
Abstract
Keywords
The neurobiological basis of obsessive–compulsive disorder (OCD) has received much attention in the last decade, with many modalities of evidence suggestinga ‘neurological'basis for OCD [1]. The most significant evidence has come from functional imaging studies using positron emission tomography (PET) and single photon emission computed tomography (SPECT). Positron emission tomography studies of OCDusing 18F-fluorodeoxyglucose (FDG) [2–6] for metabolismor 15O for regional cerebral blood flow (rCBF) [7] have reported abnormalities in the orbito-frontal and cingulate regions of the cortex and the caudate nucleus, with increased metabolism or blood flow in the orbitofrontal regions being the most consistent finding. A rCBF study [7] reported a positive correlation between symptom intensity and blood flow in the right inferior frontal gyrus, caudate-putamen, globus pallidus and thalamus. These findings have led to neuroanatomical models of OCD [1], [8], in which the cortico-subcortical circuits principally involving the orbito-frontal cortex, caudate-putamen and the cingulate cortex are hyperactive.
The actual significance of these findings is debatable: are they responsible for the symptoms of the disorder, or are they epiphenomena, or in fact remote metabolic effects of abnormalities elsewhere? One method to examine their significance is to study the effect of treatment on these abnormalities and determine if clinical improvement results in normalization of PET findings. Studies of drug therapy have produced inconsistent results in this respect [3],[9],[10]. Neurosurgery offers an opportunity to test the models directly, especially because a few distinct lesions have been used in different centres to treat OCD [11],[12]. A single-case study, because of the ability to investigate the clinical and neuroimaging data in detail, is an appropriate design to achieve this.
We report the case of a woman with severe and intractable OCD who had a dramatic and sustained improvement after bilateral orbitomedial leucotomy and was investigated with FDG-PET before and after surgery.
Method
Case report
The patient was a 37-year-old woman who first consulted a psychiatrist for obsessions and compulsions at the age of 22 years and had her first hospitalization for the treatment at 26. Her illness was continuous over 15 years with minor fluctuations. The main symptoms were as follows: (i) intrusive thoughts that she might have put a lighted match into a petrol tank; (ii) thoughts that she might have kidnapped babies and left them on the railway line; (iii) thoughts that she might have sexually assaulted her young son or his friends; (iv) thoughts that her food might have been poisoned with kerosene or her own tablets; (v) counting rituals; and (vi) repeatedly cleaning all items in her cupboard and the bathroom.
She had become increasingly dependent upon her husband from whom she sought reassurances repeatedly. Her own life had become restricted to watching video-films for most of the day, not answering phone calls or the door, and eating one take-out meal a day after it had been ‘tasted’ by her husband. She had depressed mood which remained reactive, but was not judged to have a depressive disorder. She reported constant mild anxiety symptoms, and panic attacks occurred if she went out alone. Her total score on the Yale–Brown Obsessive– Compulsive Scale (Y-BOCS) [13] was 36. On the Leyton Obsessional Inventory [14], she scored 19/46 for symptoms and 7/23 for compulsive traits.
Noteworthy background history was of a violent alcoholic father who abused her sexually between the ages of 6–11, and a mother who was obsessionally tidy. She did not abuse alcohol or drugs, but smoked excessively.
Investigations including brain computerized tomographic (CT) and magnetic resonance imaging (MRI) scans and electroencephalograms were normal. A neuropsychological assessment revealed intellectual ability in the average range, normal performance on tests of frontalexecutive functioning, and mild psychomotor slowing possibly attributable to medication.
A range of drugs, two trials of cognitive–behavioural therapy, hypnotherapy and one attempt at psychodynamically oriented psychotherapy had been unsuccessful. Trials of drugs had included clomipramine (up to 300 mg/day), fluoxetine (up to 60 mg/day), sertraline (up to 100 mg/day), other tricyclic drugs (amitriptyline, imipramine and doxepin), monoamine oxidase inhibitors (phenelzine and moclobemide), and augmentation with trifluoperazine and benzodiazepines (oxazepam and diazepam). She had shown mild improvement with clomipramine and amitriptyline, but not to a sufficient degree to continue them beyond a few months.
After a case conference at the Neuropsychiatric Institute, she was recommended for neurosurgery, and approval for this was granted by the Psychosurgery Review Board of New South Wales, a statutory body responsible for approving all neurosurgery for psychiatric disorders in the State.
