [8, 10, 38]. On balance, there is evidence that ACT is superior to standard case management, standard care and hospital-based rehabilitation on a number of domains. Results are not unanimous and factors contributing to this are worth closer examination.
Changes over time
The benefits of ACT over standard case management have diminished over time. Reasons for this have been postulated previously [43]. First, early studies compared ACT to standard care. Standard care has now developed to resemble case management and practices use in experimental arms by Stein and Test, and Hoult have now become the norm [40]. Second, the comparison groups have changed and are now more likely to be case management rather than standard care. Case management has evolved to incorporate elements of ACT such as significant home-based contacts [23] and frequent contact [60].
Definition of control/experimental groups
Poorly defined control groups complicate many of the identified studies, making it difficult to accurately determine how control and experimental groups differ. As a control group, case management is rarely described in terms of which model it is based on, for example strengths, rehabilitation, clinical case management or brokerage [38]. Even when the term ‘intensive case management’ is used there is variation in the intensity of services delivered and debate still reigns as to how intensive ‘intensive’ has to or should be [63]. The terms ‘ICM’ and ‘ACT’ at times appear to be used loosely and interchangeably and definitive factors differentiating ICM and ACT remain elusive [38]. The differences that exist between studies result in a heterogenous group limiting the conclusions of meta-analyses or systemic reviews.
Some studies have provided more extensive detail on the structure and content of the experimental arms and how they differ from the control group. This is particularly relevant to studies using terms such as ‘close supervision’ [64], which are not meaningful without a full explanation. For a number of studies the only significant difference between the arms was the size of caseloads [12–28, 47]. In these studies the two arms shared many features that originally defined ACT such as multidisciplinary teams and assertive outreach with home visits.
The UK 700 study received a great deal of criticism [29–32] regarding use of the term ‘intensive case management’. McGovern and Owen argue that the term ‘intensive case management’ is misleading because it lacked many of the expected components such as team approach, after-hours services, a psychiatrist on the team and lack of control over admissions, making it essentially a study on small case loads.
In this review only four separate studies investigated models other than ACT or ICM, one each on close supervision [64], strengths model [65], outreach case management [66, 67] and generic case management [68]. The small sample size prevents meaningful conclusions being drawn regarding these models. This is congruent with Mueser's review, which found little evidence for models other than ACT and ICM [38]. The question is raised as to why is there such a dearth of studies on models of case management, other than ACT/ICM, in recent years. It may now be widely accepted that standard case management does not produce substantial benefits for patients, hence it is no longer evaluated. Alternatively, it may be due to services having changed over the years to almost universally adopt case management as the usual model of care, making it redundant as an experimental arm.
Implementation issues
Numerous practical issues that influence the implementation of case management models in the real world setting may help explain the difficulty in replicating the definite benefits shown in initial studies of ACT. Early studies were conducted under strict research conditions with high fidelity to research models and large differences between the experimental group and standard treatment. Such high-fidelity research may not be carried out or practical in recent years [17].
Local resources, infrastructure, national policy and other systemic issues have very real interactions with how case management is practised [39, 46]. In particular, hospital admissions do not occur in a vacuum and may reflect access to beds or lack of other emergency accommodation. These factors are not constants and as policy and resources change, there will inevitably be an impact on case management both in clinical and research settings. The UK 700 study produced quite different results across its four subcentres due to local factors influencing implementation in different sites [22], and Thornicroft et al. acknowledge that service-wide and national influences confounded the PRiSM study [28].
Methodological flaws
The large UK 700 and PRiSM studies have drawn particular criticism regarding methodological flaws [29–32]. A number of common methodological flaws are repeated in numerous studies that may limit the validity of conclusions. First, robust findings may not be detected due to the studies being underpowered. The majority of studies in the present review did not present a power calculation. Kuipers et al. acknowledge that their study was underpowered to detect significant differences in bed days [53] and Holloway and Carson were not powered to detect change in depression and social behaviour [62]. Small numbers limit the validity and generalizability of the Hamernik and Pakenham, and Quinlivan et al. studies [51, 59]. Second, there are often significant attrition rates [53, 62]. Sashidharan et al. note only one-quarter of the eligible sample provided data in the PRiSM study [35]. Third, analyses were often not done on an intention-to-treat basis, with data only obtained from those still in contact at the end-point being included when comparing outcomes. Finally, raters were rarely blinded to the treatment arms. Although this may be necessary for clinical and staff safety reasons, it introduces a potential source of rater bias [19, 62].
The regularity with which poor methodology is seen reflects the small number of papers suitable for inclusion in rigorous meta-analyses. In the Simmonds et al. meta-analysis, 65 papers were identified yet only five met criteria for inclusion [40]. The Cochrane reviews included 10 out of 67 and 14 out of 75 identified papers for their case management and ACT reviews, respectively [5, 6].
Limitations
Limitations of our review include a search strategy that was limited to English-language articles and did not access unpublished papers. A number of studies were found reporting negative findings, reducing the potential bias caused by omitting unpublished studies, which may have a higher percentage of negative findings. The present article is purposefully a qualitative systematic review and was not designed as a meta-analysis. Studies were not weighted in any way and no statistical analysis was performed on results.
Conclusion
Case management is well and truly established as a major component of psychiatric treatment in most Western countries and has been for up to 20 years in some areas. Case-managed community treatment is widely accepted as the way forward and is preferable to hospital-based care [40]. Despite the widespread implementation of case management there remains vehement debate fuelled by contradictory findings, regarding the effectiveness of this type of treatment.
The question ‘Does case management work?’ is often heard but is too imprecise to be answered. Individual types of case management need to be studied separately to determine their benefits. In the present review, research on standard case management was scant. It is rarely studied as the active experimental arm and as a control arm it compares unfavourably with the ICM experimental group on admission days, number of admissions, QOL, engagement, social function and patient perception.
We were unable to clearly differentiate ACT and ICM so these are considered together. Assertive styles of intensive case management are effective in reducing the number of days spent in hospital, and improving engagement with services, compliance, independent living skills and patient satisfaction. There is poor evidence for its effectiveness in reducing number of admissions, symptoms, social function and quality of life. The present review suggests that ACT/ICM-style case management does not reduce suicide or mortality rates. Overall, ACT/ICM appears more effective than standard case management.
Quality community mental health care requires more than an effective configuration of services. We need to ensure that the content of the clinical interventions delivered to consumers include interventions with demonstrated effectiveness. The debate around how case management works is largely sterile if it is separated from the more important question of what clinical interventions work for a demonstrated illness and how to ensure that these interventions are delivered in an appropriate way to the individual patient.
Footnotes
Acknowledgements
This paper was funded by a grant from the Mental Health Branch of Department of Human Services, Victoria.