Operative procedure
Bilateral orbitomedial leucotomy [15] was performed under local anaesthesia and heavy sedation using MRI-guided stereotaxis. T1-weighted axial slices, 3 mm thick, with no gaps, were obtained parallel to the orbitomeatal plane. The target for the first lesion was identified as 6 mm above the gyrus rectus, on either side, and 1 cm anterior to the genu of the corpus callosum. Second lesions were placed 10 mm lateral to the first target points, and third lesions were 10 mm above the first. Radiofrequency thermocoagulation (60 s at 80°C) was used in order to achieve a lesion of about 8–10 mm diameter each. On postoperative MRI scans, the lesions were determined to be accurately placed in the orbito-frontal white matter. An axial MRI image through the lesions is presented in Figure 1. There were no intraoperative complications.
Two proton density brain MRI cuts (left transaxial, right coronal) from the patient imaged 2 weeks after the surgery demonstrating bilateral lesions (marked by arrows) in the white matter inferior to the frontal horns of the lateral ventricles and slightly lateral to them.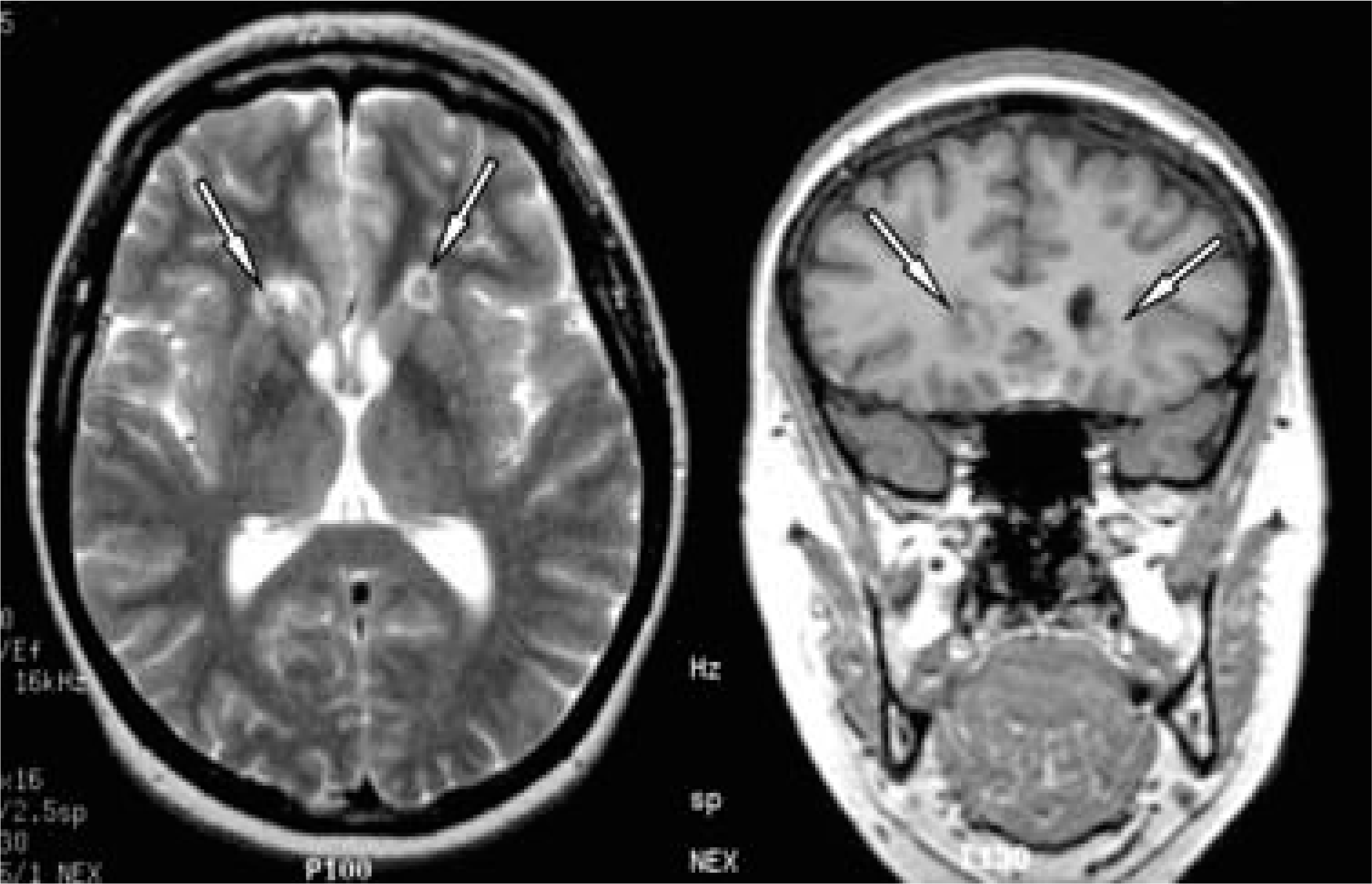
Positron emission tomography scan procedure and analysis
Scans were performed 2 days before surgery, and 18 days and 1 year postoperatively. The scans used between 400 and 450 MBqof 18F-deoxyglucose, and the patient's eyes were patched and ears plugged. Blood sampling was performed using the arterialized venous method. Region of interest analysis for cortical glucose utilization (mg glu/min/100 mL of tissue) was standardized to glucose utilization in the whole brain using the Statistical Parametric Mapping software (SPM version 1999b, The Wellcome Department of Cognitive Neurology, University College, London, UK). The normalized images can be interpreted as regional cerebral metabolic rate for glucose (rCMRglu) relative to the global level [16]. Scans two and three were spatially registered to scan one using the SPM software package and rigid-body (6 degrees of freedom) matching. The co-registered scans were then normalized on to the Talairach space. The anatomical regions of interest (ROIs) were manually traced on the reference T1-weighted MRI scan provided in the SPM package which is normalized onto Talairach space. In order to trace some of the ROIs, we re-adjusted the orientation of the MRI by rotating the whole image anticlockwise 30° around the anterior to posterior commisural plane. All three PET images were re-orientated in the same manner, the same traced ROIs applied to each PET image, and the mean, standard deviation, number of voxels of each VOI was measured. Percentage changes in relative metabolic rate from baseline were calculated for both the postoperative scans.
Results
Clinical
The patient was disoriented to time for 3 days after the surgery, but had no other complications. She spontaneously reported a marked reduction in her obsessions and urges and reduced anxiety 2 days after surgery when she was first able to be interviewed. Over thenext 4 weeks, she was engaged in a behaviour therapy programme, and in spite of needing frequent prompting and persuasion, she made significant gains. Upon her return home 1 month postsurgery, her obsessional thoughts had stopped almost completely, and she spontaneously discontinued the behaviour therapy. She reported some inappropriate jocularity, for example when visiting a relative whose husband had recently died, she felt like laughing, but this did not persistbeyond 2 months. All psychotropic drugs were discontinued after 1 month. At 2 months postsurgery, she was working 6 hours a day in a position which involved cooking and dispensing fuel. At the time of assessment at 1 year, she was free of obsessive–compulsive, anxiety or depressive symptoms, and described her treatment as ‘a miracle’. Her Y-BOCS score was zero, and on the Leyton Inventory she scored 3/46 on symptoms and 4/23 on traits. The adverse effects reported were: mild headaches intermittently for 5 months, increased intensity of smell for all odours but no olfactory hallucinations, and a gain of weightof 30 kg over 1 year, to some extent attributable to an increase in appetite and the resumption of a three-meals-a-day routine. Telephone contact in 1997, 3 years after the surgery, ascertained that she had maintained her recovery.
Repeat neuropsychological assessments were performedat 1 month and 1 year postsurgery. At 1 month postsurgery, the main finding was that her capacity for behavioural regulation was reduced, with a marked tendency to perseverate and to lose cognitive set. This impairment had resolved at the 1 year postsurgery assessment. Overall, there were no significant differences on measures of intelligence, language, visuospatial skills and most areas of frontalexecutive function. She performed better on verbal fluency. There was some increase in psychomotor speed, which probably reflected practice effects. Memory functioning was within the average range, but her capacity for new learning showed a marginal reduction from preoperative levels for both verbal and non-verbal material. Given the likely practice effects with readministration of tests, this may have represented a mild decline. The results of the tests are summarized in Table 1.
Neuropsychological test scores pre- and post-surgery and at 1 year follow up
Positron emission tomography scanning
Pre-operatively, no obvious abnormality was noted in the pattern of glucose metabolism. The second PET scan, performed 18 days after surgery showed a reduction of glucose metabolism in the head of the caudate (44%), anterior cingulate (26%), and orbital (20.5%), medial (17%) and lateral (15.5%) prefrontal cortices bilaterally and the thalamus (10%). In the third scan, a year later, the prefrontal relative metabolic rates had returned to baseline levels. Reduction in the caudate head (9.6%), anterior cingulate (15%) and the thalamus (11%) had persisted. The temporal lobes showed little change in rCMRglu, and the occipital and parietal lobes had an acute increase which persisted in the parietal lobes (12.5%) at 1 year. Representative transaxial slices at the same level from the three scans are presented in Figure 2, as are the subtraction images graphically representing the change from baseline. The mean values of rCMRglu corrected for whole brain values, are presented in Table 2.
The top panel contains representative transaxial slices at the same level from three 18FDG-PET scans from the patient performed preoperatively (a, scan 1) and 18 days postoperatively (b, scan 2) and 1 year postoperatively (c, scan 3). The scans were normalized to whole brain metabolic rate in each case. The bottom panel shows two subtraction images demonstrating change in metabolic rate postoperatively relative to the preoperative status: (d) scan 2 versus scan 1 and (e) scan 3 versus scan 1. Interested readers can contact the authors for a colour print of Figure 2.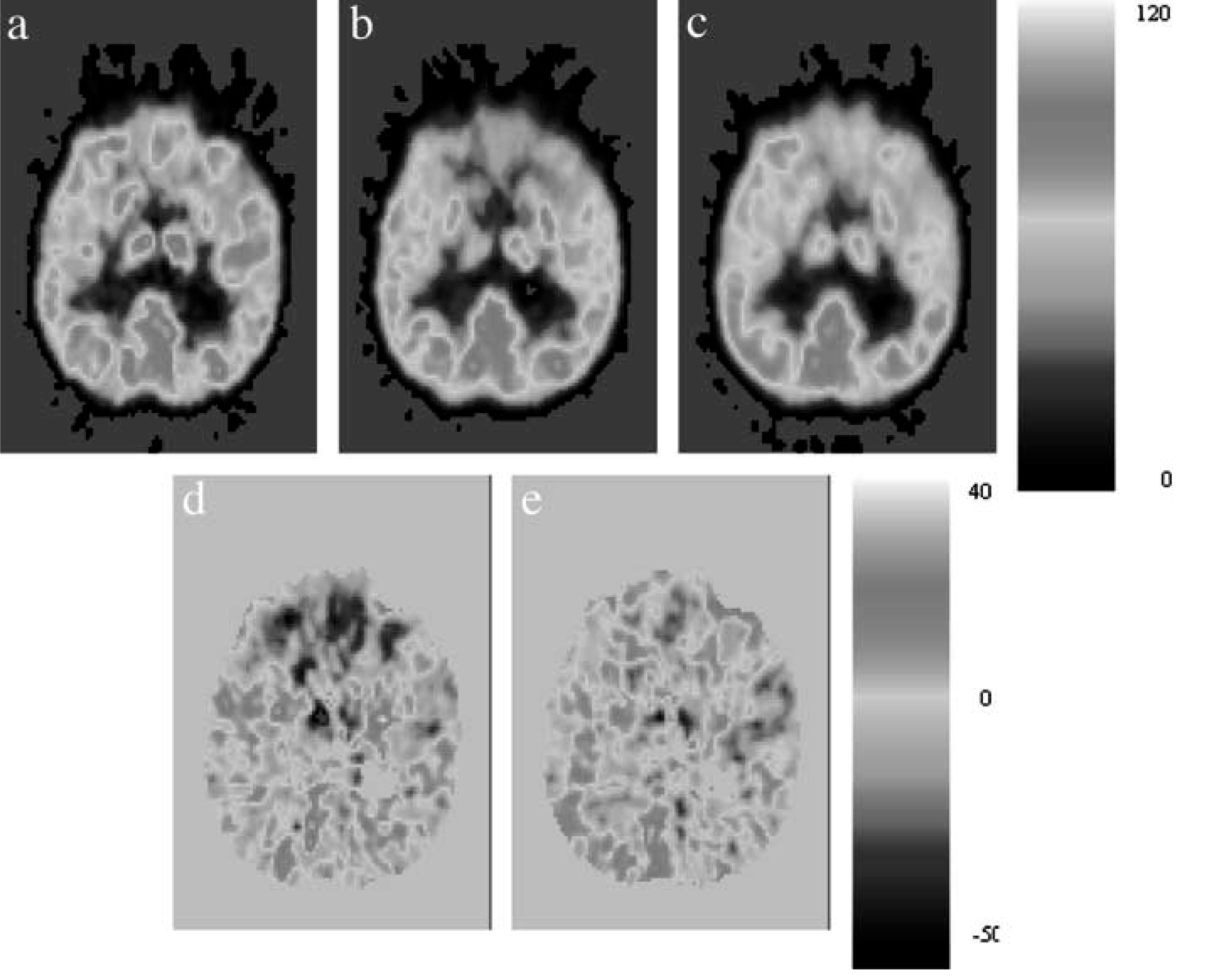
Relative values of regional cerebral metabolic rates for glucose corrected for whole brain metabolic rate using 18F-deoxyglucose positron emission tomography. Scan 1 was preoperative, Scan 2 was 18 days post-operative, and Scan 3 was 1 year later.
Discussion
This case is notable for the dramatic improvement in the patient with surgery, after previously having failed many efforts at treatment. While a placebo response cannot be dismissed in any single-case open design, it is extremely unlikely in this case given her previous non-responsiveness, the temporal relationship of the improvement with surgery and its persistence overthe 3 years of follow up. The improvement was in both her obsessions and compulsions, and while her anxiety levels improved as well, the effect of the surgery on her OCD should be considered to be primary. The improvement occurred without significant side-effects in the long term. Such a response, while unusual, is not unique in the neurosurgery literature [15],[17],[18].
The primary and prompt effect of surgery on her OCD permits speculation on the role of the lesioned pathways in the pathophysiology of OCD. Lesions were made bilaterally in the white matter connecting the orbitomedial prefrontal cortex to the subcortical structures, and possibly other cortical regions, in particular the pregenual cingulate gyrus. The striatum was not lesioned directly. The patient did not demonstrate an obvious increase in rCMR in the orbital cortex or caudate prior to the surgery. While not being congruent with the majority of the published reports that have dealt with groupdata [2–6], this preoperative status is consistent with the report by Mindus et al. [19] of five patients with severe and chronic OCD. The immediate post-surgical consequence was a reduction of metabolic rate in the caudate, the anterior cingulate, the prefrontal cortex and the thalamus. This is likely to be a consequence of the functional ‘disconnection’ between frontal corticalcortical and cortical-subcortical circuits produced by the structural lesion. The change in the prefrontal cortical metabolism may be due to altered feedback from subcortical structures, in particular the thalamus. From this study, it is not possible to say whether the neurosurgery has produced a normalization of previously abnormal metabolic rates, or has led to the development of hypometabolic regions. It could be argued that the maintenance of function at a lower level in some brain regions (caudate, anterior cingulate and thalamus) is necessary in a functionally abnormal OCD brain in order to produce a normal clinical phenotype.
The changes in orbital prefrontal cortex and caudate nuclei are similar to those reported by Mindus et al. [19] and are convergent with the effects of antiobsessional medication and behaviour therapy. Successful drugtreatment [9] and behaviour therapy [9],[20] have been shown to reduce metabolic activity in the orbital cortex and the caudate nucleus. Provocation of obsessive–compulsive symptoms while a patient is being scanned reveals an increase in activity in the orbito-frontal cortex [7],[21]. Lesions in orbitomedial cortex [22], anterior cingulate gyrus [18], medial thalamic nuclei [23] and the caudate nuclei [17] have all been associated with improvement in OCD. It is therefore difficult, and probably incorrect, to suggest that one brain region is abnormal in OCD, or that its amelioration depends upon changes in any one region. A more plausible interpretation is a dysfunction in a frontal-subcortical circuit lesioning which is likely to result in widespread effects. The persistence of reduced metabolism in the cingulate gyrus, head of caudate and thalamus in our patient is noteworthy, even when prefrontal cortical metabolic rates had returned to baseline levels. These rates suggest that the functional activity in the circuit continued at a lower level and this was associated with continuing remission of the OCD. In our patient, this was achieved with lesions bilaterally in the orbito-frontal white matter. A similar result is arguably possible by lesioning the thalamo-frontal fibres in the anterior capsule or by cingulotomy, operations that are known to help some OCD patients.
The surgery did not have significant long-term adverse effects on cognition in our patient. In the short term, she demonstrated some impairment in behavioural regulation, but this had resolved at the 1-year examination. There was a marginal reduction in her capacity for new learning, which may reflect some decline. However, overall there was little detrimental effect on cognitive function. This result is consistent with our previous report that surgery for OCD did not detrimentally affect measures of intelligence and memory [24] although disturbance in frontal-executive functioning has been reported by us [24] and some other investigators [17].
In conclusion, this case provides further support for the cortical-subcortical circuit model of OCD and that intervention on this circuit can be an effective treatment. The case also suggests that further studies of neurosurgical treatments of OCD should combine it with neuroimaging studies to achieve the goal of a rational approach to neurosurgery for psychiatricdisorders [25].
Footnotes
Acknowledgements
The authors are grateful to Wanda Schinke for manuscript preparation and the PET Centre at the Royal Prince Alfred Hospital for the PET scans.